
Abstract
Abstract
Introduction:
This case highlights the successful utilization of a multidisciplinary approach to numerous bilateral bronchopleural fistulae (BPF) using minimally invasive techniques. In this study, we present a previously healthy 14-year-old male hospitalized with 2009 H1N1 influenza and methicillin-resistant Staphylococcus aureus coinfection complicated by severe acute respiratory distress syndrome and multifocal necrotizing pneumonia, with significant lung tissue damage requiring prolonged extracorporeal membrane oxygenation (ECMO) support.
Methods:
The development of multiple BPFs precluded lung recruitment necessary to wean from ECMO. Treatment options were very limited and endobronchial valves were considered. However, localizing single airleaks with a fogarty balloon is normally the technique to determine appropriate location to place the valves. With multiple fistulae, this technique would be ineffective. Therefore, the patient was brought to interventional radiology and bronchography was performed for selective fistula mapping. With this precise localization, the multiple fistulae were ultimately controlled using image-guided embolization and the placement of multiple endobronchial valves. The success of this intervention enabled positive pressure ventilator support and rehabilitation required for weaning from ECMO support.
Conclusion:
This case highlights the successful utilization of a multidisciplinary approach to numerous bilateral BPFs using minimally invasive techniques.
Introduction
D
Recently, there has been reported success with the use of selective endobronchial valves in BPF that are refractory to other interventions. 7 Initially developed for adults with emphysema, their efficacy is based on their ability to prevent air trapping and facilitate mucus removal.8,9 The alternative to noninvasive management is mainly surgical intervention, which may necessitate native lung tissue resection. While numerous adult studies exist, there is a paucity of data focusing on pediatric BPF management. A study performed by Toth et al. demonstrated successful utilization of endobronchial valves in pediatric patients with persistent BPF. 10 Their study demonstrated the first successful utilization of endobronchial valves in the pediatric population, obviating the need for surgical intervention. Despite their success, the use of selective endobronchial valves has not been demonstrated in the scenario of multiple bilateral BPF.
In this study, we report a 14-year-old previously healthy male with severe pediatric acute respiratory distress syndrome (ARDS) secondary to 2009 H1N1 influenza and methicillin-resistant Staphylococcus aureus (MRSA) coinfection, complicated by necrotizing pneumonia requiring a prolonged 88-day extracorporeal membrane oxygenation (ECMO) course. After the development of multiple, bilateral BPF, a minimally invasive approach was instituted, which ultimately allowed for successful ECMO weaning and eventual discharge home. This case highlights two important points. First, with multiple fistulae, the traditional workflow of implementing endobronchial valves was not successful, highlighting the need for contrast bronchographic mapping for valve deployment. Second, there was successful resolution of a difficult clinical scenario in which BPF were preventing lung recruitment maneuvers vital to weaning from ECMO. This case demonstrates a successful utilization of resources from a number of subspecialities, ultimately resulting in a successful outcome.
Case Presentation
This is the case of a previously healthy 14-year-old male who presented to the hospital in septic shock secondary to H1N1 influenza and MRSA coinfection with resulting pediatric ARDS and bilateral necrotizing pneumonia requiring maximum ventilator support. The patient's cardiopulmonary status declined requiring cannulation onto venoarterial ECMO. The patient's respiratory status continued to decline and on day 15 of ECMO, he developed bilateral tension pneumothoraces requiring emergent bilateral chest thoracostomy tube insertion. The patient's clinical status remained tenuous with the development of a subsequent left-sided bronchopleural fistula as evidenced by persistent air leak from his left-sided chest tube. See Figure 1 for timeline.
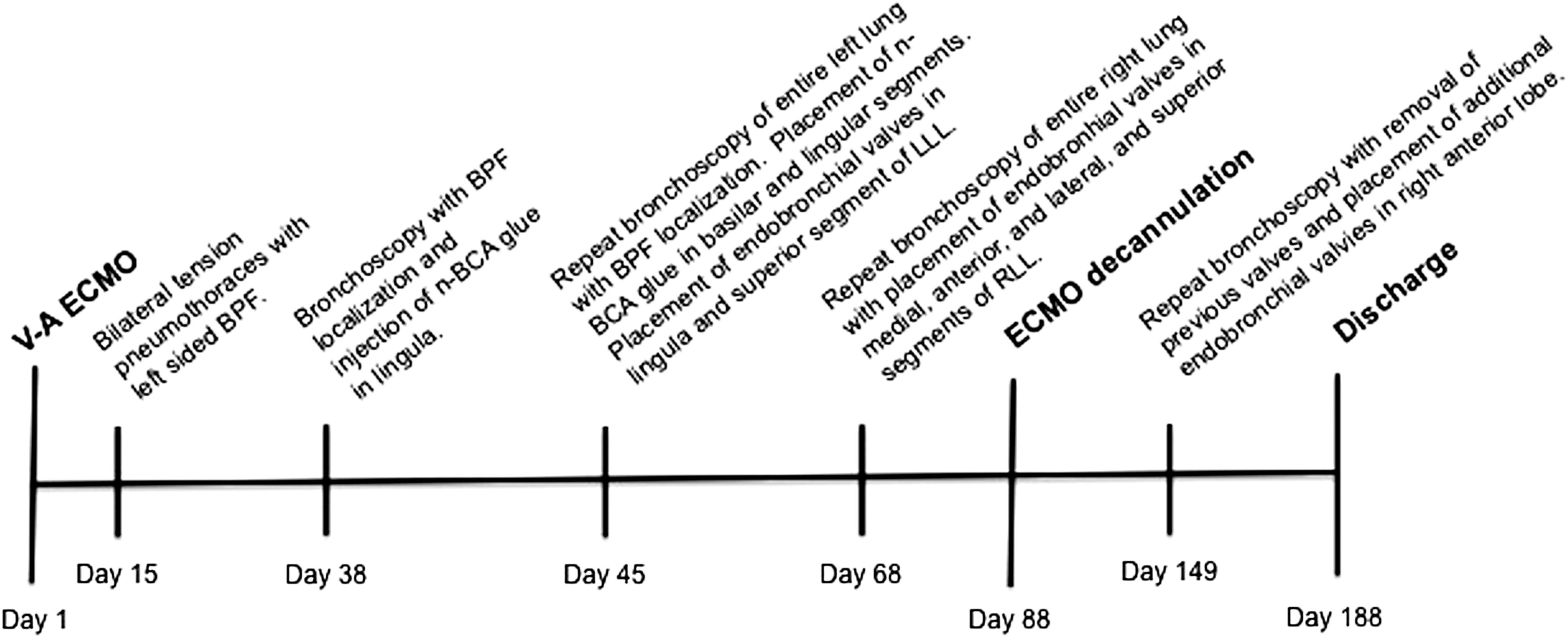
This demonstrates the timeline of events starting from the initiation of ECMO to discharge. ECMO, extracorporeal membrane oxygenation.
In an attempt to localize the fistula and improve lung recruitment, he was taken to the operating room for bronchoscopy using a flexible bronchoscope (Olympus Scientific, Tokyo, Japan). Once in the left bronchial tree, a 4F Kumpe catheter (Cook Medical, Bloomington, IN) was advanced through the bronchoscope. A 0.035 glidewire (Terumo, Tokyo, Japan) was used to selectively advance the catheter into each bronchial segment. Visipaque (GE Healthcare) was injected in each segment, allowing for the visualization of the bronchi under fluoroscopy. Contrast leaking from the bronchial tree into the pleural space indicated the presence of a bronchopleural fistula. This demonstrated BPF in subsegmental bronchi of the lingula. Once the fistulae were identified, the catheter was prepped with dextrose solution. This allowed for hand injection of N-butyl cyanoacrylate (n-BCA glue) in a 2:1 mixture with ethiadol to occlude the fistulae as distally as possible. Despite successful closure of the fistula tract, his respiratory status continued to decline with persistent air leaking from his left-sided thoracostomy tube. This made any attempt for lung recruitment impossible and prevented weaning off ECMO.
After 4 weeks of attempted lung rest and ECMO support, the patient continued to fail attempts to wean off ECMO. Therefore, further minimally invasive interventions were undertaken. Additional surgical interventions were still felt to not be feasible, as the bleeding risk on ECMO is significant and the risk of causing additional injury would be substantial. Furthermore, with the findings of a chest computed tomography scan (CT), the amount of viable functioning lung was minimal and any loss of normal lung parenchyma was thought to endanger chances of weaning off ECMO. Endobronchial valves were considered as a potential solution to the patient's problem, but techniques to determine proper placement of these valves require cessation of air leaks from the chest tube when inflating a fogarty balloon at the suspected pulmonary segment. If the airleak stops. then the correct segment has been localized and the valve is deployed. However, with the multiple fistula present, this technique was not feasible. Therefore, the patient was taken back to the operating room where once again, a flexible bronchoscope (Olympus Scientific) was used to visualize the bronchial segments. Contrast bronchography was again performed and this allowed for precise mapping of the extensive BPF. At this point, there were fistulae identified in subsegmental branches of the superior and basilar segments in the left lower lobe (LLL), and multiple fistulae were seen within the lingula (Fig. 2). The previously occluded subsegments in the lingula remained occluded. The concern at this point was that the fistula in the superior segment was too central for n-BCA glue embolization due to the possibility of proximal spill and occlusion of large central bronchi blocking off a significant amount of functioning lung tissue. For this reason, the superior segment was not embolized with glue. The additional subsegmental fistulae in the basiliar and lingular segments were embolized successfully using n-BCA. To address the remaining fistulae, the adult pulmonology team was consulted for endobronchial valve placement. Given the previous mapping and fistula occlusion, accurate placement of the valves was possible. Using a flexible bronchoscope (Olympus Scientific), a 7 mm Spiration® (Seattle, WA) valve was placed into the lingular bronchus, and a 7 mm Spiration (Seattle) valve was placed into the superior segment of the LLL. Of note, the use of the valves was through an Investigational Device Exemption (IDE) for compassionate use for unapproved devices, as this device is not FDA approved in children. Later on, the patient was once again taken to the operating room for a persistent BPF from the right lung as evidenced by leaking in his right-sided thoracostomy tube. He was noted to have BPF in his right lower lobar segments, prompting the placement of 4 additional 7 mm Spiration (Seattle) endobronchial valves in the medial, anterior, lateral, and superior bronchial segments. The air leak had significantly decreased at the conclusion of the procedure. After control of the multiple BPF, proper lung recruitment could be enabled. Finally, on day 88 of ECMO, the patient was successfully trialed off ECMO and subsequently decannulated.
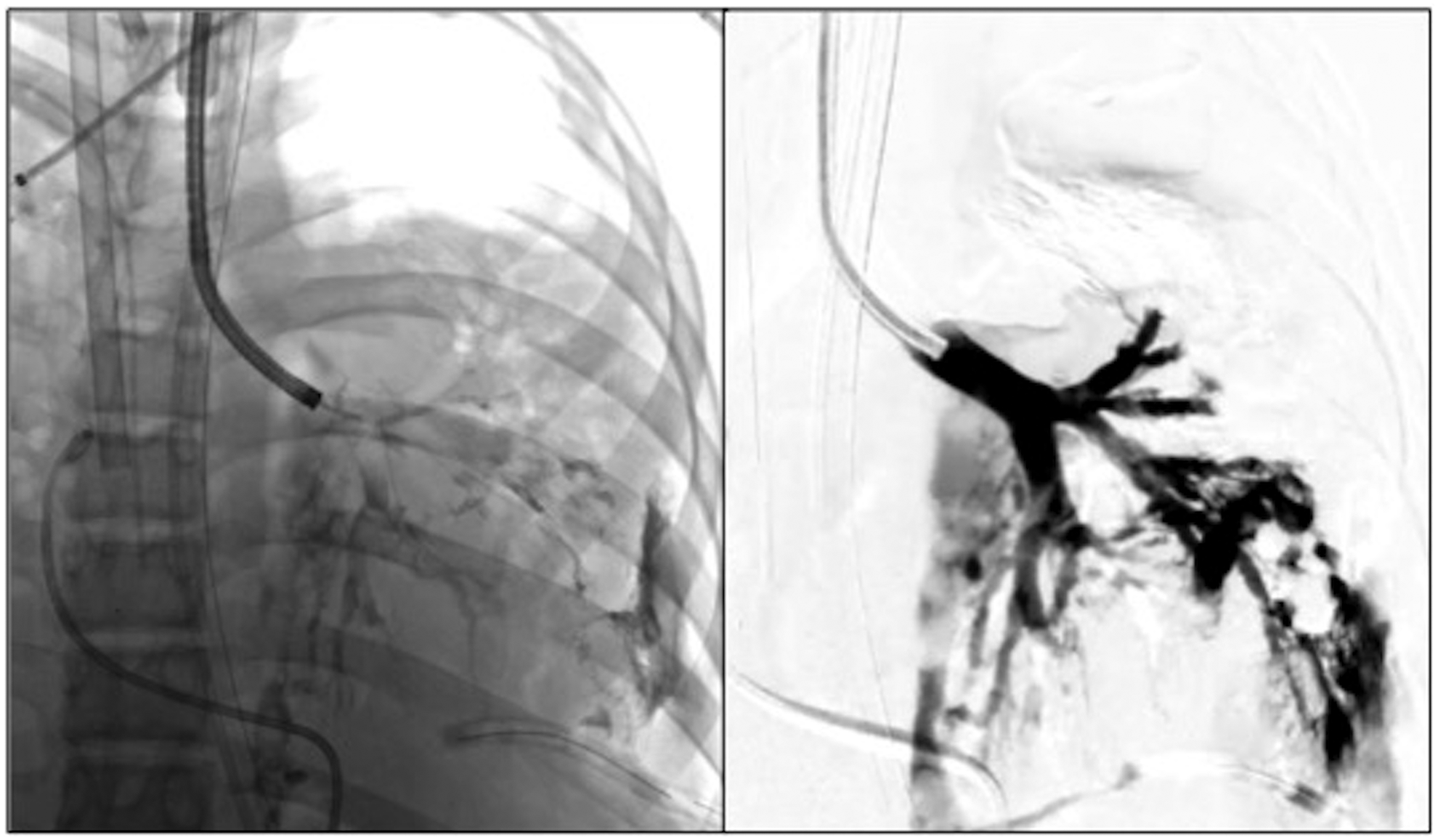
This demonstrates fluoroscopic images during the bronchography with contrast extravasation from the left lower lobe and lingula. The image on the left represents the flexible bronchoscopy with catheter going through the bronchoscope. The image on the right represents use of the DSA technique for visualization. DSA, digital subtraction angiography.
The patient did well over the next few weeks, but had increased respiratory symptoms leading to the diagnosis of a large right-sided pneumatocele requiring image-guided drainage catheter placement. Due to persistent air leaking after this, he was taken again to the operation room and was noted to have multiple right-sided BPF in the right upper lobe anterior segment with placement of both 7 and 6 mm Spiration endobronchial valves, and removal of previous valves. He continued to improve from a respiratory standpoint throughout his prolonged hospitalization. The patient was discharged with a Heimlich valve and continued requiring continued mechanical ventilation, which was successfully weaned over time to supplemental oxygen. He is now on room air, off mechanical ventilation, and the tracheostomy tube has been removed.
Discussion
BPF remain a significant problem in patients with severe pulmonary disease.10,11 Due to the poor respiratory status and associated comorbidities in patients with BPF, minimally invasive techniques are utilized as alternatives to surgical intervention. These techniques mainly focus on attempts to either control or selectively occlude BPF. Multiple treatments are available, including prolonged thoracostomy tubes, pleurodesis, endoscopic interventions, and surgery. Endoscopic approaches with fibrin glue, gel-foam, coils, stents, and endobronchial valves have been utilized with success.12–15 Our patient presented a unique and complicated scenario making him a poor surgical candidate and a challenge for any additional intervention and limited options. This case report demonstrates the successful deployment of multidisciplinary expertise and resources, including interventional radiology, pulmonology, critical care, and pediatric surgery to manage multiple bilateral BPF and allow for weaning from ECMO and improved respiratory function.
One of the definitive treatments of BPF is surgical debridement and closure, which consists of many techniques, including manual bronchial stump closure, native lung resection, and omental/muscle flap placement, among others. 16 These operations can be debilitating, and tend to provide benefit in the event of a single fistula or multiple fistulae in the same location. In our case, the possible loss of lung tissue would have been unsustainable. Surgical intervention also carries with it a significant risk of bleeding. This risk, in addition to the bleeding risk posed in patients on ECMO overall, made surgical intervention less desirable. Our patient had multiple comorbid conditions, including ongoing MRSA pneumonia, and ARDS with prolonged ECMO support. ECMO support alone provided an increased risk of bleeding with any surgical intervention, not to mention the added friability to tissue that may propagate further injury. 17 Additionally, there was the inability to perform basic physical conditioning maneuvers required to optimize lung recruitment maneuvers.
Endoscopic approaches have been utilized as an alternative to surgery. 18 One of the interventions utilized in this case is embolization of the fistula tract with n-BCA and/or fibrin glue. Using fibrin glue or n-BCA has demonstrated success in the closure of BPF, and is a well-documented approach to recurrent air leaks. 19 Unfortunately, in the event of centrally located BPF, complete occlusion to bronchial segments can be the risk of main bronchial occlusion. There were multiple fistulae in our patient that were centrally located, making complete occlusion of these multiple BPF unfeasible. In this regard, the decision to pursue a different approach was deemed necessary for survival.
Endobronchial one-way valves function by selectively occluding distal airway flow while facilitating the removal of trapped air and mucus.7,20,21 They were initially introduced for lung volume reduction surgery in patients with severe emphysema, but have also been utilized to control recurrent BPF. 20 They have been shown to be effective surgical alternatives, as demonstrated in a study by Travaline et al., who reported complete resolution of air leak in 48% of patients and a significant reduction in air leak in 45% of patients. 10 The only study of pediatric patients enrolled candidates after all other noninvasive options had been exhausted and surgery was the next step. All patients had a range of one to four endobronchial valves placed and demonstrated successful resolution of air leak after an average of 12 days. There is very limited data on the use of endobronchial valves on ECMO. The clinical data exist only in adult case reports, specifically one by Hodges et al. and the other by Brichon et al. Both of these instances utilized endobronchial valves for very distal BPF in patients on ECMO.22,23 Their results were similar to ours, where endobronchial valve placement facilitated weaning on ECMO. Traditionally, one of the main challenges to utilization of valves is identifying the bronchus for deployment. One of the most commonly performed maneuvers is to utilize a fogarty balloon, serially occluding bronchial segments and visualizing the chest tube for cessation of air leaks. However, this method is not feasible with multiple BPF, as the air can be diverted to other segments during selective occlusion. In the presented case, utilizing selective bronchographic mapping allowed for proper identification of the BPF. By utilizing endobronchial valves in combination with embolization, lung recruitment could be achieved without compromising the main bronchial segments.
In this case, we demonstrated successful management of multiple bilateral BPF by a minimally invasive approach using selective embolization and endobronchial valve placement. Ultimately, the combination of these techniques allowed for the necessary lung recruitment maneuvers and pulmonary support for ECMO weaning. Despite the patient's overall grim prognosis, a multidisciplinary approach provided the necessary interventions and treatment, ultimately leading to a favorable outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.