
Abstract
Abstract
Background:
Pancreatic ductal obstruction leading to ductal dilation and recurrent pancreatitis is uncommon in children. Treatment is dependent upon etiology but consists of decompression of the pancreatic duct (PD) proximally, if possible, by endoscopic retrograde cholangiopancreatography (ERCP) intervention or surgical decompression with pancreaticojejunal anastomosis.
Methods:
After institutional review board approval, we retrospectively reviewed the records for 2 children who underwent lateral pancreaticojejunostomy for pancreatic ductal dilation. Data, including demographics, diagnostic studies, operative details, complications, outcomes, and follow-up, were analyzed.
Results:
Case 1 was a 4-year-old female with pancreatic ductal obstruction with multiple episodes of recurrent pancreatitis and failure of ERCP to clear her PD of stones. She underwent a laparoscopic cholecystectomy with a lateral pancreaticojejunostomy (Puestow procedure). She recovered well with no further episodes of pancreatitis and normal pancreatic function 4 years later. Case 2 was a 2-year-old female who developed recurrent pancreatitis and was found to have papillary stenosis and long common bile-PD channel. Despite multiple sphincterotomies, laparoscopic cholecystectomy, and laparoscopic hepaticoduodenostomy, she continued to experience episodes of pancreatitis. She underwent a laparoscopy converted to open lateral pancreaticojejunostomy. Her recovery was also smooth having had no episodes of pancreatitis or hospital admissions for over 2 years following the Puestow.
Conclusions:
Indication for lateral pancreaticojejunostomy or Puestow procedure is rare in children and even less often performed using laparoscopy. In our small experience, both patients with pancreatic ductal obstruction managed with Puestow's procedure enjoy durable symptom and pain relief in the long term.
Introduction
C
Relieving pancreatic ductal obstruction remains the primary surgical treatment to achieve durable pain relief in such children when not amenable to endoscopic techniques.4,5 Laparoscopic approaches to pancreatic surgery are limited to specialized centers, however, they have been found to be as effective as an open approach. 6 In this study, we report our experience with two cases of chronic pancreatitis with ductal dilation managed by both laparoscopic, as well as open lateral, pancreaticojejunostomy with subsequent resolution of disease symptomatology at longer term follow-up.
Case 1
A 10-month-old girl with duodenal obstruction due to annular pancreas was treated with a laparoscopic duodenoduodenostomy at that time. She recovered from this operation, but in the ensuing 2 years developed recurrent episodes of pancreatitis wherein she was managed with pain control and bowel rest for each time. On a subsequent admission, she presented with epigastric pain, elevated lipase (10,828 IU), white blood cell count of 16.8k, and amylase 1072 IU. Ultrasound (US) of abdomen obtained demonstrated increasing pancreatic ductal dilatation from 6 mm (as seen on US 1 month prior) to 8 mm and she was now 4 years of age.
Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) demonstrated anomalous and dilated pancreatic ductal anatomy. These studies revealed a stricture in her proximal main pancreatic duct (PD) with a proximal stone and extreme dilatation of her main PD from the pancreatic head out toward the tail with areas measuring from 6 to 10 mm (Fig. 1). An accessory PD was found to be draining the uncinate process and head of pancreas, and this appeared relatively normal. An endoscopic retrograde ERCP performed at the most recent admission was unsuccessful in relieving the stricture in the main PD or retrieving the stone from the head of the pancreas. At this point, she was referred for operative intervention. A laparoscopic cholecystectomy with a lateral pancreaticojejunostomy (Puestow procedure) was performed in February of 2014. At the time of operation, she weighed 17.1 kg.
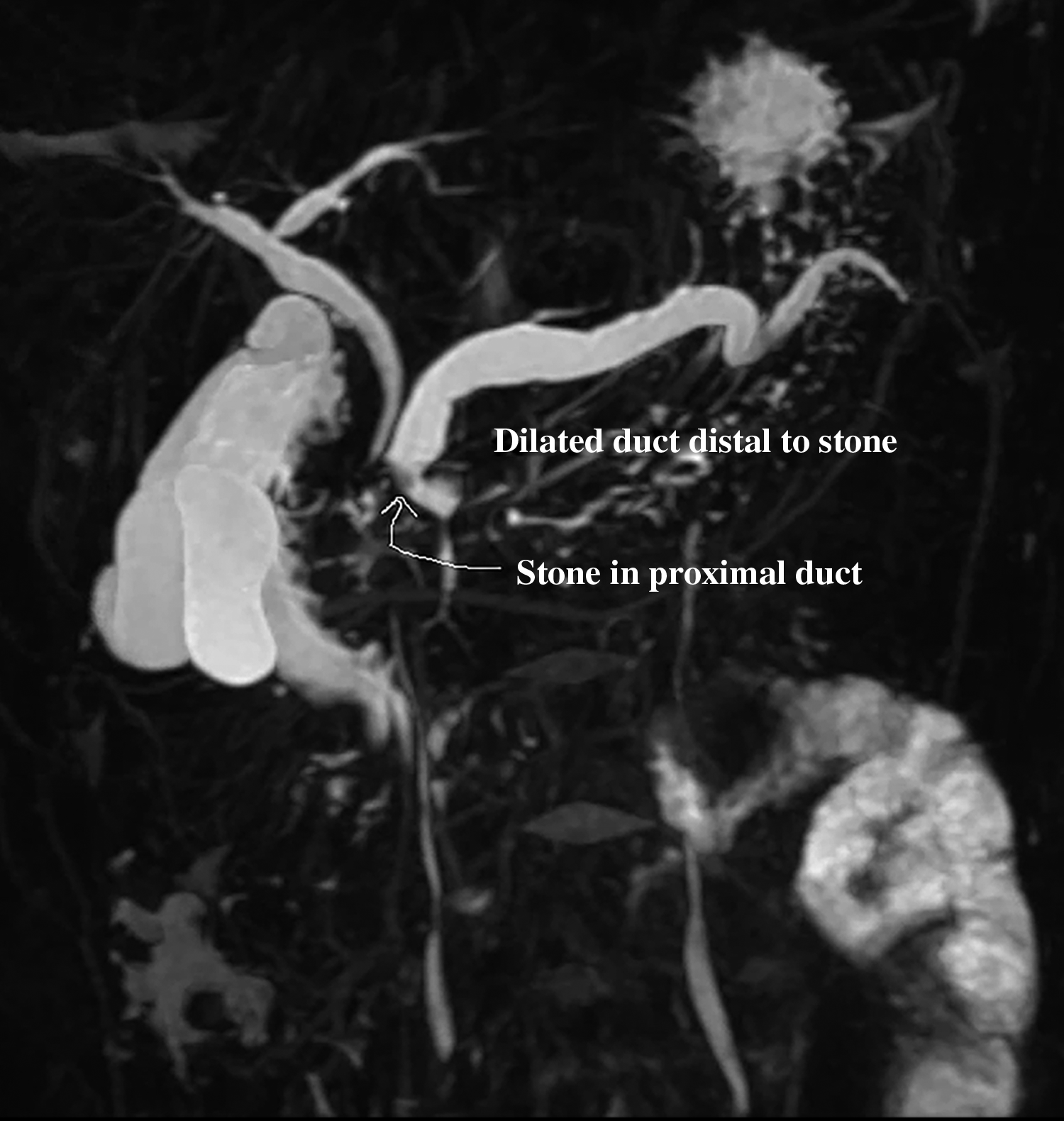
Magnetic resonance cholangiopancreatography in Case 1 showing dilated and tortuous PD (6–10) mm with filling defect (stone) in proximal duct. PD, pancreatic duct.
Technique
A 12 mm trocar was placed through the umbilicus, and four additional trocars were placed (two 5 mm trocars in the right lower quadrant and right mid abdomen and two in the left upper quadrant and left lower abdomen). A cholecystectomy was performed in a top-down manner secondary to the adhesions. The gallbladder was removed through the umbilical trocar. The lesser sac was entered by opening the gastrocolic omentum with hook electrocautery from the head of the pancreas out to the distal pancreatic body. Two transabdominal 2-0 polydioxanone suture (PDS) sutures were passed through the anterior abdominal wall into the back wall of the stomach and out back through the anterior abdominal wall and tied extracorporeally to expose the entire pancreas. At laparoscopy, a laparoscopic US probe was used to identify the ductal anatomy of the pancreas (Fig. 2). The dilated PD was easily identifiable, and the surface of the pancreas overlying the duct was marked with electrocautery with the aid of US. An incision was made in the pancreas with electrocautery through the pancreatic parenchyma until the PD was encountered. The clear pancreatic fluid was emanating once the duct was opened (Fig. 3). The duct was opened longitudinally both proximally on the pancreas toward the pancreatic head and distally so that the entire length of the pancreatotomy was 5 cm (Fig. 4). The PD was irrigated with a suction irrigator, and multiple small fragments of debris were removed from the duct. A 3-Fr Fogarty catheter was passed through this proximally into the main PD, the balloon inflated, and this was pulled back to retrieve the large single stone that was identified on the preoperative magnetic resonance imaging which was obstructing the proximal PD (Fig. 5). Once the stone was removed, the PD was flushed with saline and cleared out along its entire length. There were no other additional stones. A Roux-en-Y limb for the pancreaticojejunostomy was created extracorporeally through the umbilicus. This was replaced back into the abdomen followed by reinstitution of laparoscopy and pneumoperitoneum. The defunctionalized limb of the Roux-en-Y was brought up to the pancreas through the transverse mesocolon. The jejunum was attached to the lower aspect of the pancreas using three interrupted 3-0 silk stay sutures. An enterotomy was made in the jejunal limb with electrocautery over a length of ∼5 cm. An anastomosis was made between the superior wall of the intestine and the inferior wall of the PD opening using a 3-0 PDS running suture. An anterior row of 3-0 PDS sutures was used to achieve the superior pancreaticojejunostomy anastomosis between the superior aspect of the PD and inferior aspect of the jejunostomy. Following the completion of the anastomosis, a few stay sutures were placed to take tension off the jejunal limb on the pancreas (Fig. 6). The mesenteric defect in the transverse mesocolon was closed with Vicryl sutures. A drain was placed through the left lower quadrant trocar site over the pancreaticojejunostomy anastomosis and removed before discharge home.

Laparoscopic ultrasound probe was used to identify the ductal anatomy of the pancreas and guide pancreatotomy incision.
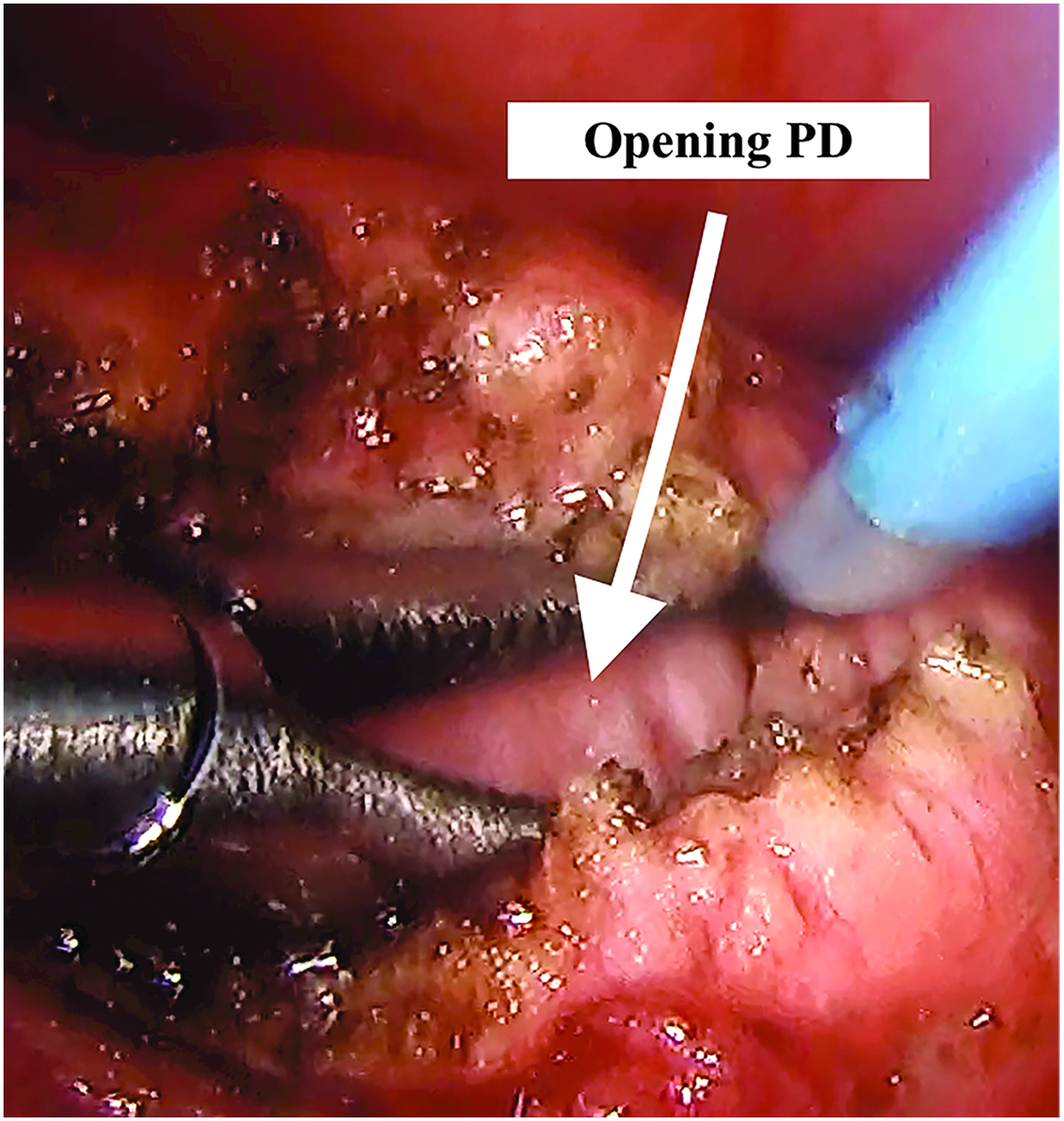
Pancreatotomy initiated with cautery until the main duct was entered. PD, pancreatic duct.

Pancreatotomy was performed over the entire anterior pancreas and extended proximally and distally for length of ∼5–6 cm. PD, pancreatic duct.
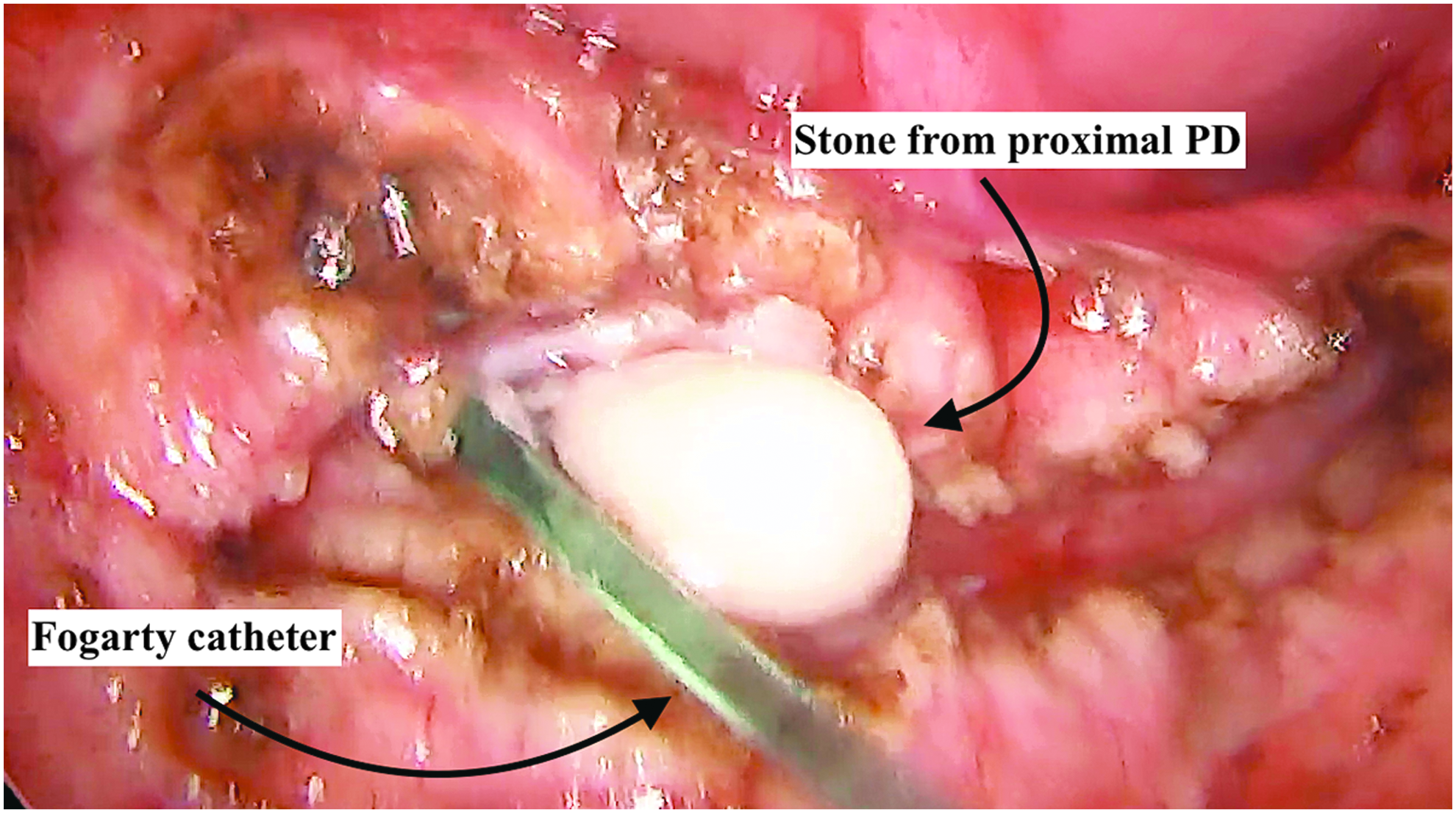
A 3-Fr Fogarty catheter was passed proximally into the main PD, the balloon inflated, and this was pulled back to retrieve a large single stone. PD, pancreatic duct.
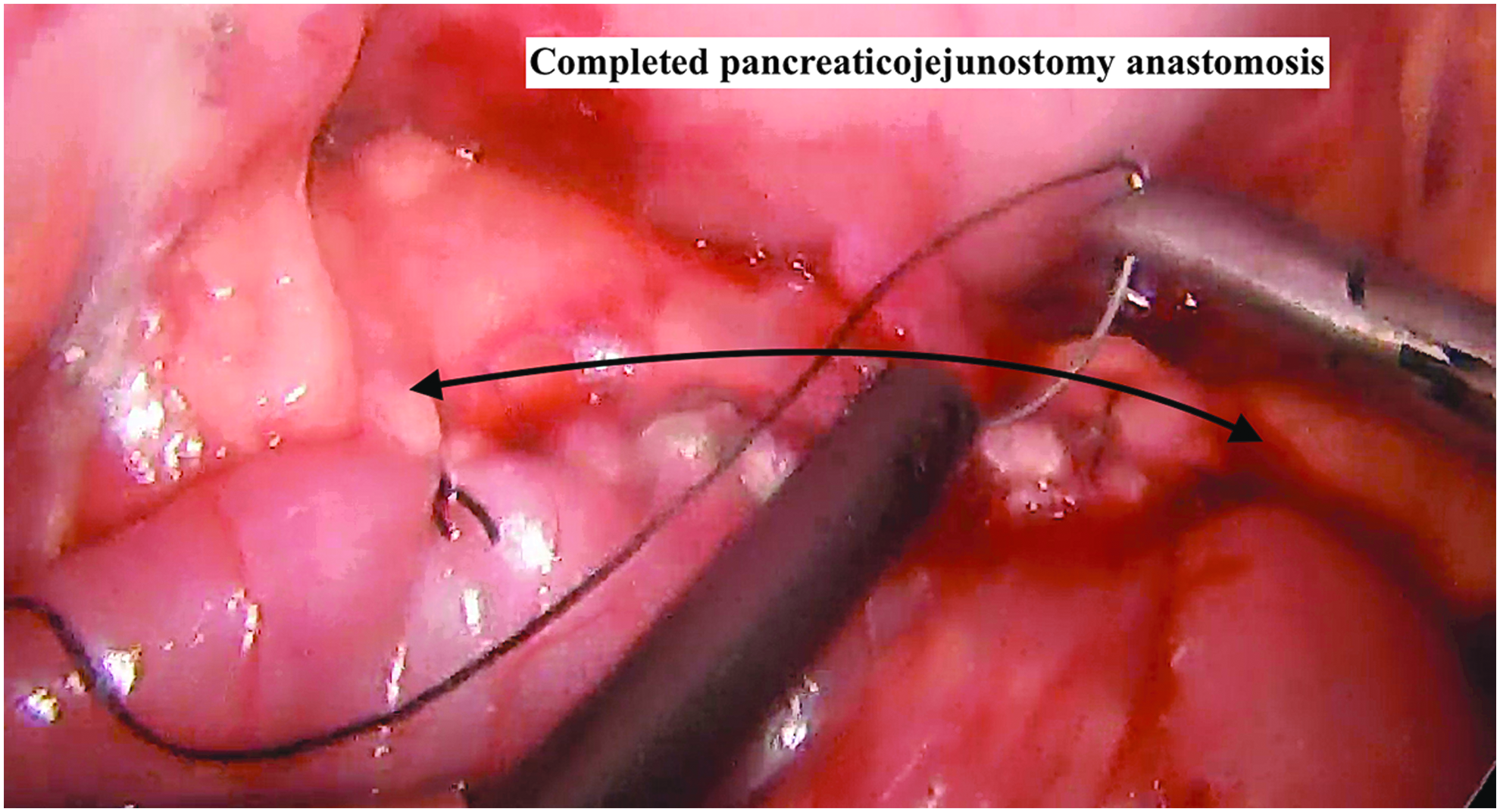
Completed pancreaticojejunostomy anastomosis.
The postoperative course was significant for an adynamic ileus, which resolved on postoperative day 5. She was discharged home on postoperative day 7 tolerating full diet. She was thriving and gaining weight appropriately, weighing 18 kg at the 3-month follow-up. Her serum glucose, amylase, and lipase were normal during follow-up visits. She had no further episodes of recurrent pancreatitis or hospital readmission for 4 years postoperatively.
Case 2
A 23-month-old female with a medical history significant for chromosome 14 translocation, agenesis of the corpus callosum, epilepsy, gastroesophageal reflux disease, optic nerve hypoplasia, and global developmental delay presented with obstructive jaundice and pancreatitis with a 6 mm stone in the common bile duct (CBD) evident on MRCP. Her prior operations included laparoscopic Nissen fundoplication and gastrostomy tube for gastroesophageal reflux disease and failure to thrive with revision in the first 9 months of life (Table 1 details chronology of other operations/interventions). She underwent ERCP and was found to have papillary stenosis for which she underwent sphincterotomy, endoscopic stone retrieval, and stent placement. She was discharged home and was admitted 1 month after her initial ERCP for recurrent pancreatitis. Second ERCP demonstrated two stones in the CBD with sludge in the bile ducts, which was cleared, and PD stent was placed. A laparoscopic cholecystectomy was performed after resolution of the acute phase of her illness in December of 2014. Despite operative intervention she continued to have recurrent episodes of abdominal pain with imaging consistent with chronic pancreatitis and CBD dilation along with dilated proximal hepatic ducts. An ERCP at this time revealed a dilated CBD with distal PD communication to the common channel and PD calculi (Fig. 7). After she developed ascending cholangitis she underwent laparoscopic hepaticoduodenostomy in an effort to avoid further episodes in April of 2015.

Endoscopic retrograde cholangiopancreatography of Case 2 shows dilated common bile duct with distal PD communication to the common channel and PD calculi at time of PD stent placement. PD, pancreatic duct.
Related to episodes of biliary obstruction or pancreatitis.
ERCP, endoscopic retrograde cholangiopancreatography; PD, pancreatic duct.
Despite this intervention and repeated ERCP and stone extractions, she continued to develop stones in the long common channel between her PD and distal CBD. Dilation of the PD had increased to 7 mm as identified on abdominal US and MRCP. In October of 2015, she underwent a lateral pancreaticojejunostomy (Puestow procedure) to alleviate the pancreatic ductal obstruction likely contributing to the recurrent episodes of pancreatitis. At the time, the patient weighed 12.1 kg.
Technique
A laparoscopic approach was attempted as described in Case 1; however, dense adhesions from prior operations made this approach unsuccessful. Conversion to laparotomy was performed through a transverse upper abdominal incision. The lesser sac was opened to expose the pancreas. US was used to identify the PD. Similar to Case 1, the pancreas was opened with electrocautery until the PD was exposed. The PD was opened over a length of 5 cm with electrocautery. The pancreatic stent placed by ERCP 2 days earlier was identified and left in place. The duct was noted to be freely draining pancreatic fluid. A Roux-en-Y limb for the pancreaticojejunostomy was created as described in Case 1, and the defunctionalized limb of the Roux-en-Y was brought up to the pancreas through the transverse mesocolon. A running anastomosis between the jejunum and the pancreas was performed with 4-0 PDS suture. A drain was left through the left upper quadrant near the anastomosis. She was discharged on postoperative day 10 tolerating tube feeds.
She was followed in clinic at 2, 3, and 6 months and 1 and 2 years postoperatively. At the 3-month follow-up her weight was 13.4 kg. At her 2-year follow-up, she continued to do well and had not been readmitted to the hospital since her Puestow nor had she had any episodes of pancreatitis. She was tolerating diet and tube feedings and was gaining weight adequately with normal pancreatic function.
Discussion
Chronic pancreatitis in children is a rare condition and often multifactorial in origin. Subclassification of ductal dilation is often characterized by etiology; (1) obstructive from anatomical abnormalities such as pancreatic divisum, annular pancreas, choledochal cysts, ampullary masses/papillae or trauma, (2) systemic from autoimmune conditions (systemic lupus erythematosus and immunoglobulin G-4 related pancreatitis) and cystic fibrosis, (3) toxic from drugs, and (4) hereditary from mutations in PRSS-1 and SPINK1 acquired in an autosomal dominant manner. 1 Regardless of etiology, the primary mechanism is increased luminal pressure from obstruction to flow of pancreatic secretions leading to significant ductal dilation and pain from ductal distension.
First described by Puestow and Gillesby, 7 lateral pancreaticojejunostomy (also known as Puestow's procedure) for the successful surgical treatment of chronic pancreatitis in children was first reported on by Scott et al. 8 Multiple authors have subsequently published their experience with the approach in children.
Resolution of pain following Puestow procedure remains the most important indicator of treatment success. A review of available literature by the American Gastroenterological Association reports rates of sustained pain relief to range from 60% to 70%. 9 Complete resolution of pain and symptoms was achieved in the cases reported in the current series without recurrence at 4 and 2 years, respectively. In addition both patients had preserved pancreatic endocrine and exocrine function with adequate weight gain. A similar trend has been reported by Palanivelu et al. in their series of 10 patients all of whom had normalization of pancreatic function with improved nutritional status postoperatively. 10 In addition, a systematic review by Yang et al. advocated early surgical intervention in patients with chronic pancreatitis in order to preserve pancreatic exocrine and endocrine function. 3 In addition to the Puestow procedure, the Frey procedure has also been described for treatment of chronic pancreatitis in children.2,11 This involves resection of or “coring out” the head of the pancreas and is useful for ductal dilation limited to the head of the pancreas. The choice of procedures is often guided by surgeon preference and experience, which was the case in the current series.
Although endoscopy for diagnosis and/or treatment is often the first-line intervention, surgery has been found to be superior in the management of painful pancreatic ductal dilation.3–5 In a randomized controlled clinical trial conducted by Dite et al. comparing endoscopic drainage to surgical intervention, surgery was found to be superior to at relieving pain and related symptoms at 1 year compared to endoscopic approaches (37% versus 14%, P < .05). 5 Cahen et al. demonstrated similar results with patients undergoing surgical drainage reporting superior pain relief at 24 months (25 versus 51, P < .001) and improved overall quality of life (P = .003) compared to endoscopic drainage. 4 It is important to note that although ductal decompression may obviate painful symptoms associated with chronic pancreatitis, disease resolution will ultimately depend on the cause associated with chronic pancreatitis.
Surgical intervention for chronic pancreatitis is uncommon in adults and even more infrequent in children. Most interventions in children are performed open, and one report employed the use of a robot to perform a lateral pancreaticojejunostomy in a teenager. 12 The first description of the use of the Puestow procedure in adults was by Glaser et al. 13 Zhang et al. published the largest cohort of laparoscopic Puestow in 2012 wherein they described the use of laparoscopy to treat chronic pancreatic ductal dilation in 4 children. 6 The operative times ranged from 103 to 154 minutes, and none of the patients had recurrent disease during the 3-month follow-up period. Our laparoscopic operative time was longer compared to the authors of the previous study possibly related to the smaller size of the patient and initial experience. Table 1 provides a comparison of preoperative, intraoperative, and postoperative characteristics of the 2 patients reported in this series.
Chronic pancreatitis remains a challenging disease to manage especially in children. Recurrent episodes refractory to medical and endoscopic treatment have been consistently shown to benefit from surgical intervention as in our experience. Surgical intervention remains infrequent due to its relative rarity being limited to specialized centers. In our small experience, both patients with pancreatic ductal obstruction managed with Puestow's procedure enjoy durable symptom and pain relief in long term.
Footnotes
Disclosure Statement
No competing financial interests exist.