
Abstract
Abstract
Background:
Thoracoscopic surgery for pediatric benign tumors is a common procedure. However, a large incision is needed to remove large tumors from the thoracic cavity. And, for intrapulmonary sequestration in lower lobe, it sometimes needs a large incision to ligate the aberrant vessels. A muscle-sparing axillar skin crease incision (MSASCI) has been introduced for thoracic open surgery, resulting in excellent aesthetic outcomes compared with a standard incision. We herein report the utility of this MSASCI technique in thoracoscopic surgery to remove large tumors from the thoracic cavity and to ligate the aberrant vessels in intrapulmonary sequestration in lower lobe.
Materials and Methods:
From 2014 April to 2016 March, we performed the MSASCI technique in thoracoscopic surgeries for 5 children.
Result:
Five cases were diagnosed as mediastinal masses (mature teratoma for 1 case, ganglioneuroblastoma for 2 cases, and extrapulmonary sequestration and intrapulmonary sequestration for 1 case each). The age at surgery was 32.0 ± 25.0 months (range 5–58 months). The size of the mediastinal mass was 9 × 5 × 5 cm, 4 × 3 × 3 cm, 5 × 5 × 2.5 cm, and 3 × 2.5 × 2 cm. For 4 other cases, except for the intrapulmonary sequestration case, the mass was resected under thoracoscopic surgery using only three or four 5-mm trocars and the mass was removed from the thoracic cavity using the MSASCI technique. For the intrapulmonary sequestration case, the aberrant vessels were resected under thoracoscopic surgery using only two 5-mm and one 12-mm trocars and the left lower lobectomy was performed using the MSASCI technique. All lesions were resected completely. No cases had surgical complications, none showed recurrence, and all cases demonstrated good cosmetic outcomes.
Conclusions:
Performing thoracoscopic surgery using a MSASCI technique is associated with good cosmetic outcome.
Introduction
R
A muscle-sparing axillar skin crease incision (MSASCI) was initially reported for open thoracic surgery in neonates by Bianchi et al. in 1998, 3 and this procedure has resulted in good cosmetic outcomes compared with standard thoracic surgical incisions, such as posterolateral incision. Furthermore, Kalman and Verebely extended this approach to children in 2002, 4 and Taguchi performed the MSASCI in 27 neonates and child patients and achieved excellent aesthetic outcomes. 5 In these reports, MSASCI was introduced for thoracic open surgery for infants and neonates with esophageal atresia, congenital pulmonary airway malformation, and lung pulmonary sequestration. However, this procedure has some technical difficulties associated with targets in the lower thoracic cavity such as ligation of feeding vessels of intrapulmonary sequestration and the resection of huge tumors developing into the lower thoracic cavity. Because the skin incision is made on the axillar skin crease, there are limitations concerning the surgical operation and surgical field visibility in such cases.
In laparoscopic surgery for large abdominal pediatric tumors, such as neuroblastoma, a Pfannenstiel incision is sometimes used to remove tumors from the abdominal cavity, resulting in good cosmetic outcomes.6,7 This procedure involves making an incision to remove a tumor on the lower abdominal wall, and the operation scar is hidden in the underwear. We expanded on this method and used the MSASCI technique to remove large thoracic tumors from the thoracic cavity in thoracoscopic surgery.
Materials and Methods
Thoracoscopic surgeries were performed using MSASCI in 5 patients from October 2014 to March 2016. Five cases were found to have mediastinal masses (mature teratoma for 1 case, ganglioneuroblastoma [GNB] for 2 cases, and extrapulmonary sequestration and intrapulmonary sequestration 1 case each).
The MSASCI procedure in our institution has already been reported by Taguchi et al. 5 The patient was placed in the left or right lateral position with one-lung ventilation using a Fogarty embolectomy catheter. The upper arm was extended to about 130°, drawn forward, and placed on an arm rest. Initially, thoracoscopic surgery was performed under positive pressure pneumothorax using one 5-mm port for the video laparoscope and two or three additional 5-mm ports. Resection of the tumor was performed using a 5-mm vessel sealing device. In the case with the extrapulmonary sequestration, the aberrant vessel was ligated using a 5-mm clip. The tumor was removed from the thoracic cavity through the MSASCI. A skin incision was made just on the axillar skin crease, and the pectoralis major and latissimus dorsi muscles were retracted superiorly and medially, respectively. The incision was deepened, and the axillary fat pad and lymph nodes were pushed upward. The anterior serratus muscle was split along its fibers through the third or fourth intercostal space (ICS). The thoracic cavity was entered through the ICS, and then the tumor was removed as usual with a bag (Fig. 1).
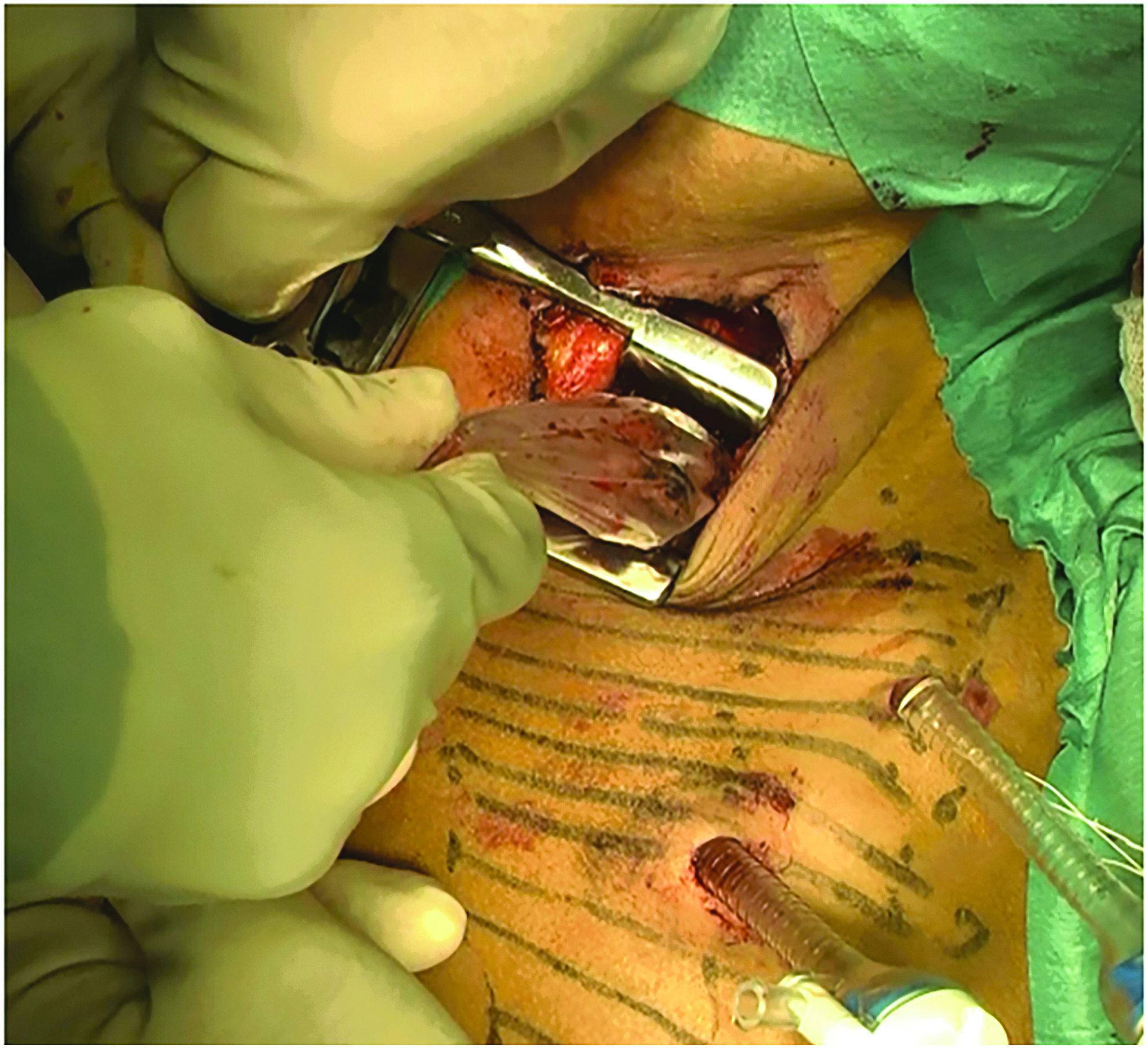
In case 2, the tumor was removed from the thoracic cavity through the MSASCI. MSASCI, muscle-sparing axillar skin crease incision.
This study was performed in accordance with the Ethical Guidelines for Clinical Research published by the Ministry of Health, Labour and Welfare of Japan on July 30, 2003 (revised 2008), and complied with the 1964 Declaration of Helsinki (revised 2008). This study was approved by the Ethics Committee in our institution (28-478).
Results
The thoracoscopic surgeries using MSASCI were performed in 5 patients. The clinical data for the patients treated with this procedure are shown in Table 1. In case 1, the mature teratoma originated from the thymus gland and occupied the median side of the thoracic cavity (Fig. 2). In case 2 and case 5, the GNB was located at the paraspinal region (Fig. 3). In case 4, the intrapulmonary sequestration and feeding vessels were located at the left lower lobe (Fig. 4).

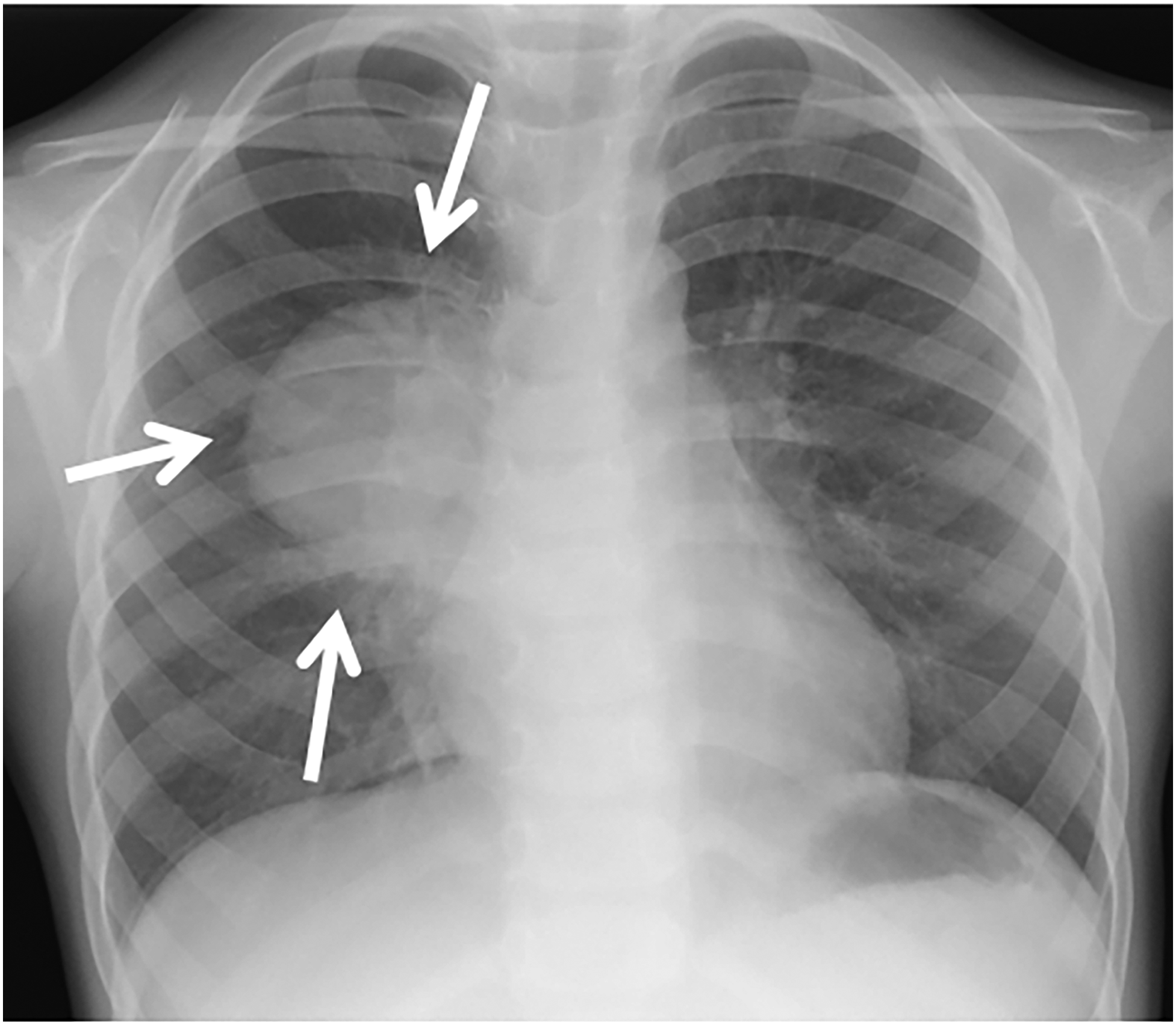
X-ray image showing the mediastinal ganglioneuroblastoma in case 2 (indicated by white arrows).
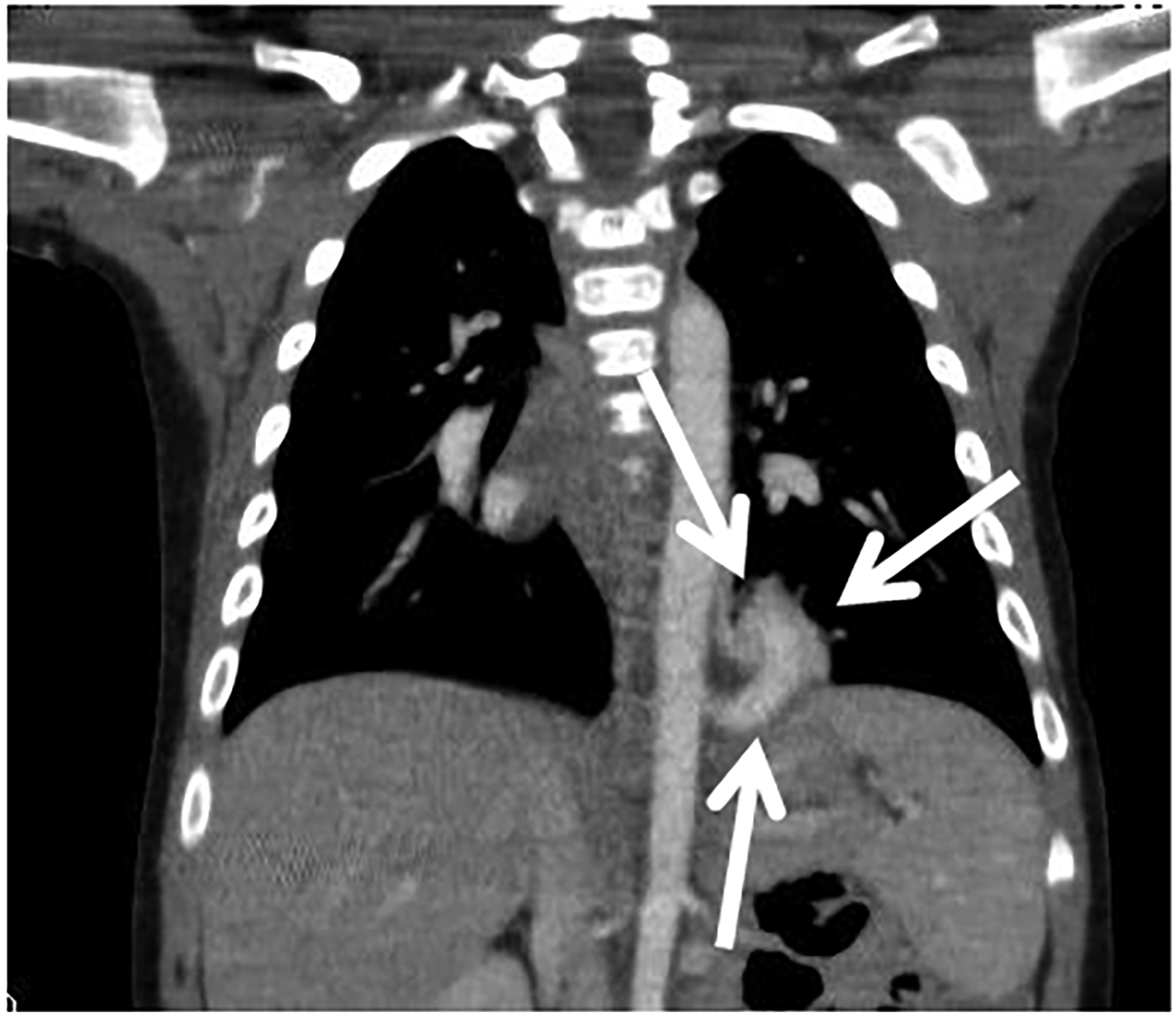
Coronal CT image showing the intrapulmonary sequestration and feeding vessels in case 4 (indicated by white arrows). The feeding vessels are located on the diaphragm.
CR, complete resection; EPS, extrapulmonary sequestration; GNB, ganglioneuroblastoma; IPS, intrapulmonary sequestration; MSASCI, muscle-sparing axillar skin crease incision; MT, mature teratoma.
At the time of the operation, the patients' ages were 32.0 ± 25.0 months (range 5–58 month) and their body weight was 12.1 ± 4.6 kg. Four of 5 cases were left sided. The size of the mediastinal mass was 9 × 5 × 5 cm, 4 × 3 × 3 cm, 5 × 5 × 2.5 cm, and 3 × 2.5 × 2 cm. For the 4 other cases, except for the intrapulmonary sequestration case, the mass was resected under the thoracoscopic surgery using only three or four 5-mm trocars, and the mass was removed from the thoracic cavity using the MSASCI technique. For the intrapulmonary sequestration case, the aberrant vessels were resected under thoracoscopic surgery using only two 5-mm and one 12 mm trocars and the left lower lobectomy was performed using the MSASCI technique. The operation time, including that for the MSASCI procedure, was 200.4 ± 78.1 minutes. All five tumors were successfully resected completely, and no recurrence has yet been reported since these operations. Figure 5 shows the excellent cosmetic outcomes of each case after surgery.
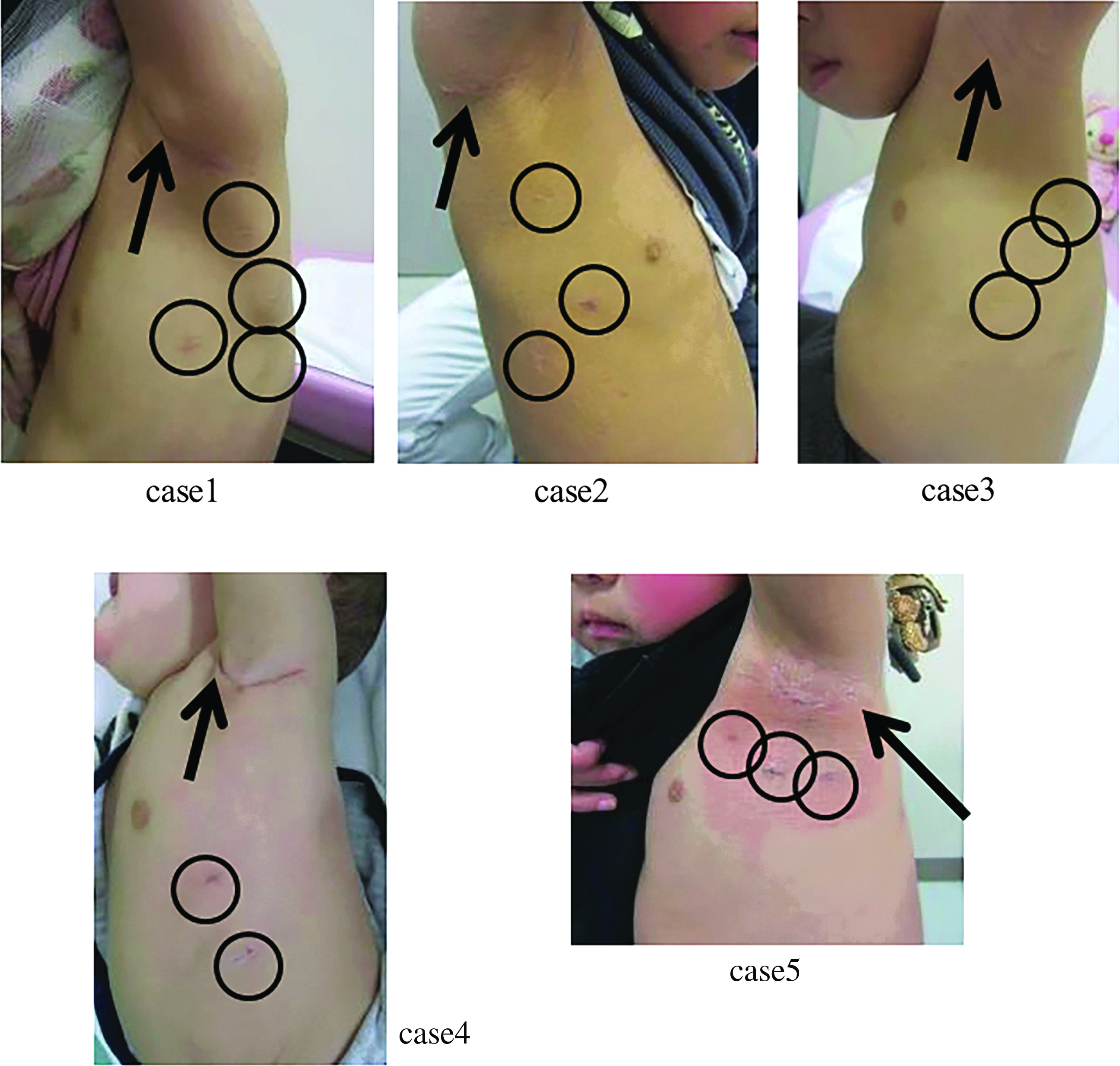
The excellent cosmetic outcomes of the 5 cases at 9 months, 4 months, 2 years, 1 month, and 1 month after the operation, respectively. The round marks show the scar of the trocar, and the arrows show the scar of the MSASCI. MSASCI, muscle-sparing axillar skin crease incision.
Discussion
Thoracoscopic surgery for a mediastinal tumor was previously reported, and the tumor was removed through an enlarged port site.2,8 However, the larger the tumor, the larger the scar of the port. This correlation negates the cosmetic advantages of thoracoscopic surgery for large tumors. The MSASCI technique has been reported to result in good cosmesis of open thoracic surgery for children. In this study, we extrapolated this technique for thoracoscopic surgery to remove a tumor from the thoracic cavity and achieved good cosmetic outcomes.
Previously, the majority of patients undergoing open thoracic surgeries using the MSASCI technique without thoracoscopic procedures have been <1 year of age.3–5 Kalman and Verebely reported that 16 of 26 cases were neonates, and Taguchi et al. reported that 23 of 27 cases were infants and neonates. One reason for this predominance of infants is that a child's skin hardens with age, making thoracic open surgery difficult to perform for lower ICSs in older children. However, with the current surgical technique described in this report, a MSASCI technique was only used to remove the tumor, as we entered the thoracic cavity through the upper ICSs. This approach makes this technique easy to perform in older children. Furthermore, open thoracic surgeries using the MSASCI technique without thoracoscopic procedures have been associated with complications of wound disruption and transient arm paralysis in a small number of patients, necessitating monitoring of the peripheral blood pulse and oxygen saturation on their hand. 5 Using the current technique, the duration of performing MSASCI technique is not very long, as this incision is only used to remove the tumors from the thoracic cavity. Therefore, the risk of these complications may be reduced.
If a tumor preoperatively and definitively diagnosed as a benign tumor, it may be able to be removed through the incision for a 5-mm port after cutting the tumor into several pieces. 2 However, the tumor in case 1 was a mature teratoma, and the boundary between the tumor and the thymus gland was unclear. In addition, for immature teratoma cases, the tumor sometimes shows recurrence. 9 We were able to determine the complete resection using the resected sample because the tumor was removed en bloc in our case. In addition, ganglioneuroblastoma, nodular (GNBn) is a rare subset of GNB. It is a heterogeneous tumor showing components of neuroblastoma as the malignant component on a ganglioneuroma or GNB background. 10 The clinical outcome of GNBn depends on the neuroblastoma component. Therefore, en bloc resection can aid in achieving the accurate pathological examination of GNB cases.
In conclusion, performing thoracoscopic surgery using a MSASCI technique is associated with a good cosmetic outcome. This technique is, therefore, expected to become one of the approaches when performing thoracoscopic surgery for large thoracic benign tumors and intrapulmonary sequestration of lower lobe in children.
Footnotes
Acknowledgment
The English used in this article was reviewed by Brian Quinn (Editor-in-Chief, Japan Medical Communication).
Disclosure Statement
No competing financial interests exist.