
Abstract
Abstract
Background:
Headscarf use is becoming more common throughout the world. Many articles describe the problem of aspirated headscarf pins but few if any give technical details for retrieval or innovative methods of removal if traditional bronchoscopy fails particularly in the pediatric population. Herein, we describe our method of deep sedation with laryngeal mask airway (LMA) and flexible bronchoscopy (FB) and retrieval with a stepwise algorithm if traditional FB fails.
Methods:
A retrospective review of pediatric patients with aspirated headscarf pins was performed. Patient demographics, symptomatology, procedure specifics, and outcomes were recorded.
Results:
Fifty-six patients had pins removed at our institution between January 2010 and May 2017. Ninety-one percent were female. Each had a history of aspiration of a needle confirmed by a chest X-ray. The most common presenting symptom was cough in 48%. Only a small minority had physical exam findings (9% either wheezing or decreased air entry). FB via LMA under deep sedation was used as a primary intervention and was successful in 52 of 56 cases (93%). Fluoroscopy was added to aid the FB in 3 cases and was successful in 2 of the 3 patients. Two patients underwent mini-thoracotomy for removal. All pins were removed successfully and none of the patients had any postprocedural complications.
Conclusion:
Surgeons caring for pediatric patients throughout the world should be knowledgeable in a common problem often facing girls wearing headscarves. Given the majority of the needles are in segmental bronchi in teenage girls, we recommend FB as the primary modality with the addition of fluoroscopy to guide if needed and video-assisted thoracoscopy or mini thoracotomy if less invasive methods fail.
Introduction
A
Since many of these patients are teenage girls, there is all the more reason to have a clear plan with an algorithm should the primary plan not prove successful. Some publications, even from our institution, have advocated for conscious sedation and a combination of the abovementioned retrieval methods.6,7 However, this method does not isolate the esophagus from the trachea and has either led to more procedures to remove pins from the esophagus or waiting for spontaneous passage from the gastrointestinal tract. Others have described general anesthesia 8 but most do not have a detailed description of the anesthetic approach. Our aim was to review our hospital's experience with aspirated pins in all patients to assess the efficacy of our methods for retrieval. Additionally, we offer some “lessons learned” in retrieving the more difficult cases.
Materials and Methods
After Institutional Review Board approval was obtained, we conducted a retrospective study of a prospectively collected database of aspirated headscarf pins in patients up to 18 years of age between January 2010 and May 2017 at a tertiary teaching hospital. Patient demographics, presenting signs and symptoms, radiologic findings, operative notes and findings, lengths of stay, and outcomes were reviewed.
Each patient received deep sedation in the operating room via a laryngeal mask airway (LMA). The vocal cords were anesthetized with local anesthetic and an appropriately sized flexible bronchoscope was inserted down the LMA. The foreign bodies were grasped using alligator forceps through the working channel of the flexible bronchoscope. At times, the pin was beyond the reach of the bronchoscope. If this was the case, an aliquot of saline was instilled and often the pin would float into reach. If the foreign body was dropped exiting the vocal cords, it fell into the LMA and was easily retrieved. Uncommonly, when the foreign body was not visible, fluoroscopy was utilized to guide the bronchoscopy. In rare cases where the foreign body was not visible because of migration into the parenchyma or because of resultant granulation tissue a mini thoracotomy was performed.
Results
Fifty-six patients underwent removal of pins from their airways during the 88 months time period. Basic patient demographics are summarized in Table 1. The large majority of the patients were female (91%). The pins accidently aspirated by the male patients while they were holding the pins between their lips for different reasons. The mean age was 13.3 years old (range 0.9–18 years). A histogram of the patient ages is presented in Figure 1.

Histogram showing age distribution of aspirated headscarf pins.
Of the 56 patients, 52 were successfully removed with FB through an LMA. Of the 4 remaining patients requiring more advanced procedures, 2 were removed with fluoroscopy assistance guiding the bronchoscope to the foreign body while 2 required an invasive procedure, in our case, mini-thoracotomy.
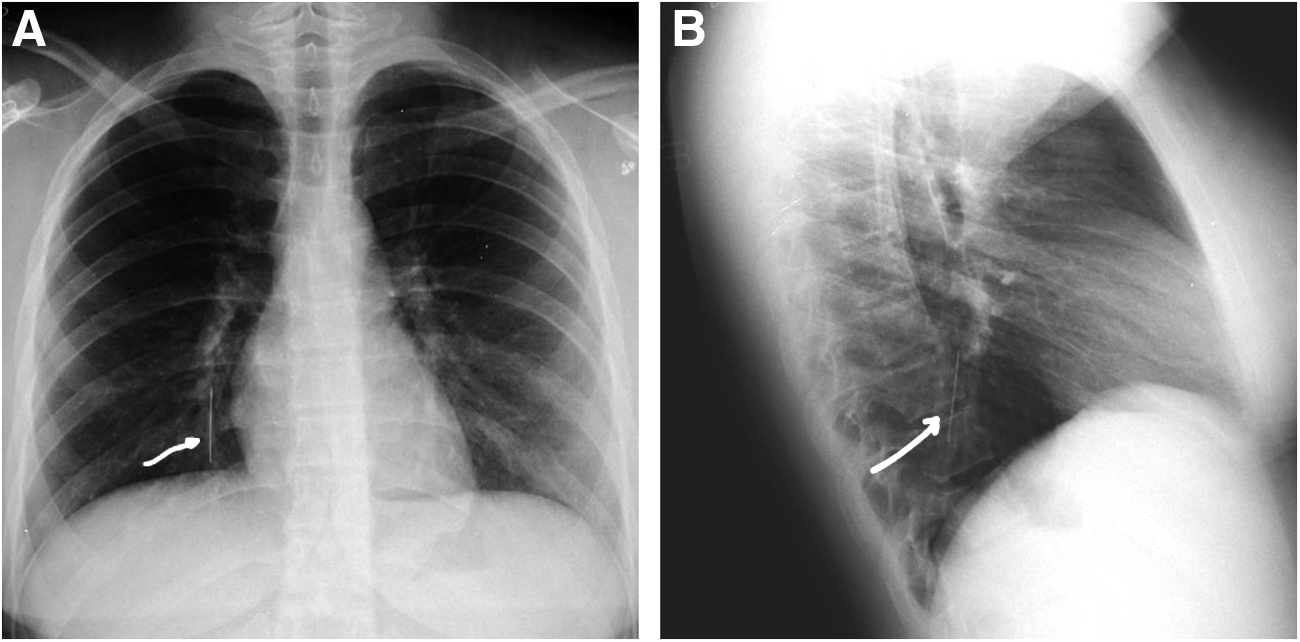
All patients had a positive history of aspirating a foreign body but less than half had cough (48%) and other symptoms of shortness of breath (18%), chest pain (5.4%), and wheezing (5.4%) were even less common. Additionally, physical exam findings were lacking in our patient population with only 2 of the 56 (3.6%) having lateralizing findings on auscultation. Interestingly, 2 of the 3 patients who had wheezing went on to receive more advanced procedures. Of the 4 patients needing more advanced procedures, all had cough where only 48% of the total population presented with cough. The presence of the pins was confirmed by a chest X-ray (Fig. 2A, B). None of these preprocedure predictors of failure of standard bronchoscopic removal reached significance due to the low numbers of patients.
The successful methods of removal are summarized in Table 2. Fifty-two needles were removed with FB alone and did not need any other procedures. Four patients needed more advanced procedures. FB and fluoroscopy was used in 3 patients and was successful in 2. The remaining 2 patients (1 failed fluoroscopy and 1 not attempted) underwent mini-thoracotomy with removal. The average length of stay for patients with simple flexible bronchoscopic removal (admission to discharge) was 1.5 days (range 1–3). The patients who received the successful combination of bronchoscopy and fluoroscopy stayed 2 and 4 days. The patient who stayed 4 days was an asthmatic who had an exacerbation during his hospitalization. The patients who underwent mini-thoracotomy each stayed 4 and 6 days in the hospital.
FB, flexible bronchoscopy; LOS, length of stay.
Table 3 contains the sites of the pins. Only 7 (13%) were in the trachea and the pins were nearly equally distributed between 25 (44%) right and 24 (43%) left side if they were not in the trachea. If the pins made it to one side or another, most were found in a segmental bronchus with the right segment 10 being the most common single segment. Predictably, the single pin found in the parenchyma necessitated a mini-thoracotomy for removal. The other patient who required a mini-thoracotomy was the youngest patient in our series who had a large amount of granulation tissue in the right main stem bronchus preventing passage of the bronchoscope.
NA, not applicable.
All pins were oriented head-down, meaning the tip of the pin was oriented upward toward the bronchoscope as illustrated in Figure 3. This presented challenges when the needle was either bent or coughed back up the bronchus causing the tip to lodge in the wall of the bronchus. The first scenario was the most challenging especially if the head of the pin was completely occluding a segmental bronchus. Even without coughing, the orientation of the pin would often lodge in the side and cause the removal to be more challenging. Using a combination of saline to float the needle out (if not lodged in the wall) or grasping as close to the tip and pushing distally to dislodge while still controlling the tip of the needle for removal. The second scenario is challenging as well and can often require quite a bit of force to push the needle distally to ultimately be able to remove it. At times removal with bronchoscopy took upward of 30 minutes of bronchoscopy time. Removal of challenging pins requires tremendous patience. When the pin is not found by bronchoscopy, fluoroscopy aided the locating of two of three of the pins obviating the need for an operation in those patients.
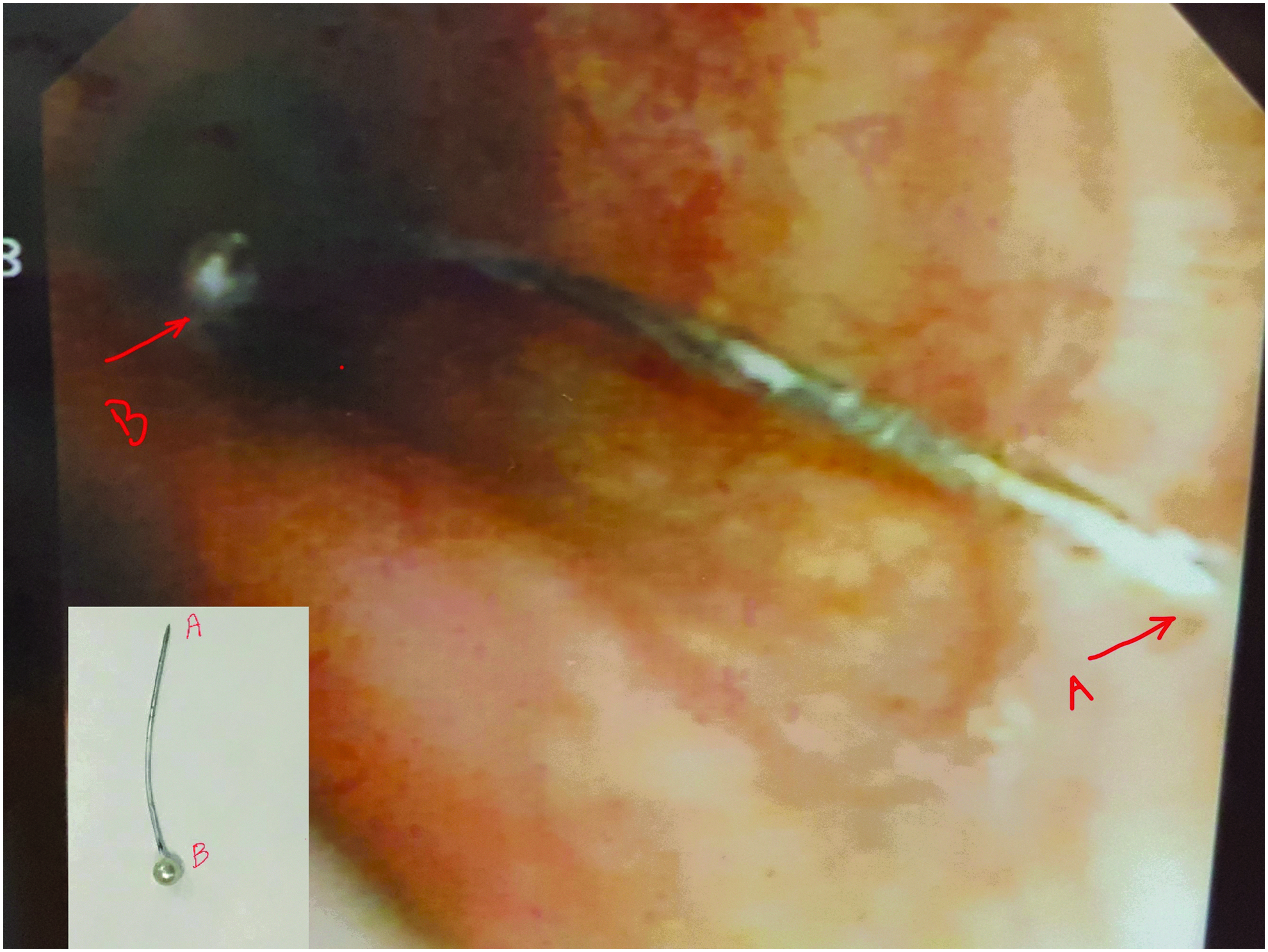
Flexible bronchoscopic view of aspirated pin with the head, B, oriented distally and the tip, A, oriented proximally.
There were no complications observed in any patient.
Discussion
Removal of aspirated straight pins is relatively common among young scarf-wearing women as they learn to wear the scarf.1–8 Pediatric surgeons typically default to rigid bronchoscopy for airway and esophageal foreign body removal as many of the foreign bodies are proximal given the small diameter of the airway in children. The aspirated pins described here have a smaller diameter and are often aspirated by older children with larger airways and therefore are found deeper within the airway. In our series we found they were most likely to be located in segmental bronchi. Given the depth of location, we recommend FB as a first-line therapy for aspirated pins. We have found FB through an LMA under deep sedation to be the easiest and most useful method as it provides easy access to the vocal cords, it can reach up to the segment orifices and if the pin is dropped as it passes through the vocal cords it is not swallowed or misplaced in the oropharynx. Our suggested algorithm for removal is detailed in Figure 4.
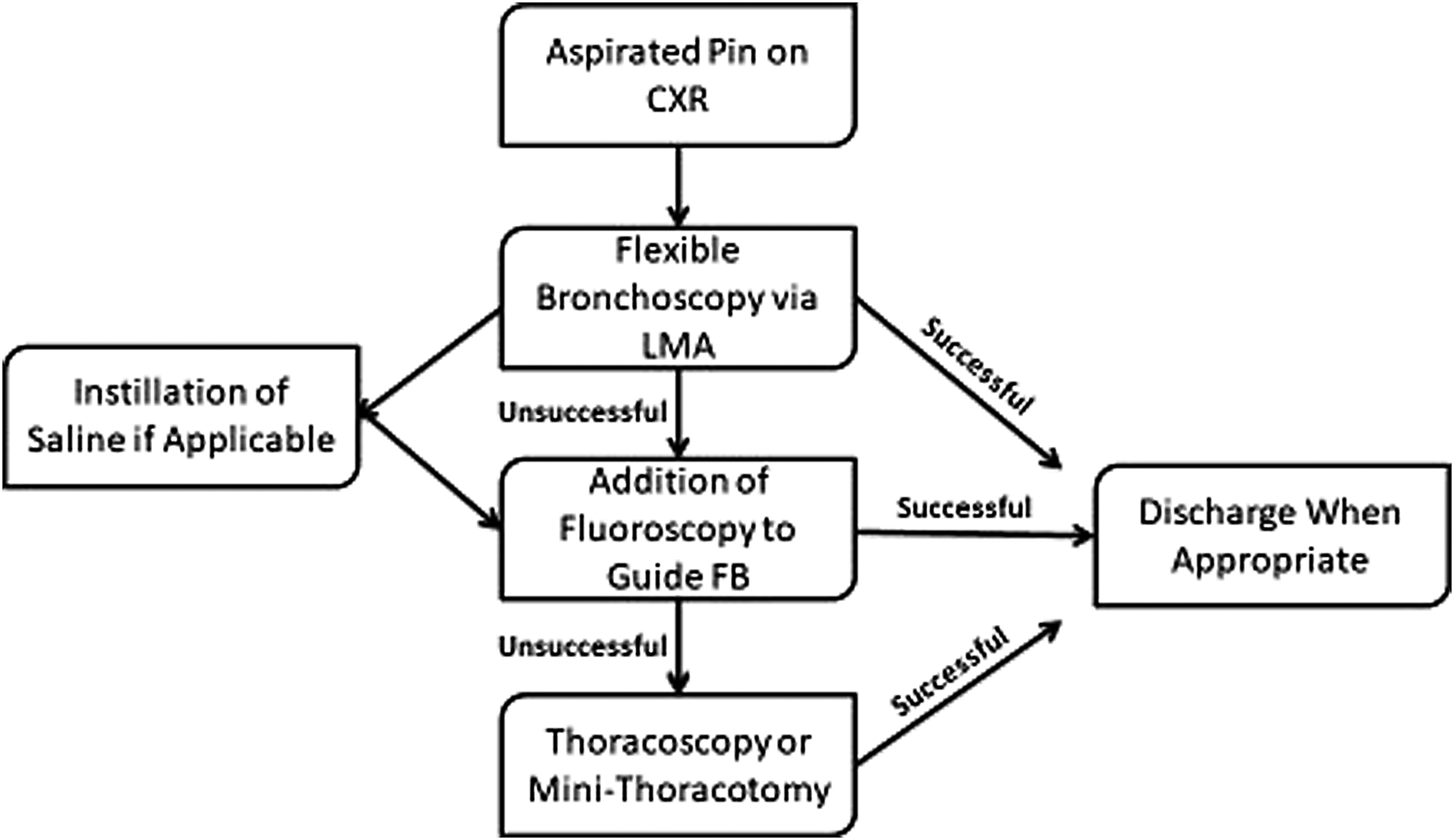
Suggested algorithm for removal of aspirated headscarf pin with flexible bronchoscopy via LMA. CXR, chest X-ray; LMA, laryngeal mask airway; FB, flexible bronchoscopy.
When comparing our series to others of comparable size, our 3.5% need for mini-thoracotomy is lower than most. Without the use of fluoroscopy, our rate of mini-thoracotomy would have doubled and be at the level of most larger series. We believe that the addition of fluoroscopy during bronchoscopy allows the surgeon to decrease the number of invasive procedures for this subset of challenging patients.
In our series, mini-thoracotomies were our invasive method of choice. Others have suggested video-assisted thoracoscopy as an alternate method. 4 We certainly concede that video-assisted thoracoscopy could be a reasonable option and we may offer for the next patient whose pin is not amenable to removal with noninvasive methods. We also predict that fluoroscopy could be useful during the video-assisted thoracoscopic procedure as well.
With the vast majority of patients not needing an invasive method of removal, ideally we would like to predict preoperatively which patients are at higher risk of failing noninvasive means of removal. Unfortunately, the rarity of the need for invasive removal makes such predictions difficult. However, we found that of the 3 patients with wheezing, 2 needed mini-thoracotomies. Additionally, 2 children were very young in our series, 11 months and 1.4 years, with the 11-month-old requiring a mini thoracotomy. It is unclear when the 11-month-old child aspirated the pin but there was enough granulation tissue in the right mainstem bronchus to preclude visualization and removal with bronchoscopy. Because of this, we speculate that younger patients with limited or unknown history are at higher risk for needing more extensive procedures given the size of the airway and potential for chronicity causing an inflammatory reaction increasing the difficulty of a successful bronchoscopy. And finally, in the 2 fluoroscopic cases and the older thoracotomy case the pins were found in segmental bronchi or in the parenchyma, respectively. Clearly if the pin was more centrally located on preprocedure chest X-ray, this would predict a higher likelihood of success in bronchoscopic removal.
Our study is retrospective in nature and subject to all the limitations inherent to that method of analysis. Additionally, the low numbers of patients needing advanced methods of removal made it difficult to provide statistical basis for our recommendations.
Despite the limitations, we conclude that pin aspiration is a commonly encountered malady among young scarf-wearing women. There are few, if any, preprocedure signs or symptoms that are reliable for identifying patients who will fail standard FB. However, a stepwise approach to the removal of these foreign bodies can prevent unneeded aggressive intervention.
Footnotes
Disclosure Statement
All authors claim that no conflict of interest exists.