
Abstract
Abstract
Background:
Laparoscopy for colorectal cancer treatment is widely accepted. However, there is no consensus as to whether or not laparoscopy can be considered the preferred treatment strategy in octogenarian and nonagenarian patients with colon cancer. The aim of this study was to compare operative and postoperative outcomes of laparoscopic right colectomy between oldest-old (≥80 years) and younger (<80 years) patients with colon cancer.
Methods:
The study population was sampled from the CLIMHET Study Group cohort. Between January 2005 and December 2015, data were retrieved for all patients who had undergone elective laparoscopic right colectomy for colon cancer in five University Hospital centers in France (CHU of Clermont-Ferrand, Hôpital Civil of Strasbourg—IRCAD, Hôpital Henri-Mondor of Créteil, Hôpital Européen Georges Pompidou of Paris, and CHRU of Tours).
Results:
Overall, 473 cancer patients were selected and analyzed. There were 156 oldest-old patients (median age: 84.1 years, range: 80–96) and 317 younger patients (median age: 67 years, range: 25–79). After adjusting based on propensity score on gender, obesity, American Society of Anesthesiologists score, smoking, arteriopathy, coronaropathy, comorbidity, and American Joint Committee on Cancer staging, no significant difference was found in operative and postoperative outcomes, except for time to resume a regular diet (3.6 days versus 3.0 days, P = .008) and length of hospital stay (12.1 days versus 9.1 days, P = .03), which were longer for oldest-old patients. Overall and disease-free survival rates were also equivalent between groups.
Conclusion:
These findings support that laparoscopic right colectomy can be safely performed in cancer patients aged 80 and older, and its outcomes are similar in oldest-old and younger patients.
Introduction
I
The proportion of oldest-old people has substantially increased over recent years worldwide, and this growth is expected to accelerate in the coming decades. In particular, the group of individuals aged 80 and older, namely the “oldest-old” people, is increasing even faster than the number of old persons overall, with a projection of 202 million oldest-old people in 2030 and 434 million ones in 2050.5,6 Consequently, an increasing number of individuals aged 80 and older are diagnosed with cancer and non-cancer pathologies, requiring surgical treatments every year, 7 and an increasing number of surgical operations are performed in octogenarian and nonagenarian patients. However, an advanced age is associated with a higher American Society of Anesthesiologists (ASA) score, a higher cardiac and pulmonary comorbidity rate, a poorer nutritional status, and a reduced physiological reserve to cope with major surgery.8–10
Several studies have reported the benefits of laparoscopic colorectal surgery compared to open surgery in elderly patients,11–16 with recent reports describing good outcomes in octogenarians17–19 and in very old patients with colorectal cancer. 20 However, despite a growing body of evidence supporting that laparoscopic outcomes in elderly patients with colorectal cancer are similar to those observed in younger patients, 21 further studies are required to establish the optimal care strategy for the oldest-old population.22–24
Because laparoscopy requires the induction of a pneumoperitoneum and often longer operative times, laparoscopic colorectal resection is not always recommended for oldest-old patients, 25 and the feasibility and safety of the whole procedure should be carefully considered. 26 In particular, the patient's general status and performance, the underlying pathology (e.g., malignant or benign), and the type of surgical procedure required (e.g., right or left colectomy) are the main factors to be taken into consideration before performing laparoscopic surgery in oldest-old patients.
This study aimed to describe the operative and postoperative outcomes of laparoscopic right colectomy performed in octogenarian and nonagenarian patients with colon cancer. To assess the feasibility and safety of laparoscopy, the outcomes observed in the oldest-old group (≥80 years old) were compared with those observed in younger patients (<80 years old) undergoing laparoscopic right colectomy for the same indication.
Materials and Methods
The study population was retrieved from the CLIMHET Study Group database, which includes patients undergoing laparoscopic right colectomy between January 2005 and December 2015 in five University Hospital centers in France (CHU of Clermont-Ferrand, Hôpital Civil of Strasbourg—IRCAD, Hôpital Henri-Mondor of Créteil, Hôpital Européen Georges Pompidou of Paris, and CHRU of Tours). Data were extracted from a retrospective database concerning exclusively the laparoscopic approach in right colectomies for benign and malignant pathologies. The study was conducted in accordance with the ethical principles ascertained in the Declaration of Helsinki.
For these analyses, we selected all patients who underwent an elective laparoscopic right colectomy for histologically proven colon cancer located in the ascending colon (from the ileocecal valve to the right colonic flexure). Patients with synchronous colon cancers, metastatic disease, locally advanced cancer requiring multivisceral resections, or who underwent reoperations for tumor recurrence were excluded. Based upon the patient's age at the time of surgery, the study population was divided into two groups: the oldest-old group (including patients aged 80 or older) and the younger group (including patients aged 79 or less).
Perioperative antiembolic stockings were applied for deep vein thrombosis prophylaxis. Laparoscopic right colectomies were performed as previously reported using a medial-to-lateral approach for radical operations.27–30 The ileocolic anastomosis was performed either intracorporeally or extracorporeally. 31 Conversion was defined as the completion of the right colectomy procedure through either an enlarged incision or an abdominal incision of ≥6 cm.
The following variables were analyzed: age, gender, body mass index (BMI), obesity (BMI >30), ASA score, smoking, diabetes, arteriopathy, coronaropathy, previous laparotomy, previous laparoscopy, comorbidity score in elderly patients (as described by Covinsky et al. 32 ), American Joint Committee on Cancer (AJCC) staging, lesion localization (e.g., cecum, ascending colon, right colonic flexure ( = hepatic flexure), and ileocecal valve), operative time, conversion rate, anastomotic characteristics (e.g., manual and extracorporeal), perioperative antibiotics, perioperative transfusion, and perioperative intravenous fluids. Postoperative morbidity and mortality were defined as events occurring during hospital stay or within 90 days after resection. Postoperative complications were categorized according to the Dindo–Clavien classification. 33 Surgical complications included prolonged ileus (>5 days with nasogastric tube), anastomotic leakage, anastomotic hemorrhage, wound infection, intra-abdominal abscess, bleeding, and evisceration. Nonsurgical complications included cardiac, vascular, and pulmonary ones. All complications were assessed by a clinician and were prospectively registered into databases at discharge or during the first outpatient visit. Postoperative outcomes included the following: reoperation rate, time to resume a regular diet, time before ambulation, time to flatus, time to the first stools, time before cessation of intravenous fluids l, intensive care unit (ICU) stay, length of hospital stay, and number of lymph nodes harvested.
Statistical analysis
For descriptive statistics, continuous variables are presented as median (range) and categorical variables as numbers and percentages. For bivariate two-sided comparisons between oldest-old and younger groups, a Mann–Whitney U test, a chi-squared test, or a Fisher's exact test was used. Binary, multimodal, and linear regression analyses were performed to control the effects of covariates on operative and postoperative outcomes, including, in the multivariate analysis, those variables that reached a significant P value in the univariate analyses. In addition, a multivariate analysis of demographic, clinical, and pathological variables was used to identify independent factors associated with the incidence of postoperative complications. Overall survival (OS) and disease-free survival (DFS) rates were computed using the Kaplan-Meier method and compared between groups using the log rank (Mantel–Cox) test. A P value <.05 was considered significant. Statistics were performed using the R software (version 3.2.0, R Core Team, R Foundation for Statistical Computing, Vienna, Austria).
Results
Out of a total of 637 patients of the CLIMHET Study Group database, 473 patients were selected and included in these analyses. All patients underwent an elective laparoscopic right colectomy for colon cancer. Demographic and clinical characteristics are reported in Table 1. The oldest-old groups presented with a lower proportion of male patients (45.5% versus 57.1%, P = .01), a higher ASA score (P = .0002), fewer smoking patients (5.1% versus 16.7%, P = .0002), and more arteriopathy and coronaropathy compared to the younger patients' group. Comorbidity score and AJCC staging were also significantly different between the two groups.
Values shown in bold denote a statistically significant value.
AJCC, American Joint Committee for Cancer; ASA, American Society of Anesthesiologists; BMI, body mass index.
Operative variables are outlined in Table 2. Both groups had similar operative times. No significant difference was found in the conversion rate and in the technical details of the surgical procedure, such as ileocolic anastomosis, perioperative antibiotics, transfusion, and administration of intravenous fluids. No significant difference was found when adjusting the P value for gender, obesity, ASA score, smoking, arteriopathy, coronaropathy, comorbidity score, and AJCC staging.
Adjusted for gender, obesity, ASA score, smoking, arteriopathy, coronaropathy, comorbidity score, and AJCC staging.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiologists.
Postoperative outcomes are displayed in Table 3. Surgical complication rates were not different between the two groups (28.2% for oldest-old patients versus 20.8% for younger patients, P = .08). The most common complication in both groups was prolonged ileus (8.3% for the oldest-old group and 7.3% for the younger group). A significant difference was found in the incidence of nonsurgical complications, with a greater incidence of cardiac, vascular, and pulmonary complications in the oldest-old group (14.7% versus 7.6%, P = .02). However, this difference was no longer significant in the preoperative risk-adjusted analysis. The younger patients' group showed a shorter time to resume a regular diet (3.0 days versus 3.6 days, P = .007), a reduced time to first flatus (3.0 days versus 3.3 days, P = .02), and a reduced time before cessation of intravenous fluids (5.5 days versus 6.1 days, P = .004) compared to the oldest-old group. In addition, a shorter ICU stay (0.62 days versus 1.2 days, P = .04) and a shorter hospital stay (9.1 days versus 12.1 days, P = .0001) were observed in younger patients compared to oldest-old ones. However, only the time to resume a regular diet and the length of hospital stay remained significantly different in favor of the younger patients group in preoperative risk-adjusted analysis. A trend toward statistical significance was noted for the Dindo–Clavien classification of postoperative complications (P = .06). However, no group difference was noted when adjusting for covariates. The 90-day mortality and the number of lymph nodes harvested were also similar between groups.
Values shown in bold denote a statiscially significant value.
Adjusted for gender, obesity, ASA score, smoking, arteriopathy, coronaropathy, comorbidity score, and AJCC staging.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiologists.
Results of the univariate and multivariate analyses of factors associated with the incidence of postoperative surgical and nonsurgical complications are shown in Table 4. Diabetes, arteriopathy, operative times longer than 240 minutes, and transfusion were significantly associated with the incidence of postoperative surgical complications. Multivariate logistic regression analysis showed that all these factors were significant predictors of the incidence of postoperative surgical complications. Coronaropathy, comorbidity score, and AJCC staging were significantly associated with postoperative nonsurgical complications. On the contrary, the oldest age did not appear as an independent prognostic factor associated with postoperative surgical or nonsurgical complication.
Values shown in bold denote a significant result.
AJCC, American Joint Committee on Cancer; BMI, body mass index; CI, confidence interval.
Median follow-up time for the whole study population was 36 months (range: 1–121). OS and DFS are displayed in Figures 1 and 2. OS of the oldest-old group was comparable to the one of the younger patients' group. Survival rates were as follows: 98% at 1 year, 95% at 3 years in the oldest-old group versus 97% at 1 year, and 93% at 3 years in the younger patients' group (P = .15), respectively. DFS rates were as follows: 94% at 1 year, 89% at 3 years in the oldest-old group versus 96% at 1 year, and 92% at 3 years in the younger patients' group (P = .29), respectively.
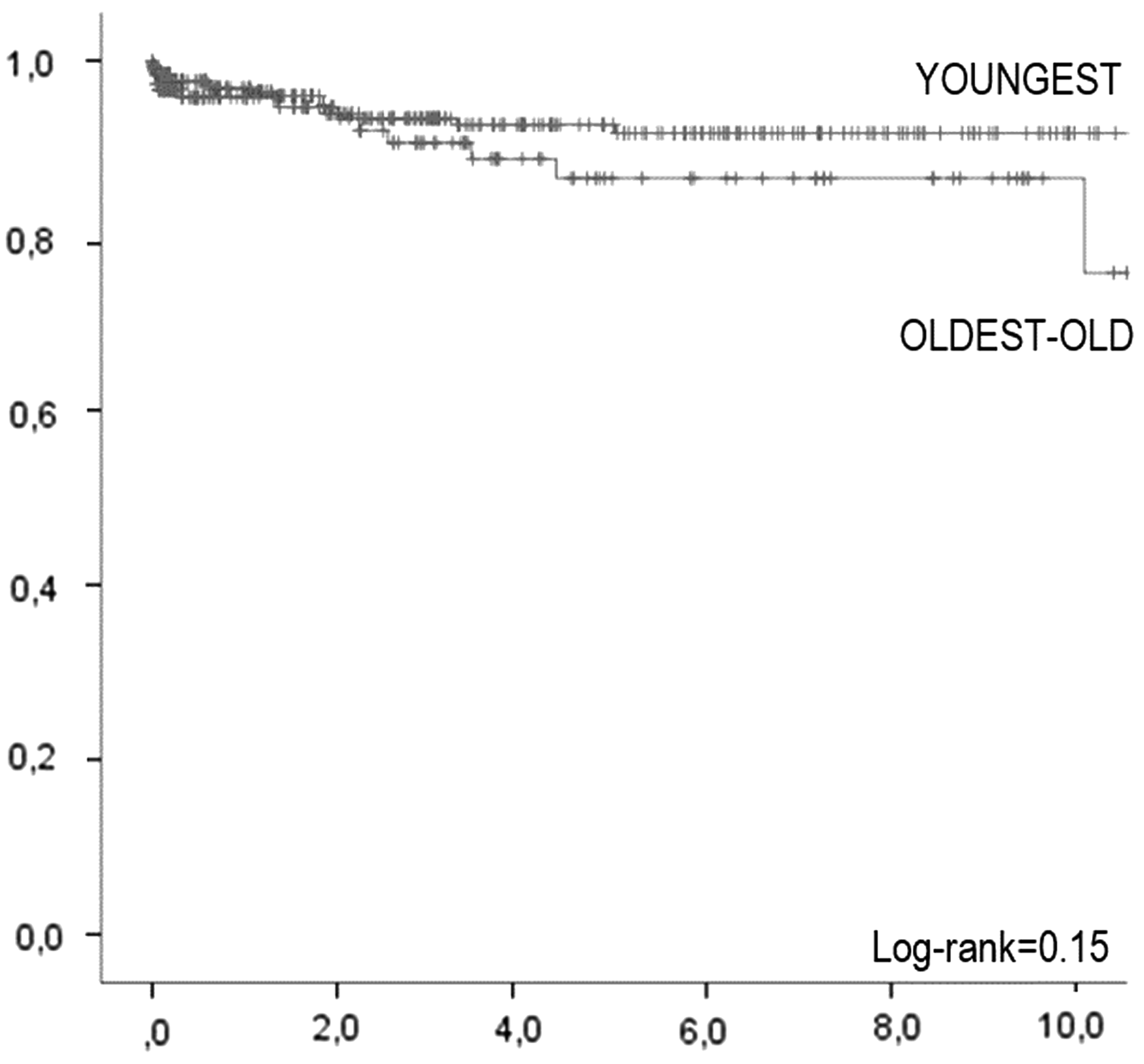
Overall survival.

Disease-free survival.
Discussion
In a large cohort of patients with colon cancer, this study shows that laparoscopic right colectomy can be safely performed in oldest-old patients as in younger ones. Operative and postoperative variables are comparable between the two groups of age, although time to resume regular diet and length of hospital stay are longer in the oldest-old patients' group. However, being octogenarian or nonagenarian does not appear to be a predictor of postoperative surgical and nonsurgical complications.
Nowadays, laparoscopic surgery is considered the gold standard approach for colon cancers and it is also gaining widespread application for rectal cancers.34–37 However, in elderly patients, laparoscopy is still a matter of controversy, 38 and several studies indicated that an increasing age is an independent predictor of increased surgical mortality,39–43 whereas other studies supported that age per se has a minimal effect on surgical morbidity and mortality risks.20,26,39–42,44
Due to the global aging process and particularly to the fact that people aged 80 and older are growing faster than any younger segment of the population, abdominal surgeons deal with oldest-old patients almost everyday. 5 Octogenarian and nonagenarian patients undergo an increasing number of surgical operations performed every year,7,26,45 and they represent a surgical challenge because of the association with multiple comorbidities and with reduced physiological reserves and tolerance to stress.26,38,43 In addition, the use of laparoscopy has been associated with the risk of adverse hemodynamic effects related to pneumoperitoneum induction in patients with limited cardiopulmonary reserve. At present, this drawback seems to be limited. Recent studies observed an improved OS in elderly patients operated on with laparoscopy as opposed to open surgery,46,47 and the possibility to work with low intra-abdominal pressures may contribute to minimize this risk. 38
This study confirms that the oldest-old population is more vulnerable than younger patients, presenting with a higher comorbidity score and particularly with more cardiovascular pathologies (e.g., arteriopathy and coronaropathy). However, the operative outcomes of laparoscopic right colectomy are not different between groups, supporting the feasibility and safety of laparoscopy even in octogenarian and nonagenarian patients. Of note, the conversion rate was similar in both age groups and no conversion to open surgery was required due to anesthesia problems related to the pneumoperitoneum.
Overall postoperative morbidity, including surgical and nonsurgical complications, and 90-day mortality were equivalent between the oldest-old patients' group and the younger patients' group when adjusting for gender, obesity, ASA score, smoking, AJCC staging, and comorbidities. Independent predictors significantly associated with postoperative surgical complications were as follows: diabetes, arteriopathy, operative time ≥240 minutes, and perioperative blood transfusion. For nonsurgical complications, the significant predictors were as follows: coronaropathy, high comorbidity score, and advanced AJCC staging. These predictors were already observed in previous studies,9,20,45,48,49 while age was not significantly associated with postoperative morbidity. 48 This highlights the critical concept that the age factor cannot be simply considered the chronological age of the patient, rather, it should include the complete evaluation of the patient's physical, mental, and functional health to assess the related risk for postoperative adverse events. Similarly, the age threshold to define the elderly population has been a matter of debate and has been progressively increased over the last decades.19,39,43,49–55 In this study, we decided to evaluate the feasibility and safety of laparoscopic right colectomy in oldest-old patients, a specific age category, which necessarily emerged from the global increase in life expectancy. As observed in other studies conducted in elderly populations (75 years and older),20,48,49 also in this study, the quality of the aging process (e.g., presence of comorbidity), rather than the chronological age of the patient, appears to be the critical factor predicting surgical outcomes.
With respect to short-term postoperative outcomes, the oldest-old patients' group showed significantly longer times to resume a regular diet and a longer length of hospital stay compared to the younger patients' group. These longer times may result from a slower return to gastrointestinal functions, a more intense postoperative pain and fatigue, and a lower physical reserve, which can be expected in octogenarian and nonagenarian patients. Conversely, long-term outcomes showed similar overall and DFS rates.
This study has strengths and limitations. The study population is a homogeneous cohort of patients operated on for colon cancer using laparoscopic right colectomy only. This is rarely found in the literature where most studies evaluated colon and rectal cancer together, which, however, require different treatments (e.g., chemoradiotherapy) and surgical interventions. Notwithstanding, caution should be taken to interpret and generalize these findings. The CLIMHET database involved five University Hospitals and included patients who underwent a laparoscopic right colectomy only. No comparative evaluation with open surgery for colon cancer in oldest-old patients could be performed. In addition, due to the long time interval considered, the impact of therapeutic protocols, such as adjuvant chemotherapy, could not be assessed and selection bias cannot be ruled out. All surgeons involved in the study were highly experienced in laparoscopic surgery, and for every patient, indication for surgery was determined after discussion in multidisciplinary meetings. As a result, operative and postoperative outcomes cannot be directly generalized to low-volume, nontertiary, or nonuniversity centers. Further studies should be conducted to assess the impact of specific therapeutic protocols in combination with laparoscopic colectomy in the specific subset of elderly patients.
Conclusion
Laparoscopic right colectomy can be safely performed in oldest-old patients with colon cancer with operative outcomes that are comparable to those observed in younger patients. Postoperatively, the oldest-old patients' group recovers more slowly than the younger patients' group. However, age per se does not appear to be a significant predictor of postoperative surgical and nonsurgical complications. Nevertheless, the presence of comorbidities, especially cardiovascular ones, and their severity impact on postoperative outcomes should be attentively evaluated preoperatively to assess the patient's risk.
Footnotes
Disclosure Statement
No competing financial interest exists.