
Abstract
Abstract
Background:
Experimental study to evaluate feasibility of continuous intraoperative neural monitoring (C-IONM) in transoral endoscopic thyroidectomy vestibular approach (TOETVA).
Methods:
Duroc–Landrace pigs were orally intubated with electromyogram endotracheal tube. Automatic periodic stimulation (APS) electrode was allocated in the operative field through the 5-mm ports. APS was then repose on vagal nerve (VN) with different approaches: (1) median, that is, between sternothyroid and thyroid gland; and (2) lateral, that is, between sternocleidomastoid and sternothyroid. VN was stimulated proximally and distally to the APS location to verify whether the dissection and/or placement determined VN injury. Video presentation is offered.
Results:
Assembled APS accessory was feasible in large-brained animals. The two basic options for VN approaches were tested. Baseline obtained had amplitude values >1000 μV, bilaterally.
Conclusions:
C-IONM was feasible in TOETVA in porcine models, but simplification of electrode design and application is needed.
Introduction
Continuous intraoperative neural monitoring (C-IONM) is an endorsed technology to perceive imminent nerve lesions and to end the associated surgical maneuver and impede permanent recurrent laryngeal nerve (RLN) injury in thyroid surgery. 1 C-IONM contributes continuous RLN function report, which is useful in complex procedures especially as in endoscopic and robotic thyroidectomy. 2 C-IONM overcomes the limit of intermittent application (I-IONM), that is, RLN at risk of injury between or proximally to the stimulation sites.1–3
With numerous institutions beginning to perform transoral endoscopic thyroidectomy vestibular approach (TOETVA), there is an accretion concern in novel accessories that may early advise for RLN stress.4–7
A recent article reports on C-IONM feasibility in transoral endoscopic procedures in humans. 8
It is identically necessary that the safeness of an original technology and related procedure is verified before it is generally applied on patients.
The purpose of this translational study was to evaluate the feasibility of C-IONM application in TOETVA and describe a step-by-step procedure in a porcine model.
Materials and Methods
Animal breeds
Protocol was approved by local Animal Care of Jilin University (China). Two Duroc–Landrace piglets (25 kg) (n = 4 RLN, n = 4 vagal nerves or VNs) underwent general anesthesia via i.v. thiopental 15 mg/kg administration and oral intubation performed via size number 7ID EMG (electromyogram) endotracheal tubes (TriVantage; Medtronic, Jacksonville, FL) to explore the application of C-IONM. Anesthesia was maintained with sevoflurane 1% to 2% and cardiopulmonary monitoring was performed. EMG parameters, including threshold, latency, amplitude, and evoked potentials in swine, are similar to humans.9–14
Monitoring equipment and setup
The monitor (NIM-Response 3.0 System; Medtronic) was set with a response threshold to identify small response at 150 μV, stimulation rejection artifact at 2.6 ms, and rectangular pulsate-negative stimulus of 100 μs duration at 4 Hz. Proper EMG tube position was verified by laryngoscope and obtaining first VN V1 stimulation value and\or baseline >500 μV.1,2,11 Single-use, incrementing Prass stimulating probe, monopolar, standard flexible tip (product n.8225490; Medtronic), was inserted transcutaneously, midline for complementary intermittent IONM. IONM was offered analogous to standards by the International Neural Monitoring Study Group.11,12
TOETVA and C-IONM procedure
TOETVA procedure has been previously described.5–7 C-IONM was delivered by the automatic periodic stimulation (APS; Medtronic) accessory. The APS electrode was wet before to facilitate its sliding into the 5-mm ports. The outer black clip of the APS electrode was carefully removed. After the creation of the working space,5–7 the probe was allocated in the operative field through the left 5-mm port (Fig. 1). The side of the ports is determined by the dominant side of thyroid disease. The port was then removed by sliding the wire inside until the end and then restored and reinserted. Therefore, the wire of the APS remained between the port and the vestibule. In this way, there was no interference and displacement with the introduction of the endoscopic instruments in the port.
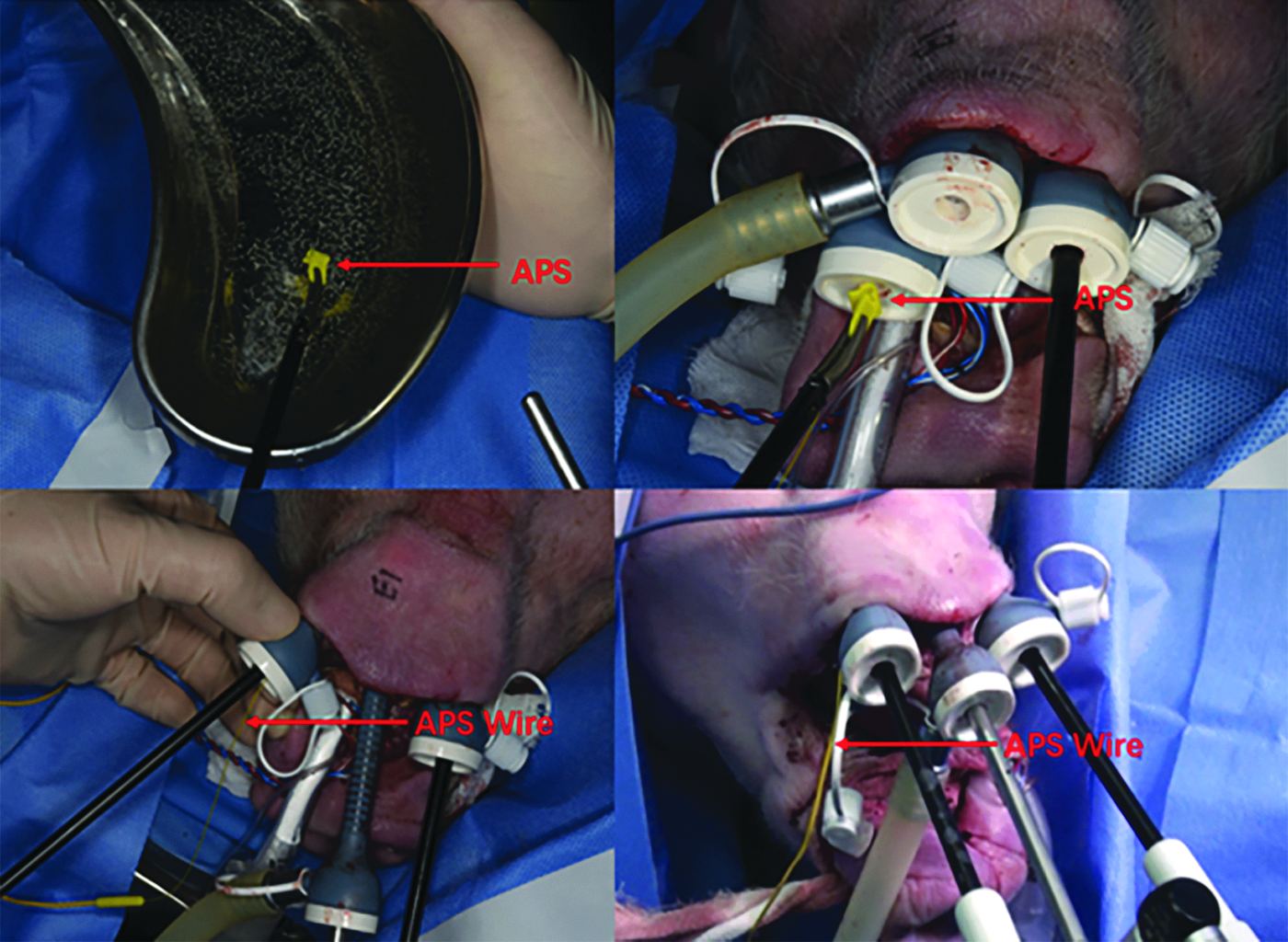
The APS accessory is wet before to facilitate its sliding into the left 5-mm port. Also, the outer black clip is carefully removed. The APS electrode is placed through the left 5-mm port. The port is then removed by sliding the wire inside until the end and then restored. Therefore, the wire of the APS remains between the port and the vestibule. In this way, there is no interference with the introduction of the endoscopic instruments in the port. The side of the port is determined by the dominant side of thyroid disease. APS, automatic periodic stimulation.
We evaluated two different approaches to the VN, bilaterally and in both pigs.
Median, that is, in between the sternothyroid and thyroid gland (Fig. 2a, b).
Lateral, that is, between the sternocleidomastoid and sternothyroid (Fig. 3a, b).
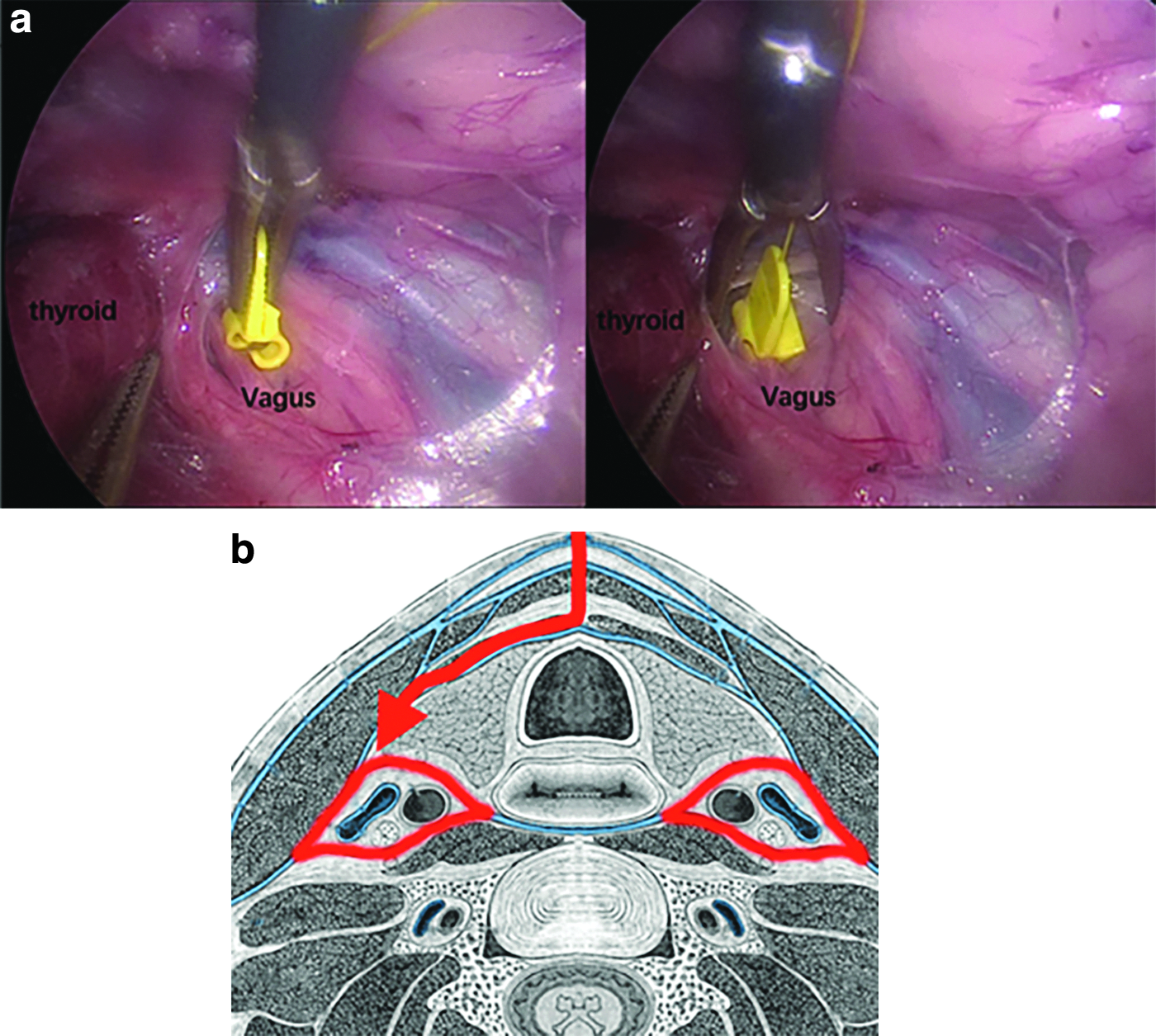
The anterior median approach (i.e., between sternothyroid and thyroid gland). The APS is positioned gently on the VN after opening the carotid sheet by a 2-cm pouch. Careful 360° dissection of the VN with Maryland forceps is required. To prevent VN thermal injuries, energy-based devices are avoided. Intraoperative view
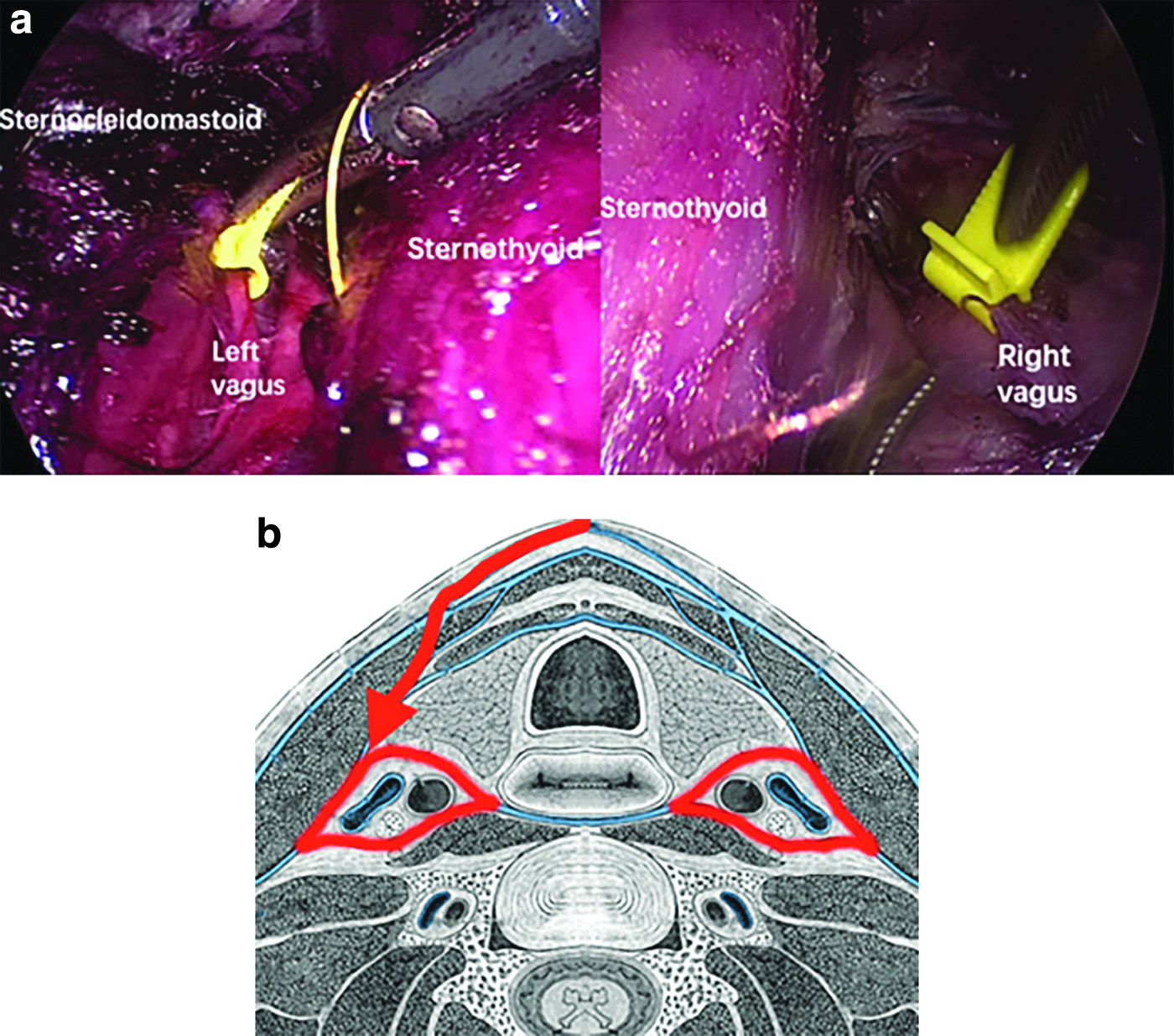
The modified anterolateral approach to the vagal nerve (i.e., between the sternocleidomastoid and sternothyroid). Intraoperative view
The APS was positioned gently on the VN after opening the carotid sheet by a 2-cm pouch. Careful 360° dissection of the VN with Maryland forceps is required. To prevent VN thermal injuries, energy-based devices were avoided. The APS electrodes were then reposed gently on the VN. During VN dissection and after the C-IONM electrode was placed, the VN was stimulated repeatedly by means of the intermittent stimulating probe, proximally and distally to the location of APS, to verify whether the dissection or electrode placement determined VN injury. After connecting the APS electrode with the monitor system, baselines for the latency and amplitude were graded. Stimulation frequency for C-IONM was set for every second, thus evaluating the RLN and VN constantly. To ensure that the APS probe wire was devoid of or interfered with the endoscopic view, the APS electrode wires were anchored on the platysma with two stitches from external to internal (Fig. 4). During the experiment, EMG signals were recorded steadily. An upper limit threshold for the latency (+10%) and a lower limit threshold for amplitude (−50%) were used as alarm lines.1,2 In addition, acoustic and optical signals alerted the surgeon when a preset threshold had been crossed or when the electrode had become dislodged. Removal of APS was performed by gently opening and pulling out the pins. Protocol included multiple sequences and test for APS positioning, with different APS sizes (2 and 3 mm) in distinct VN cervical locations. The TOETVA procedure was done under an operating 30° endoscope.
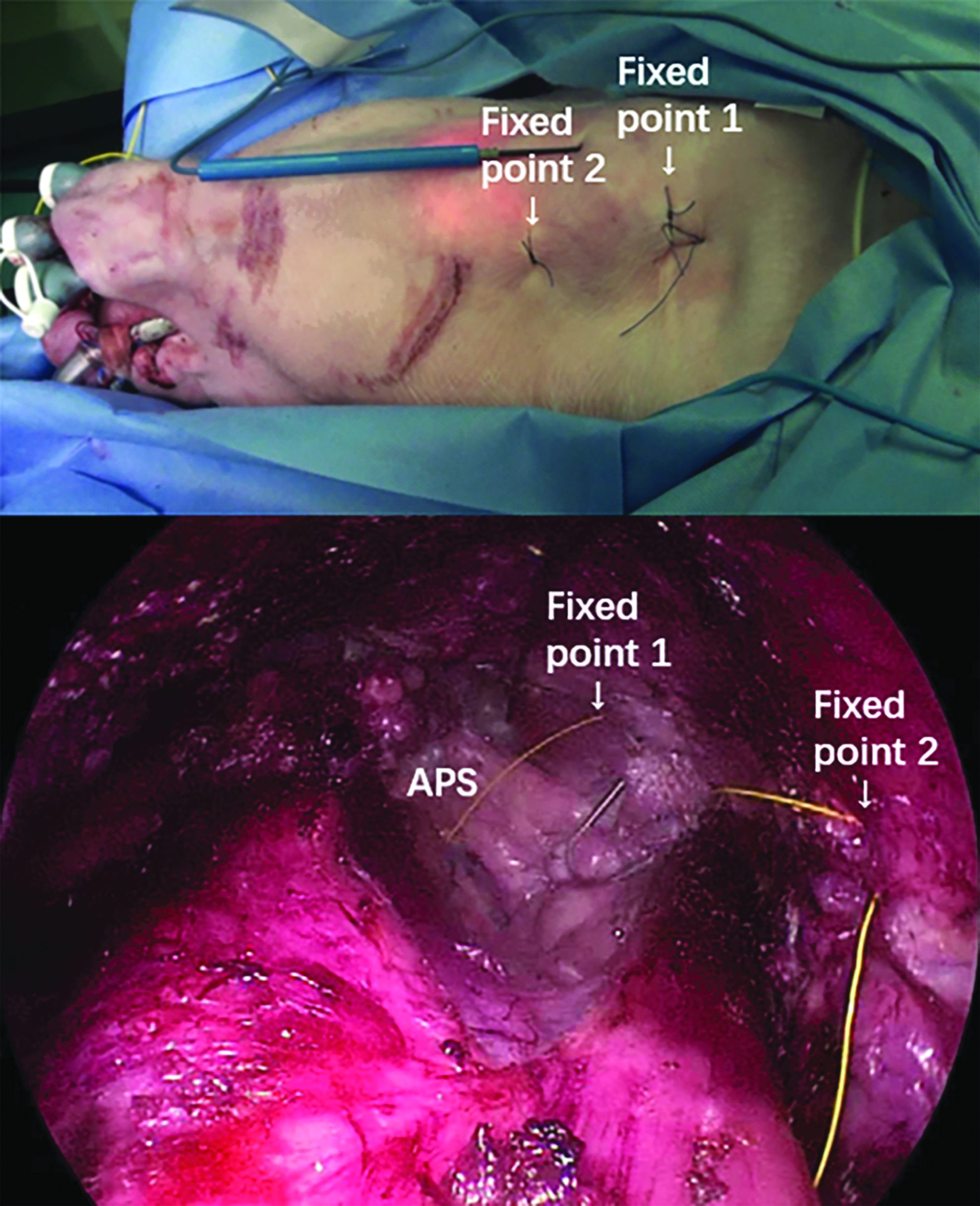
The APS electrode wires were fixed on the platysma with two external to internal stitches to prevent wire endoscopic view inference during transoral endoscopic thyroidectomy vestibular approach. APS, automatic periodic stimulation.
Results
Intermittent monitoring and normative EMG data
The VNs and the RLNs were identified and stimulated in all procedures bilaterally. We achieved the IONM intermittent standardized technique with V1, R1, R2, V2 determinations: the mean ± standard deviation (SD) response amplitudes were 1950 ± 279 μV for V1 and 2036 ± 549 μV for R1. Mean response amplitudes of R2 and V2 were 1966 ± 521 μV and 2092 ± 676 μV, respectively.
APS implanting
Supplementary Video S1 of the experimental surgical procedure is available (please note that the TOETVA surgery shown in this video is for APS positioning and C-IONM demonstration purposes only). Assembled continuous monitoring with APC accessory was feasible in large-brained animals. Surgical approach and APS electrode placement last between 15 and 37 minutes operative time. The two basic options for VN approaches were successfully tested. The lateral approach to the VN was more demanding, because of the required muscular dissection. The mean ± SD were 18.5 ± 8 minutes for medial approach and 27 ± 7 minutes for lateral approach. No major vascular injuries occurred. VN 360° dissection was achieved without injury confirmed by proximal stimulation (Supplementary Video S1). APS flexible wire produced no interference with the endoscopic instrumentations and view. There were no broken accessories.
Amplitude baselines
Baselines obtained had amplitude values >1000 μV, bilaterally, in both pigs. The mean ± SD response amplitudes were 1950 ± 279 μV.
Signal stability
The EMG signals were stable. Nerves showed unchanged EMG signals after complete APS positioning and thyroidectomy. The mean ± SD response amplitudes were 1920 ± 279 μV for V1 and 2044 ± 249 μV for R1. Mean response amplitudes of R2 and V2 were 2066 ± 121 μV and 1922 ± 216 μV, respectively. C-IONM was performed successfully without any adverse combined event of decreased amplitude or increased latency in both the pig models: there was no significant difference in RLN and VN latency (increase) and amplitude (decrease) with procedure. No APS accessory displacement occurred during animal thyroidectomy. C-IONM use was not associated with any cardiovascular sequelae. There were no problems with APS removal from the VN and the surgical field.
Discussion
Witzel and Benhidjeb 15 first tested the feasibility of intermittent monitoring for the RLN in a porcine model in TOETVA, in 2009. Authors proved IONM to be a performable procedure in living swine with a long stimulating probe. The RLNs were identified visually and then confirmed with IONM at the beginning (R1) and at the end of the bilateral procedures (R2). 15
Chen et al. 8 described foremost the use of C-IONM in 20 TOETVAs (i.e., 28 nerves at risk). C-IONM was achieved using a C2 monitor and delta stimulating electrode (Inomed, Freiburg, Germany). The flexible stimulating electrode was trans-vestibular inserted, with its cable wire lying outside one trocar. 8 The VN was anatomized, looped, and then covered by the probe. Alarms were set when the EMG amplitude reduced by 50% and latency prolonged by 10%. 8 The stimulation was set at 0.7 mA every 1 second. C-IONM procedures were successfully completed. No adverse neural, cardiovascular, or gastrointestinal sequelae happened. The ipsilateral C-IONM procedure required a mean of 10.33 minutes. There was one instance of probe displacement in this series. One combined EMG event manifested, which improved after releasing the retractor on the gland. This patient had no RLN paralysis postoperatively. 8
Here, we described the implantation of APS in a porcine model. Each step of the VN preparation, probe insertion, and monitoring is illustrated so that the end surgeon can replicate the process. The experimental study and video confirmed the technical feasibility of C-IONM on the performance of TOETVA with APS accessory in pig model. Obtained baselines were >1000 μV, to test the quality of APS positioning and recording.
Supplementary Video S1 illustrates the implantation procedure and critical steps to ensure quality EMG recordings.
Although technically realizable, we here below introduce some important issues to thoughtfully consider translating the obtained results in humans.
Simplification of C-IONM electrode design and application is advisable in the near future for TOETVA due to the following reasons. (1) Instances of equipment interference with the other endoscopic instruments, in particular with the flexible wire in the surgical field. (2) Nevertheless, it is advisable once inserted, not to pull out of the vestibule the flexible wire, as it is time-consuming to reinsert. (3) C-IONM location requires an additional 360° dissection of the VN.16,17 All C-IONM technologies available need to dissect the VN by 360° to accommodate the electrode on the nerve. This procedure can be challenging endoscopically, time-consuming, or even harmful to the nerve and vessels while positioning the accessory and at removal of the electrode.
Furthermore, C-IONM accessory should be versatile because the location of the VN in relation to the common carotid artery and internal jugular vein in humans is variable.18,19 Moreover, carotid arteries kinking is frequent with advancing age.18,19
Table 1 summarizes the features of C-IONM electrodes available currently for thyroid surgery; none of these seem to be easy to apply in TOETVA. Special care should be taken while handling the APS probe and preparing the VN surface for implantation.
Continuous Intraoperative Neural Monitoring Electrodes Available for Thyroidectomy
None of these seems to be easy to apply in TOETVA. Simplification of electrode design, geometry, and application on the VN is advisable in the near future.
APS, automatic periodic stimulation; EC, European community; TOETVA, transoral endoscopic thyroidectomy vestibular approach; VN, vagal nerve.
Percutaneous and transcutaneous C-IONM has been described recently and appears to be promising for endoscopic and robotic thyroidectomy. 20
Footnotes
Acknowledgment
The present study was financially supported by Jilin provincial special fund for healthcare (Grant Nos. SCZSY201714 and SCZSY201504).
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Authors' Contributions
Conception and design: H.S. and G.D.; administrative support: G.D.; collection and assembly of data: H.S., G.D., and D.Z.; data analysis and interpretation: H.S., G.D., and D.Z.; article writing: all authors; and final approval of article: all authors.
Disclosure Statement
D.Z., S.L., G.D., T.W., J.Z., G.X., and H.S. have no conflict of interest to disclose, and no other funding or financial relationship with the surgical industry.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.