
Abstract
Abstract
Background:
Since last two decades minimally invasive techniques have revolutionized surgical field. In 2003 Pomel first described laparoscopic pelvic exenteration, since then very few reports have described minimally invasive approaches for total pelvic exenteration.
Methods:
We report the 10 cases of locally advanced rectal adenocarcinoma which were operated between the periods from March 1, 2017 to November 11, 2017 at the Tata Memorial Hospital, Mumbai. All male patients had lower rectal cancer with prostate involvement on magnetic resonance imaging (MRI). One female patient had uterine and fornix involvement. All perioperative and intraoperative parameters were collected retrospectively from prospectively maintained electronic data.
Results:
Nine male patients with diagnosis of nonmetastatic locally advanced lower rectal adenocarcinoma were selected. All patients were operated with minimally invasive approach. All patients underwent abdominoperineal resection with permanent sigmoid stoma. Ileal conduit was constructed with Bricker's procedure through small infraumbilical incision (4–5 cm). Lateral pelvic lymph node dissection was done only when postchemoradiotherapy MRI showed enlarged pelvic nodes. All 10 patients received neoadjuvant chemo radiotherapy, whereas 8 patients received additional neoadjuvant chemotherapy. Mean body mass index was 21.73 (range 19.5–26.3). Mean blood loss was 1000 mL (range 300–2000 mL). Mean duration of surgery was 9.13 hours (range 7–13 hours). One patient developed paralytic ileus, which was managed conservatively. One patient developed intestinal obstruction due to herniation of small intestine behind the left ureter and ileal conduit. The same patient developed acute pylonephritis, which was managed with antibiotics. Mean postoperative stay was 14.6 days (range 9–25 days). On postoperative histopathology, all margins were free of tumor in all cases.
Conclusion:
Minimally invasive approaches can be used safely for total pelvic exenteration in locally advanced lower rectal adenocarcinoma. All patients had fast recovery with less blood loss. In all patients R0 resection was achieved with adequate margins. Long-term oncological outcomes are still uncertain and will require further follow-up.
Introduction
Pelvic exenteration for locally advanced rectal cancer is a well-established procedure. Mortality and morbidity associated with this procedure vary with institution and the number of cases per year.1–4 R0 resection is the most important criteria to predict survival, and median 5-year survival for locally advanced cancer after pelvic exenteration is 50% (range 31%–77%). For rectal cancer, laparoscopy is noninferior to open resection even after chemoradiotherapy (CTRT) with long-term outcomes as long as circumferential margin predicted by magnetic resonance imaging (MRI) is clear.5,6 In fact, the results of Colorectal cancer Laparoscopic or Open Resection (COLOR II) trial show superior outcomes for low rectal cancer in laparoscopy when compared with open group. Laparoscopy beyond total mesorectal excision (TME) is not well established5,7; however, selected centers with high volume and good results in lap TME do practice it. 8 Procedures, such as seminal vesicle excision and prostate shaving for locally advanced disease, have been described, but these may raise concern about positive margins and result in high recurrence rate.
Locally advanced rectal cancer in young males is not uncommon in Indian context. 9 Based on the trial of rectal cancer surgery in locally advanced rectal cancers after CTRT, performing a maximum operation with minimal approach can be associated with less blood loss, morbidity, and early recovery. 10 Also, psychological impact of small incision and quality of life cannot be underestimated. Very few studies are available describing laparoscopic pelvic exenteration, mainly in gynecological malignancies. 11 In India, total pelvic exenteration (TPE) is not widely accepted because of high surgical morbidity. We think that application of laparoscopic surgery could reduce this morbidity. In this study, we describe our experience in laparoscopic pelvic exenteration of lower rectal adenocarcinoma after CTRT in men.
Materials and Methods
We report the 10 cases of locally advanced rectal adenocarcinoma, which were operated between March 1, 2017, and November 11, 2017, at the Tata Memorial Hospital, Mumbai, and Maharashtra, India. Of 10 patients, 9 were male and 1 was female. MRI showed that all male patients had lower rectal adenocarcinoma with prostate involvement. The female patient had posterior fornix and uterine involvement. After confirmation of the diagnosis, local imaging (MRI pelvis), and metastatic workup (contrast-enhanced computed tomography of the thorax and abdomen), all patients received conventional neoadjuvant chemoradiotherapy (NACTRT). Of 10 patients, 7 also received additional neoadjuvant chemotherapy due to poor response to NACTRT. With preanesthetic fitness and informed consent, all patients underwent laparoscopic procedure (en bloc cystoprostatectomy + abdominoperineal resection + end sigmoidostomy + ileal conduit + V-Y plasty ± lateral pelvic lymph node dissection [LPLND]). Lateral pelvic node dissection was performed only when significant nodes were present on pre-CTRT MRI scan. All perioperative and intraoperative parameters were collected retrospectively from prospectively maintained electronic data (Table 1).
Demographic and Clinical Parameters
ASA, American Society of Anesthesiologists; BMI, body mass index; F/B Chemo, followed by chemotherapy; NACTRT, neoadjuvant chemoradiotherapy.
Surgical technique
Patient was placed in Lloyd-Davies position after epidural and general anesthesia. Small bolster was placed under buttocks. Trendelenburg position and right lateral tilt was given with shoulder support and chest belt (Supplementary Video; Supplementary Data are available online at www.liebertpub.com/lap).
Primary excision
With camera port at umbilicus, five ports were inserted (three 12 mm and two 5 mm) as shown in picture (Fig. 1). After bowel repositioning, the procedure began with medial-to-lateral dissection of rectosigmoid until the lateral abdominal wall. Inferior mesenteric artery was ligated and cut at the origin. Retrorectal space was dissected until origin of levator ani muscle. Then peritoneal cuts were made along bilateral external iliac vessels reaching up to medial umbilical ligament. Bilateral vas deferens was dissected and cut. Pararectal spaces were developed on both sides after mobilizing and medializing ureters. Paravesical spaces developed after dissecting obliterated umbilical artery in it (Fig. 2). Both spaces were connected after ligating superior and inferior vesicular vessels supplying the urinary bladder. On both sides white endopelvic fascia was identified. Bladder was mobilized from anterior abdominal wall and space of Retzius was dissected and connected with paravesical spaces. Puboprostatic ligament was cut, and then dorsal veins were clipped and cut with harmonic ace (Ethicon, Inc.) (Fig. 3). Urethra was cut with harmonic ace (Fig. 4). After cutting ureters distally, sigmoid colon was cut with the Echelon endostapler (Ethicon, Inc.).

Port placement.
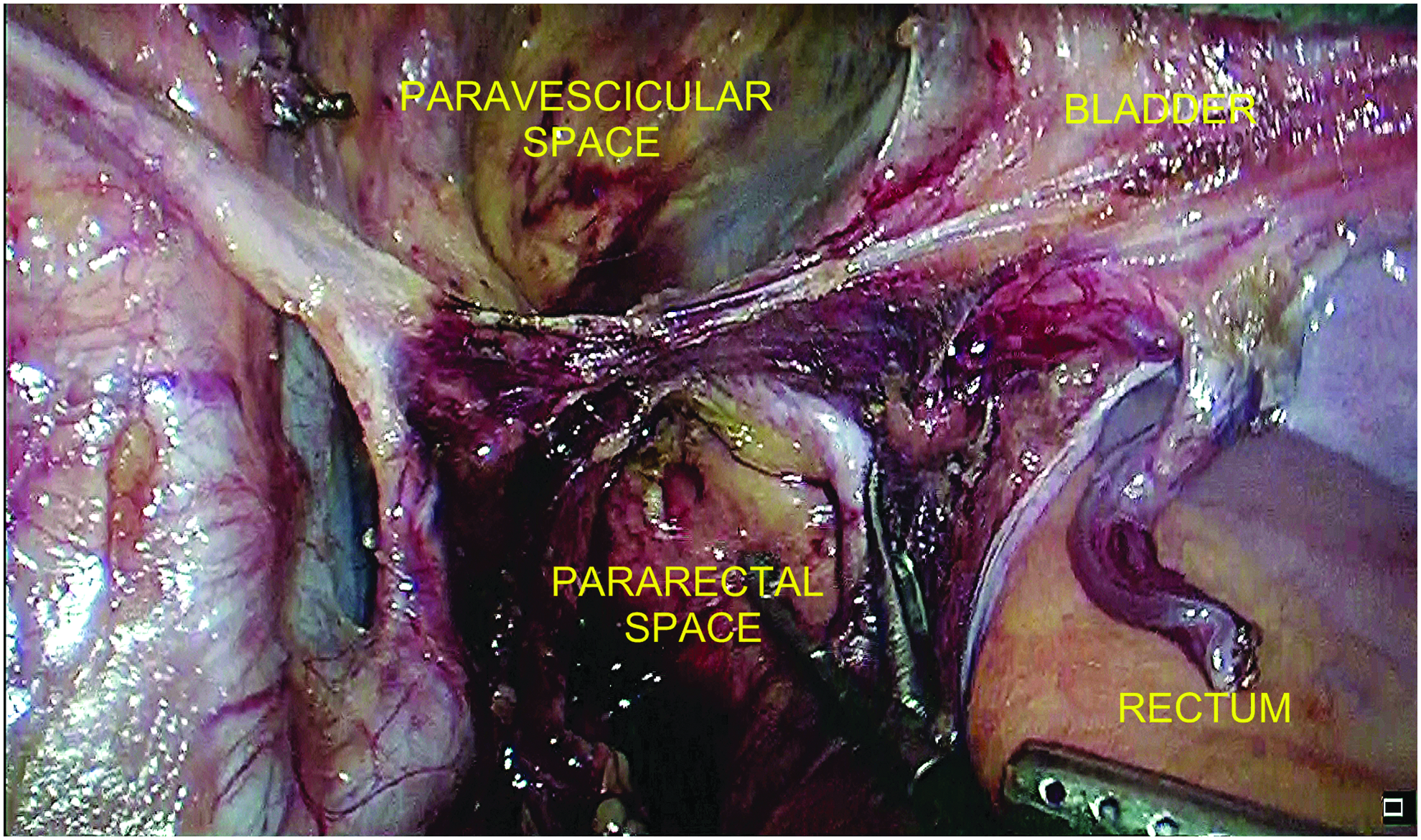
Left side dissection.
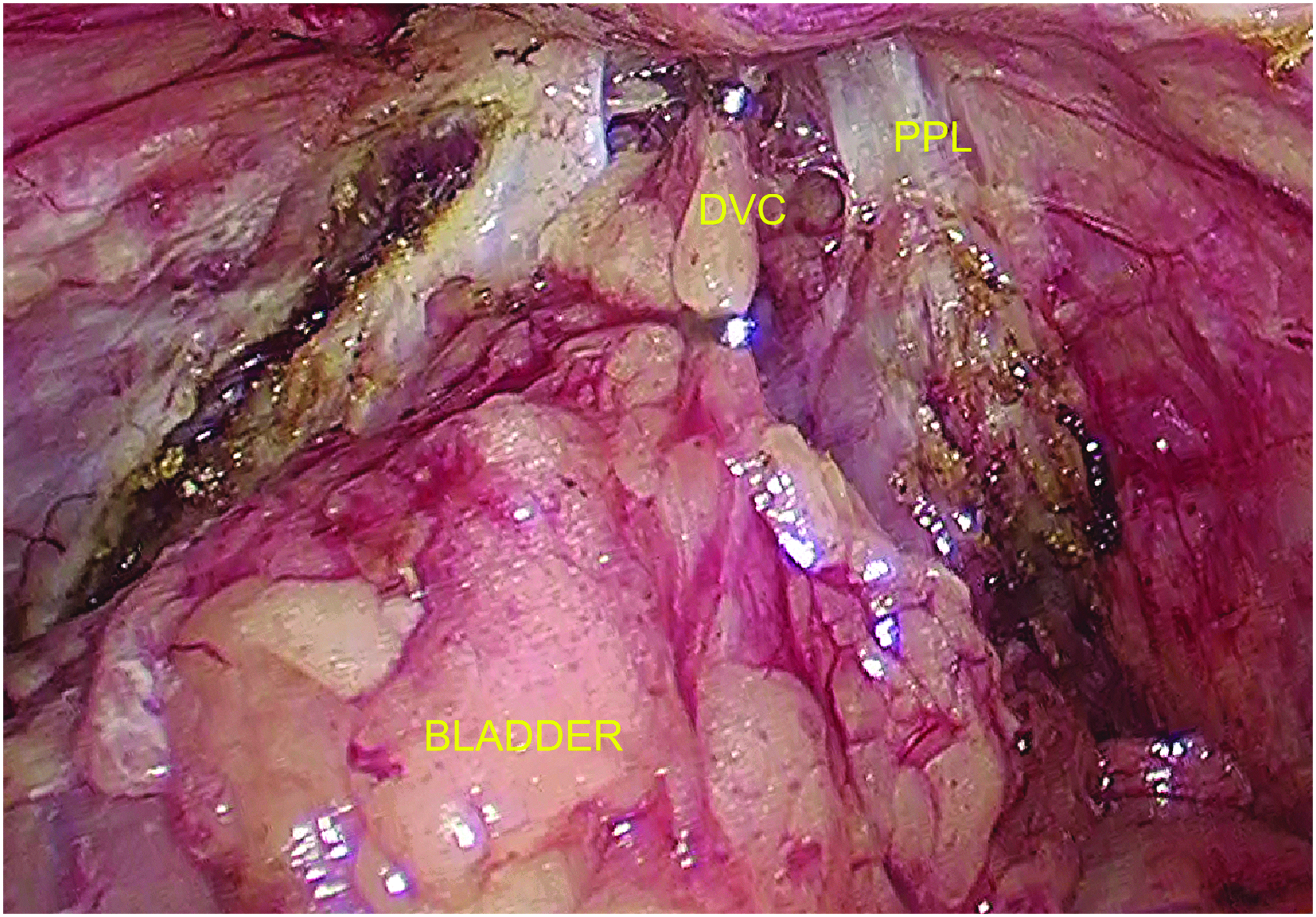
Space of Retzius dissection. DVC, dorsal vein; PPL, puboprostatic ligament.
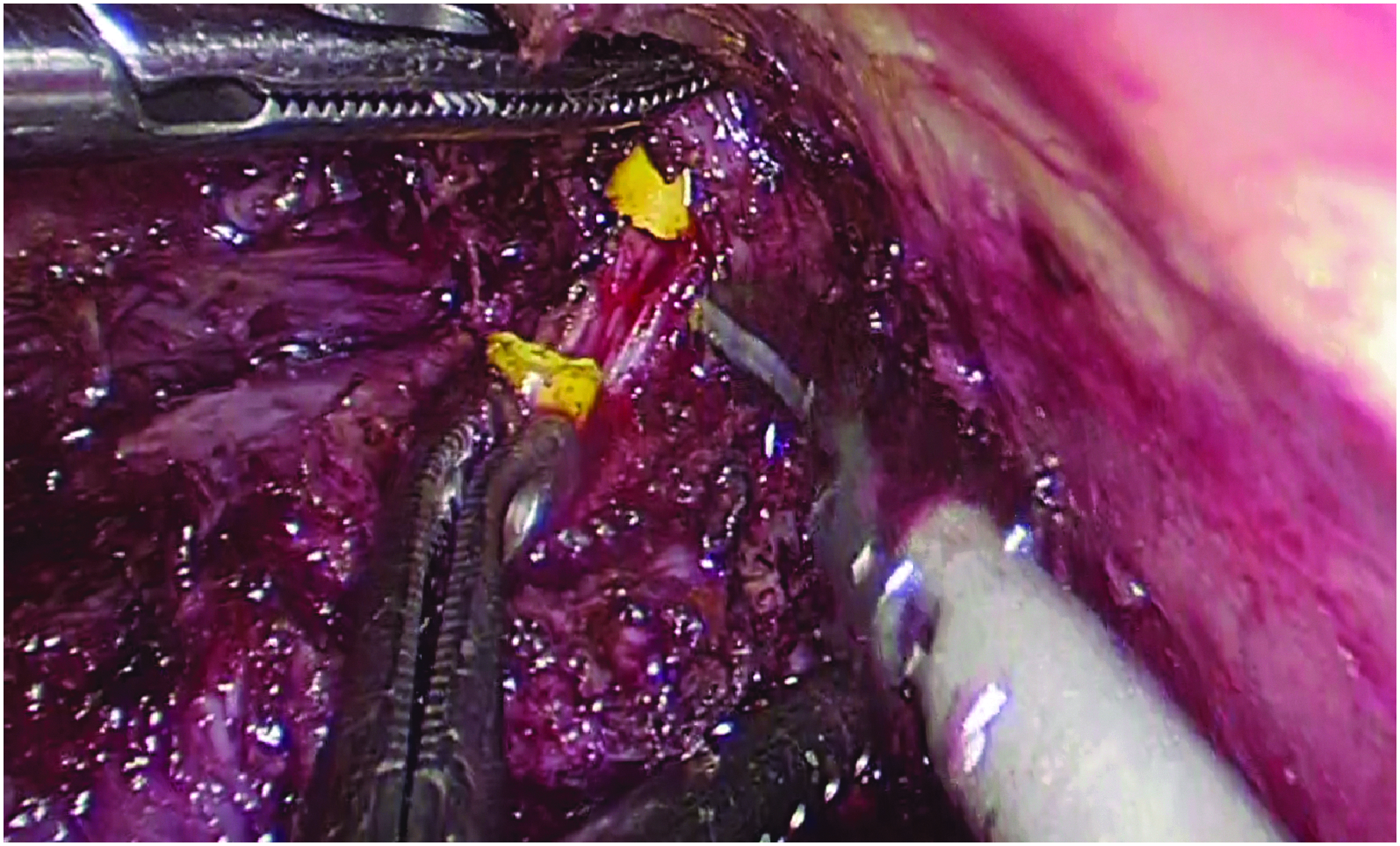
Urethra cut, posterior mucosa seen.
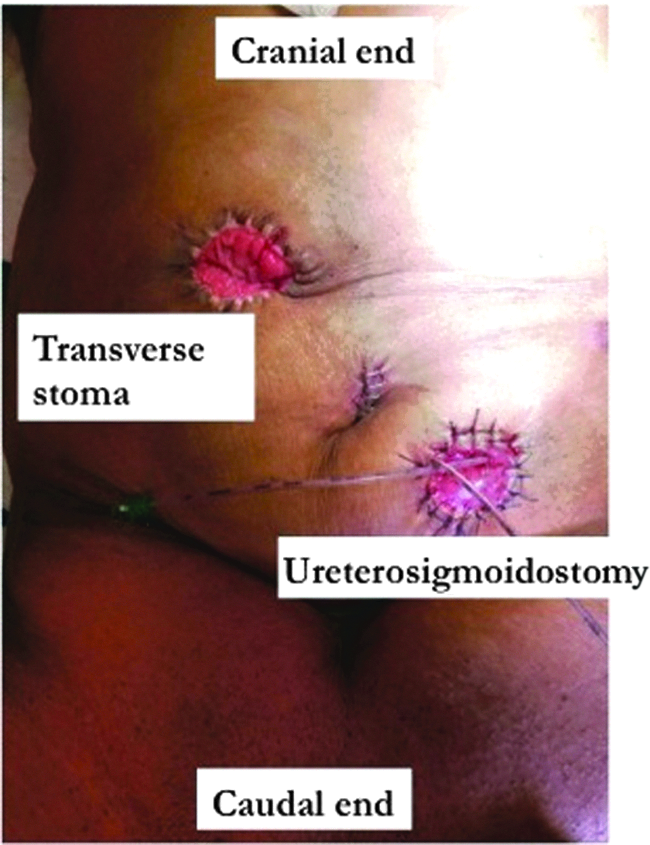
All patients underwent abdominoperineal resection with permanent sigmoid stoma. Elliptical incision was made around the anus; ischiorectal fossa was dissected bilaterally until levator ani was reached. Levator was cut on lateral pelvic wall and specimen was removed. Bladder reconstruction was done with ileal conduit in 7 patients, and as sigmoid conduit in 1 patient. Ileal conduit was constructed using Bricker procedure. Ureteral stents after conduit formation were left in place for 7–8 days compared with 5 days by urologists as small bowel may be included in radiation field. In early 2013, we had morbidity after delayed urinary leaks after CTRT. Ileal conduit harvest and ureteroileal anastomosis were performed through small infraumbilical midline incision (4–5 cm) after applying wound retractor in 8 patients (Fig. 5). End sigmoidostomy was done. In 1 patient, previous transverse stoma was retained and ureterosigmoid anastomosis was performed after stapling the sigmoid colon distal to the transverse stoma (Fig. 6). Lateral pelvic node was dissected in cases where nodes were significant on pre-CTRT MRI. Perineal defect was closed in all patients with either unilateral or bilateral V-Y plasty (Fig. 7).

Ileal conduit through infraumbilical incision.
Sigmoid conduit after stapling colon distal to transverse stoma. Previous transverse stoma retained.

Results
Nine male patients and 1 female patient with diagnosis of nonmetastatic locally advanced lower rectal adenocarcinoma were selected. MRI scan showed that all male patients had locally advanced disease with involvement of prostate and/or seminal vesicles. One female patient with uterine involvement was selected for posterior exenteration. All patients were operated with minimally invasive approach without any conversion to open laparotomy. LPLND was performed only when MRI after CTRT showed enlarged pelvic nodes. Eight patients underwent LPLND (unilateral, 6 patients; bilateral, 2 patients). All 10 patients received NACTRT, whereas 8 patients received additional neoadjuvant chemotherapy. Mean body mass index (BMI) was found to be 21.73 (range 19.5–26.3). Mean blood loss was 1000 mL (range 300–2000 mL). Mean duration of surgery was 9.13 hours (range 7–13 hours). One patient developed paralytic ileus, which was managed conservatively. One patient developed intestinal obstruction due to herniation of the small intestine behind the left ureter and ileal conduit. Exploratory laparotomy was performed for the same. The same patient developed acute pyelonephritis, which was managed with antibiotics. Mean postoperative stay was for 14.6 days (range 9–25 days).
Postoperative histopathology findings showed circumferential margins to be free of tumor in all cases (Table 2).
Intraoperative and Postoperative Parameters
CRM, circumferential resection margin; DRM, distal resection margin; LPLND, lateral pelvic lymph node dissection.
Discussion
It is clear that TPE is a major and morbid surgical procedure. Since first open TPE described by Brunschwig for palliative purpose, 12 indications of exenteration have changed completely. Although mortality rates have decreased considerably, morbidity is still high (13%–75%). 4 For the past two to three decades, laparoscopy and other minimally invasive surgical approaches such as robotic surgery have completely revolutionized the surgical field. Their main advantages are mainly small incision, less blood loss, better magnification, and fast postoperative recovery. Laparoscopic surgery has considerable learning curve and requires good teamwork. As experiences are gained, more advanced and complicated procedures are being performed with minimally invasive approaches.
Pomel et al. 13 described laparoscopic pelvic exenteration for recurrent cervical cancer. In 2011, Vasilescu et al. 14 described an entirely robotic TPE and extended lymphadenectomy for recurrent endometrial cancer. Puntambekar et al. 11 in a series of 16 patients reported low morbidity rate with 2 patients having subacute intestinal obstruction and 1with urinary leak. Yang et al. 15 reported short-term outcome of 11 cases of TPE for pelvic malignancies. They reported a significantly less blood loss and postoperative stay in the laparoscopic group. 15 All these case reports and retrospective case series have been described for gynecological malignancies. Mukai et al. described first case report of laparoscopic total pelvic exenteration (LTPE) with lateral pelvic node dissection. 16 Ogura et al. studied safety of LTPE in colorectal malignancies. 17 LTPE group had less blood loss and comparable complication rate, postoperative stay, and operation time.
In our center with high volume and experience of laparoscopic rectal resections with good oncological and safety profile, we also had experience with multivisceral resections of rectal cancer; hence, we progressed to minimally invasive rectal cancer resection.18,19
A recent study suggested that outcome of extended TME depends on the response to CTRT, 20 with poor responders having higher local recurrence rates in extended TME group compared with the beyond TME group. Also, results of salvage surgery for poor responders improve with additional chemotherapy.21,22 With experience, we feel that the best outcome in terms of local recurrence is better with TPE rather than with extended resection of rectum. With regard to lateral pelvic nodes, this is performed where preoperative MRI showed enlarged pelvic nodes. 23
All our male patients had disease involving prostate and seminal vesicles. Probably these are the best candidates for laparoscopic resection. We have not included patients with involved lateral margins or recurrent cancers due to concerns of ability to achieve free margins and long operative time. We have followed anatomical dissection of avascular spaces in pelvis and proper dissection with ligation of all named tubular and vascular structures. There was no conversion to open surgery; also, we did not encounter any significant bleeding due to systematic dissection. Although mean blood loss was 1033 mL (range 300–2000 mL), perineal dissection contributed to most of it. We think ligation of dorsal venous complex (DVC) is most difficult partly due to significant bleeding. We left this part for the end of pelvic dissection. Even if bleeding occurred, we packed this part with tape gauze; this bleeding was secured during perineal dissection in a supine position. Few reports have described control of DVC in a prone position. Prone position may be helpful in easy control of DVC. Also, we increased abdominal gas pressure, which helped in controlling DVC bleeding.
A patient with higher BMI may present more complexity for this laparoscopic procedure. In our study, mean BMI was 21.73, which is more on the leaner side. This could be due to selection bias.
Mean duration for the operation was 9 hours (range 7–13 hours), which was comparable to open TPE that we performed in our institute. One patient developed intestinal obstruction and required laparotomy due to internal herniation of small bowel from behind the sling formed by the left ureter and ileal conduit. We consider this due to inadequate retroperitonealization of ileal conduit and left ureter. It is most important to fix the left ureter to the retroperitoneum so that potential space for herniation can be obliterated. Two patients developed prolonged ileus, but managed conservatively. Our patients had a postoperative stay of 14.78 days (mean 9–25 days). With all this limited experience, we can say that T4 lower rectal cancer is amenable for laparoscopic exenteration safely. We think that good selection of patient and proper pelvic anatomical knowledge are keys to successful LTPE. Not to forget that good team and adequate laparoscopic experience are important factors. Ours is a tertiary care center with large volume of patients and experienced surgeons in laparoscopic pelvic procedures. It is obvious, that this is a retrospective, noncomparative, small case series, but we can conclude that laparoscopic TPE is a safe, less morbid procedure in selected group of patients of lower rectal cancer after CTRT.
Conclusion
Minimally invasive approaches can be used safely for TPE in carefully selected locally advanced lower rectal adenocarcinoma. All patients had fast recovery with less blood loss. In all patients, R0 resection was achieved with adequate tumor-free margins. But long-term oncological outcomes are still uncertain and require further follow-up.
Ethics Committee Approval
This study has been approved by the Ethics Committee and Institutional Review Board of the Tata Memorial Hospital, Mumbai.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.