
Abstract
Abstract
Introduction:
Patients with neurogenic bladder frequently also have bowel dysfunction and a simultaneous urologic and colorectal reconstruction is possible. We present our experience with combined reconstructive procedures using robot-assisted laparoscopy, and demonstrate the utility of a minimally invasive approach that considers both the bowel and bladder management of these patients.
Methods:
We retrospectively reviewed all patients who underwent combined bowel and urologic reconstruction at our institution since the start of our multidisciplinary robotic program.
Results:
Seven patients were identified in our cohort with a mean age of 6.4 years (3.8–10.1 years). Six patients had myelomeningocele and 1 had caudal regression. Malone appendicostomies were placed in all 7 patients. A split appendix technique was used as a conduit in 5 patients, in situ appendix in 1, and neoappendicostomy with cecal flap in 1. Six patients had a Mitrofanoff appendiceal conduit created, while 1 patient had a sigmoid colovesicostomy for urinary diversion. Five patients required bladder neck repair. One patient had stenosis of the Mitrofanoff and one patient had an anastomotic leak of the sigmoid anastomosis. The average operating time was 526 minutes (313–724 minutes). The median length of stay (LOS) was 5 days (4–7 days), excluding one outlier who suffered an anastomotic leak and had an extended LOS (50 days). All patients who underwent continent bladder reconstruction are dry on their current catheterizing regimen, 6/7 are clean with antegrade flushes.
Conclusion:
Patients with neurogenic bladder often have coexisting bowel dysfunction, which provides an opportunity to reconstruct both organ systems simultaneously and achieve social urinary and bowel continence. Before committing to any intervention, the surgeon should consider both the urologic and gastrointestinal needs of the patient, and perform the needed procedures simultaneously. We describe a number of combined operations aimed at bowel and bladder management that can be performed safely using robot-assisted laparoscopy.
Introduction
Children born with neurogenic bladder as a result of myelomeningocele or caudal regression syndrome often have difficulties related to both urinary and fecal incontinence. The psychosocial sequelae of incontinence in childhood include increased depressive symptoms, poor self-image, and difficulty with peer relationships in adolescence and beyond,1,2 and thus getting such patients clean and dry are key goals. A subset of these patients benefit from continent urinary diversion, which permits intermittent bladder drainage, social continence, and self-reliance. Likewise, the neurologic abnormalities that result in poor urinary function may also cause dysfunction of the gastrointestinal tract. In patients with coexisting bladder and bowel dysfunction, a simultaneous urologic and colorectal reconstruction is possible, and also may allow for the sharing of valuable tissue. These techniques are well described using a laparoscopic technique, but less is known about the use of robotic-assisted surgery for these reconstructive procedures.3,4
Herein we present our experience with combined reconstructive procedures using robot-assisted laparoscopy and demonstrate the utility of a minimally invasive approach that considers both the patient's bladder and bowel management.
Methods
We retrospectively reviewed all patients who underwent combined urologic and gastrointestinal reconstruction at our institution since the start of a multidisciplinary robotic program in 2016. Data captured included age and weight at the time of surgery, diagnosis, the procedure performed, and surgical utilization of the appendix. Intraoperative records were reviewed to determine the length of key steps in the robotic procedure and the overall length of the case. Operative videos and surgical technique were reviewed and operative results analyzed. We defined dry of urine as having one or fewer urinary episodes weekly or no leakage between catheterizations (clean of stool meant having one or fewer episodes of fecal incontinence per week). Statistical analysis of key outcome variables was performed using Microsoft Excel 2010 (14.0.7015.1000), Microsoft Corporation. This study was approved by the Institutional Review Board at Nationwide Children's Hospital.
Robotic configuration
The daVinci Si Surgical System (Intuitive Surgical, Sunnyvale, CA) robot was used in all cases. In 5 patients, the robotic setup was as follows: 12 mm camera port through the umbilicus, 8 mm robotic port through the right-upper quadrant, 8 mm robotic port through the right-lower quadrant, 8 mm robotic port through the left mid-abdomen in the anterior axillary line, and a 12 mm left-upper quadrant assist port (Fig. 1). One patient had a similar setup without the right lower quadrant port. The last patient who underwent a sigmoid resection had the 12 mm camera through the umbilicus, an 8 mm robotic port through the right mid-abdomen at the level of the umbilicus, 8 mm robotic port through the right lower quadrant, a robotic port through the left mid-abdomen at the level of the umbilicus, and a 12 mm assist port through the left upper quadrant.
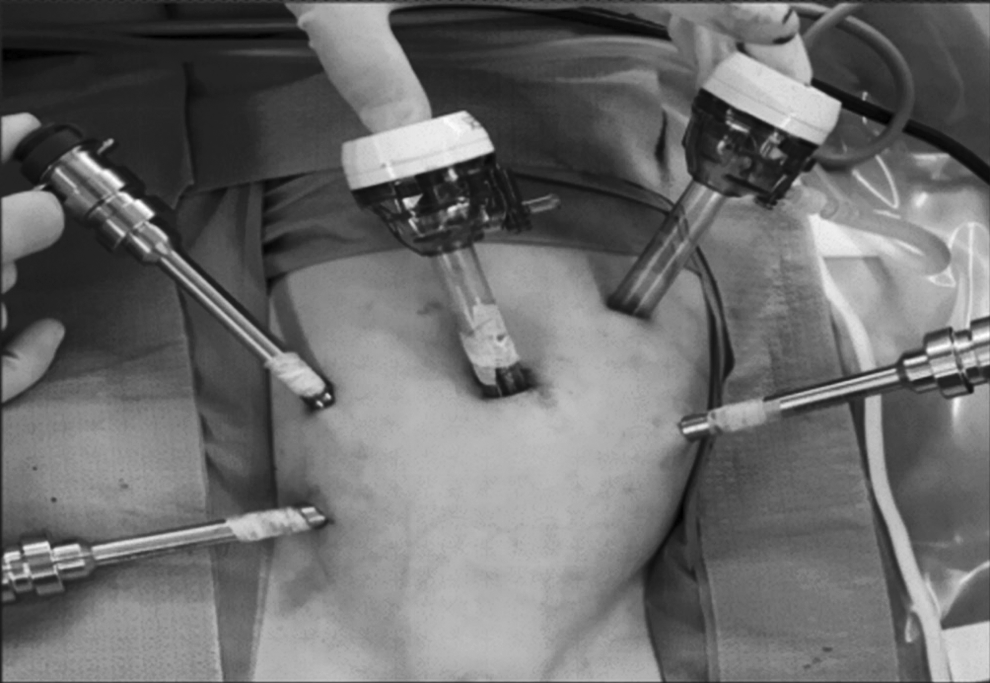
Robotic port placement for combined urologic and colorectal reconstructive procedures. A 12 mm camera port is placed through the umbilicus, followed by 8 mm robotic ports in the right-upper quadrant, right-lower quadrant, and the left mid-abdomen in the anterior axillary line. A 12 mm assist port is placed in the left-upper quadrant.
Results
Seven (4 male and 3 female) patients underwent both Malone appendicostomy and genitourinary reconstruction for the management of their fecal and urinary incontinence over the study period. The median age at the time of reconstruction was 5.4 years (range 3.8–10.1 years). The median weight percentile was 64.1 (range 0.1–95.1). The underlying diagnosis was myelomeningocele in 6 patients (86%) and caudal regression syndrome in 1 patient (14%). Median follow-up was 0.8 years (range 0.3–1.6 years).
Table 1 illustrates our patient characteristics and their operative details. The appendicostomy technique used in these patients was an in situ appendicostomy in 1 patient (14%), split appendix in 5 patients (71%), and neoappendicostomy using a cecal flap in 1 patient (14%). Six patients had a Mitrofanoff created using the appendix (5 split and 1 in situ), and 1 patient had a colovesicostomy created from sigmoid colon. Five patients had a bladder neck reconstruction at the time of the procedure. The right lower quadrant and the umbilicus were the sites of exteriorization for the Malone appendicostomy and Mitrofanoff appendicovesicostomy, respectively, in 6 patients. The remaining patient's umbilicus was used for the Malone appendicostomy and the left upper quadrant used for the colovesicostomy.
Patient Characteristics, Operative Details, Complications, and Functional Outcomes of Patients Who Underwent Combined Robot-Assisted Laparoscopic Urologic and Colorectal Reconstruction
Total OR time includes time needed for induction of anesthesia, laparoscopic dissection before docking, and closure.
CRS, caudal regression syndrome; EBL, estimated blood loss; MMC, myelomeningocele; LOS, length of stay; LUQ, left upper quadrant; NA, not applicable; RLQ, right lower quadrant; VP, ventriculoperitoneal
The overall median console time was 301 minutes (range 145–479 minutes) and the median total operating room time was 527 minutes (range 313–724 minutes). The median estimated blood loss was 25 cc (range 10–100 cc). There were no intraoperative complications or conversions to laparoscopic or open technique. The median hospital length of stay (LOS) was 5 days (range 4–7 days), with the one outlier excluded (50 days). Complications occurred in 2 patients: 1 patient had stenosis of the Mitrofanoff stoma, and 1 had a colo-colonic anastomotic leak, which required exploratory laparotomy for repair and subsequent development of a colocutaneous fistula. At present, 6/6 (100%) patients who underwent continent bladder reconstruction are dry and the remaining has a urinary stoma, and 6/7 (86%) patients are clean on their antegrade enema regimen.
Discussion
The utility of robotic-assisted laparoscopic surgery has been well described in a variety of fields since its first clinical description in the 1990s. While it has gained popularity and become widely accepted in the treatment of many adult surgical conditions, its use in the pediatric population has been more slowly adopted. The aim of our study was to review our institutional experience with robotic-assisted laparoscopy in combined urologic and gastrointestinal procedures and describe the utility of a collaborative approach to these complex patients.
All patients in our series were incontinent of both urine and stool as a result of myelomeningocele (n = 6) or caudal regression syndrome (n = 1) causing neurogenic bladder and bowel. The goal of surgical intervention in all cases was to create conduits to the bladder and large intestine that allow the child or parent to perform intermittent catheterization of the bladder and to instill enema flushes to the large intestine, allowing the child to be socially continent of urine and stool. Both laparoscopic and robotic techniques for creation of Mitrofanoff appendicovesicostomy5–11 and Malone appendicostomy4,12–15 are well described. There are less data on performing the two procedures simultaneously, however.3,16
Our series demonstrates that performing simultaneous urologic and colorectal reconstruction can be performed safely using robotic-assisted laparoscopy. We experienced no intraoperative complications. Postoperative complications were seen in 2 patients, which are well described in nonrobotic approaches.8,10 Mitrofanoff stenosis, which was seen in 1 (14%) of our patients, is not well understood given the paucity of robotic experience in the literature to date, 6 but the rate of stenosis after open Mitrofanoff creation has been reported to approach 20%.17,18 The second and more serious complication in our series was a child who experienced anastomotic leak after sigmoid resection with colovesicostomy and Malone appendicostomy. This child returned to the operating room on postoperative day #4 for exploratory laparotomy and repair of sigmoid anastomosis, and experienced an extended LOS due to, in part, complications related to his VP shunt.
There are significant advantages to performing these procedures simultaneously whenever possible in children (Table 2). For one, performing both procedures simultaneously saves one additional abdominal procedure and anesthetic event. If the child is viewed through a strictly “urologic” or “colorectal” lens, this advantage would not be realized. This collaborative approach allows for the postoperative days to be overlaid in both cases. Second and more importantly, it permits the sharing of tissues that can be utilized in the management of both urologic and colorectal dysfunction. In our cohort of patients, 5 were able to successfully undergo the split appendix technique. In 1 patient, the sigmoid colon was used for the bladder conduit. The removal of his redundant segment of colon in addition to the appendicostomy resulted in a significant improvement in his stooling symptoms. 19 The benefit of performing these procedures simultaneously and sharing tissue used for the reconstruction underscore the benefits to the collaborative approach to the management of these complex pediatric patients. 20
Advantages of a Collaborative Approach to Children with Neurogenic Bladder and Bowel
We recognize several limitations based on the retrospective design and relatively small numbers of our study. Data collection was performed using patient records collected for the purposes of clinical care, and thus its accuracy is dependent on correct input of data. In addition, we do not have a similar cohort of patients who underwent laparoscopic or open approaches by which to compare the intraoperative and postoperative complications. Ultimately, more studies are needed to further define the role of robotic-assisted laparoscopic surgery in the urologic and colorectal management of pediatric patients and to better understand the benefits and drawbacks compared to laparoscopic and open surgical techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.