
Abstract
Abstract
Introduction:
The laparoscopic repair of Morgagni's hernia (MH) has been reported to be safe and feasible. However, it is still unclear whether laparoscopy is superior to open surgery in repairing MH.
Materials and Methods:
Using a defined search strategy, three investigators independently identified all comparative studies reporting data on open and laparoscopic MH repair in patients <18 years of age. Case reports and opinion articles were excluded. Meta-analysis was conducted according to PRISMA guidelines and using RevMan 5.3. Data are expressed as mean ± SD.
Results:
Systematic review - Of 774 titles/abstracts screened, 51 full-text articles were analyzed. Three studies were included (92 patients), with 53 (58%) open approaches and 39 (42%) laparoscopy. Meta-analysis - The length of surgery was shorter in laparoscopy (50.5 ± 17.0 min) than in open procedure (90.0 ± 15.0 min; P < .00001). Laparoscopy shortened the length of hospital stay (2.1 ± 1.4 days) versus open surgery (4.5 ± 2.1 days; P < .00001). There was no difference with regards to complications (laparoscopy: 8.8% ± 5.5%, open: 9.4% ± 1.6%; P = .087) and recurrences (laparoscopy: 2.9% ± 5.0%, open: 5.7% ± 1.8%; P = .84).
Discussion:
Comparative studies indicate that laparoscopic MH repair can be performed in infants and children. Laparoscopy is associated with shortened length of surgery and hospital stay in comparison to open procedure. Prospective randomized studies would be needed to confirm present data.
Introduction
M
Although the majority of Morgagni hernias are asymptomatic, usually repair is recommended to avoid future complications. Surgical options include open repair (transabdominal or transthoracic route), or laparoscopic repair. The first laparoscopic repair was performed by Kuster et al. in 1992, 4 and since then it has become a popular approach among pediatric surgeons. Ponsky et al. reported that in the suspicion of Morgagni hernia with a nonconclusive radiologic workup, laparoscopy is an effective technique to diagnose and then repair the hernia in infants and children. 5 Following several successful single case experiences reported in the literature, large series and multicenter studies have confirmed that laparoscopic repair of Morgagni hernia is a safe and feasible approach for infants and children.6–8 However, given the rarity of this condition, there is still no consensus among pediatric surgeons on whether the gold standard for Morgagni hernia repair is via an open or a laparoscopic approach. A recently published retrospective study from eight pediatric surgical centers has shown that the laparoscopic technique is well standardized and associated with a very low recurrence rate in experienced hands. 8 The authors concluded that children with Morgagni hernia should always be treated by laparoscopy and only in centers with high-volume minimally invasive surgery activity. 8 However, this study, like many others, was noncomparative and lacked an open surgery group.
Therefore, to establish the evidence-based gold standard approach for Morgagni hernia repair in infants and children, we performed a systematic review and meta-analysis, where we interrogated the literature on whether one surgical approach may be superior to the other.
Materials and Methods
Both the systematic review and meta-analysis were drafted with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 9 Two different health librarians were involved: the Gerstein Science Information Centre (University of Toronto, ON, Canada) and the Bibl@Ud'A (“d'Annunzio” University of Chieti-Pescara, Italy).
Systematic review
This study was registered on PROSPERO—international prospective register of systematic reviews (registration number: CRD42017055297). 10 A systematic review of the literature was made using a defined search strategy. Three investigators (G.L., E.Z.R., and V.C.) independently searched scientific databases (PubMed, Medline, Cochrane Collaboration, Embase, and Web of Science) using a combination of keywords (Table 1). MeSH headings and terms used are “Congenital Morgagni('s) diaphragmatic hernia AND (laparoscopy OR open procedure)” and “Morgagni('s) hernia AND (laparoscopy OR open procedure)” (Supplementary Data S1; Supplementary Data are available online at www.liebertpub.com/lap). Case reports, opinion articles, and case series with less than 10 patients were excluded. All gray literature publications (i.e., reports, theses, conference proceedings, bibliographies, commercial documentations, and official documents not published commercially) were excluded. The full text of the potentially eligible studies was retrieved and independently assessed for eligibility by the same three investigators. Any disagreement between them over the eligibility of particular studies was resolved through discussion with a fourth author (A.Z.).
Meta-analysis
Only studies comparing open versus laparoscopic approach to treat Morgagni hernia in infants and children were included. Patients were divided into two groups according to the surgical approach (open or laparoscopic). Outcome measures included patient demographics (age and weight at surgery), intraoperative results (length of surgical procedure, percentage of conversion to laparotomy in laparoscopic procedures, and incidence of Morgagni hernia repair with patch), and postoperative measures (time to full feed, length of hospital stay, complications, and recurrences). The meta-analysis was conducted with RevMan 5.3, 11 using the random-effects model to produce risk ratio (RR) for categorical variables and mean differences (MD) for continuous variables, along with 95% confidence intervals (CI). We produced I2 values to assess homogeneity and quantify the dispersion of effect sizes. Publication biases were assessed using the funnel plot method.
Data were compared using Fisher's Exact Test and are expressed as mean ± SD. When median and range were reported, mean ± SD were estimated, as previously reported. 12
Quality assessment
Risk of bias for individual studies was assessed in duplicate (G.L. and E.Z.R.) using the methodological index for nonrandomized studies (MINORS). 13 Differences between the two reviewers (G.L. and E.Z.R.) were resolved through consensus and discussion with a third author (V.D.C.). The total score for this 12-item instrument ranges 0–24 points with a validated gold standard cutoff of 19.8.
Two authors (P.L.C., and A.P.,) independently evaluated the present systematic reviews and meta-analysis using A Measurement Tool to Assess Systematic Reviews (AMSTAR). 14
The PRISMA checklist of our study was then completed. 9
Results
Systematic review
Of 774 abstracts screened, 51 full-text articles were thoroughly examined, and three studies met our inclusion criteria (Fig. 1). There were no randomized controlled trials. Selected articles were all retrospective and included 92 patients, with 53 (58%) open repair and 39 (42%) laparoscopic repair (Table 2).15–17 The age at surgery was mentioned in only one study 17 with no differences between open (median 10 months, range 1–60 months) and laparoscopic repair (median 15 months, range 8–42 months; P = ns; Table 3). The weight at surgery was also reported in one article 16 with no differences between open (7.9 ± 18.1 kg) and laparoscopic surgery (9.4 ± 22.9 kg; P = ns; Table 3).
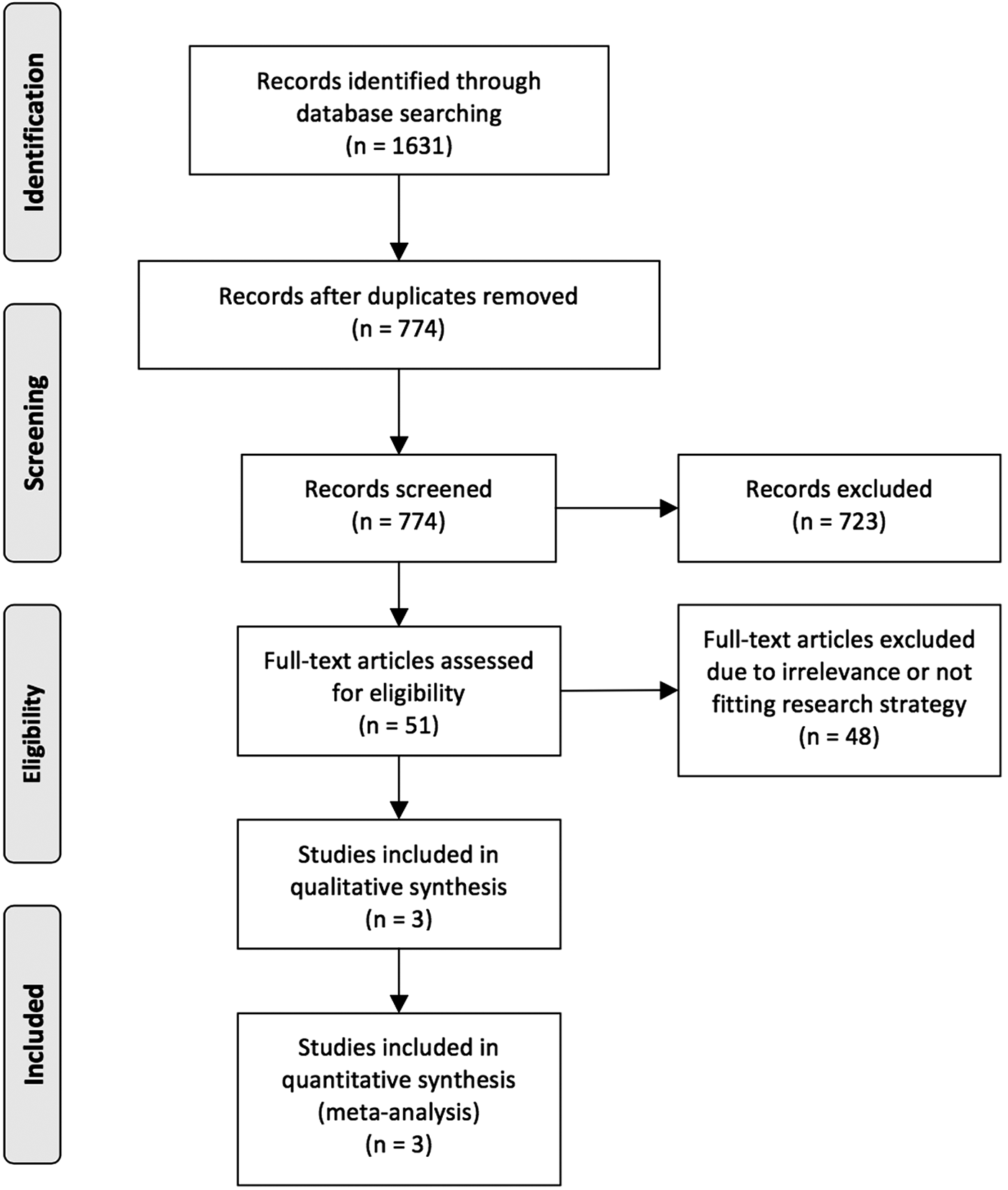
Diagram of workflow in the systematic review and meta-analysis.
Data are reported as mean ± SD or median (range).
n.r., not reported.
n.s., not significant.
Meta-analysis
The length of surgery was mentioned only in one article by Al-Salem et al., 17 where it was reported to be shorter in laparoscopy [median (range) = 40 (27–95) minutes; estimated mean ± SD = 50.5 ± 17.0 minutes] in comparison to the open procedure [median (range) = 90 (60–120) minutes; estimated mean ± SD = 90.0 ± 15.0 minutes; P < .00001, Table 3]. Conversion from laparoscopy to open approach, mentioned in one article, 16 occurred in 3 children out of 12 (25%). Furthermore, the same study was the only one to report the requirement of a patch repair, 16 with no difference between laparoscopy (5/9 patients, 55.5%) and open procedure (1/8 patients, 12.5%; P = ns, Table 3).
When mentioned, 17 laparoscopy was reported to be associated with a shorter time to full feed (median 1 day, range 0.8–1.5 days) in comparison to the open procedure (median 2.1 days, range 1.7–3.1 days; P < .00001, Table 3). As a result, patients undergoing the laparoscopic repair had a shorter length of hospital stay (2.1 ± 1.4 days) in comparison to those who had open surgery (4.5 ± 2.1 days; P < .00001; MD −2.46 [95% CI −3.43 to −1.49], Fig. 2). There was no significant heterogeneity between the studies included in the meta-analysis (I2 = 53%, P = ns). The funnel plot of published studies demonstrated a convincing symmetry indicating no potential publication bias, although symmetry is difficult to determine with only two studies contributing to the funnel plot.

Forest plot comparison of the length of hospital stay after laparoscopy and open procedure to treat Morgagni hernia.
The incidence of overall postoperative complications was not different between patients who underwent a laparoscopic repair and those who had an open repair (laparoscopy: 3/34 patients, 8.8% ± 5.5%, open: 5/53 patients, 9.4% ± 1.6%; P = .80; RR 1.23 [95% CI 0.25–6.14]; I2 = 18%; Fig. 3A). Similarly, the prevalence of recurrence between the two groups was comparable (laparoscopy: 1/34 patients, 2.9% ± 5.0%, open: 3/53 patients, 5.7% ± 1.8%; P = .95; RR 1.08 [95% CI 0.09–13.63]; I2 = 40%; Fig. 3B).
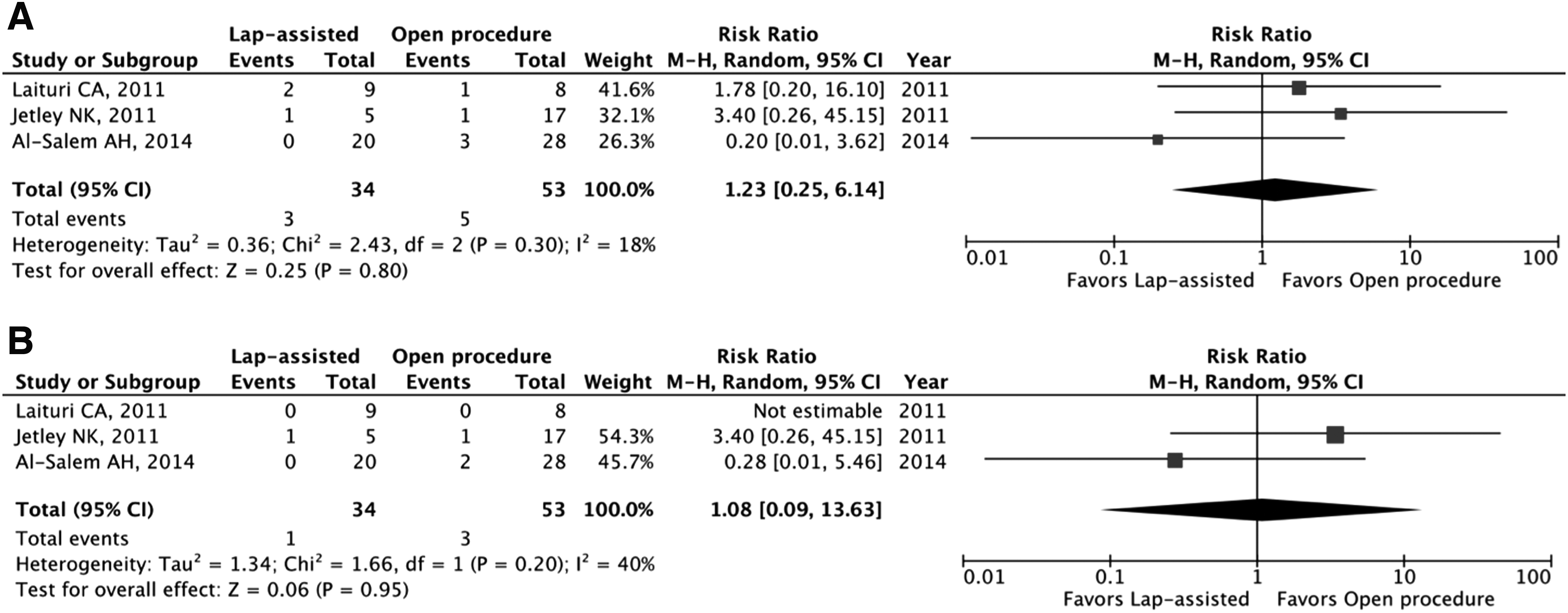
Forest plot comparison between laparoscopic and open repair for Morgagni hernia on
Discussion
This study indicates that laparoscopic repair of Morgagni hernia in infants and children can have some advantages compared to the open repair: laparoscopy is associated with shorter surgical procedure, time to reach full feeds, and postoperative length of hospital stay. However, the prevalence of postoperative complications and hernia recurrences are similar following both procedures.
The diaphragm of infants born with a congenital diaphragmatic hernia, either the classical Bochdalek type or the Morgagni hernia, can be repaired by various surgical approaches: trans-abdominal or trans-thoracic open techniques, and laparoscopic or thoracoscopic minimally invasive techniques. 18 Due to the anatomical position of the foramen of Morgagni, surgeons have classically preferred the trans-abdominal route for repair, as inspection of hernia contents and reduction is easy, access and repair of bilateral hernias is feasible and inspection and correction of a potential associated malrotation is possible. 19 As an alternative, some surgeons have supported the trans-thoracic approach, as it allows an easy freeing of the pleural adhesions from the hernia sac.20,21 However, this approach cannot always guarantee a good view of both sterno-costal triangles and bilateral hernia may be missed. 8 For this reason, the thoracoscopic repair of Morgagni hernia has not become popular. 22
The open trans-abdominal approach requires exposure of the central portion of the diaphragm, via either an upper midline or an upper transverse incision. A large abdominal scar may be disappointing given that these defects are commonly small, simple to repair, and patients are usually asymptomatic and not physiologically compromised. 16 Over the last decade, the laparoscopic repair has become the standard at many centers and the debate in the literature has mainly focused on the two variants of trans-abdominal approach. In our analysis, we did not include patients who underwent a trans-thoracic repair, to maintain a homogeneous comparison. Moreover, only very few studies report the outcome of the trans-thoracic approach in children.
As for the classical Bochdalek hernia, Morgagni hernia can be repaired primarily or with a patch. Primary repair is usually feasible and can be performed by bringing the anterior and posterior portions of the defect together with interrupted synthetic nonabsorbable sutures. 23 This can be achieved also via laparoscopy as recently reported by Esposito et al., who concluded that with a standardized technique hernia recurrence and need for a patch are both very low. 8 To reduce the tension on the suture line, some surgeons have advocated the use of the transparietal stitch to suspend the diaphragm to the abdominal wall.6,23 Particularly, Azzie et al. proposed the placement of interrupted synthetic nonabsorbable sutures through the full-thickness of the anterior abdominal wall, incorporating the posterior rim of the defect and returning back out through the anterior abdominal wall, with the sutures tied in the subcutaneous tissue. 24
However, when required, a patch overlapping the edges of the Morgagni hernia defect provides a good tension-free repair, even laparoscopically.25,26 In particular, Garriboli et al. reported that five children out of 12 (42%), all laparoscopically repaired without a patch, developed a hernia recurrence and required a patch closure. 27 Given the high recurrence rate, the authors advocated for a more liberalized use of the patch. 27 In our meta-analysis, we did not find any difference in the percentage of patch use or rate of hernia recurrence between laparoscopic and open repair (Table 3).
We acknowledge that there are limitations in our present study mainly due to the fact that a meta-analysis relies on the quality of the studies and data available in the literature. In our meta-analysis, all studies included were retrospective (Table 2). None of the studies reached the gold standard cutoff on MINORS of 19.8 out of 24 (Table 4). All three articles used retrospective data and reported inadequate baseline data (e.g., not adequate comparison of comorbidities between the two groups). None of the studies reported blind evaluation of objective endpoints or provided sample size calculations. Moreover, only in the study by Jetley et al. 15 mentioned both the length of follow-up and the loss to follow-up. Furthermore, the endpoints were appropriate and complete to the aim of the study only in the article by Al-Salem et al. 16 and the incidence of conversion in laparoscopic group was mentioned only by Laituri et al. 17 However, when independently assessed by two authors using AMSTAR, the present systematic reviews and meta-analysis received a relevant score (Supplementary Table S1). Finally, the PRISMA checklist of our study was completed (Supplementary Table S2).
See Ref. 13
0 = not reported.
1 = reported but inadequate.
2 = reported and adequate.
In conclusion, this study shows that there is a lack of evidence in the literature to determine the gold standard surgical approach to repair Morgagni hernia in infants and children. Nonetheless, three comparative nonrandomized studies indicate that laparoscopic repair of Morgagni hernia in infants and children is associated with shortened length of surgical procedure and hospital stay in comparison to open surgery. Prospective randomized studies with long-term follow-up would be needed to confirm present outcome data.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.