
Abstract
Abstract
Introduction:
Surgical management of the high urogenital sinus (UGS) is challenging. Presence of a short urethra is a contraindication for UGS mobilization as this is likely to affect urinary continence. In addition, vaginal reconstruction of the high suprasphincteric confluence is complex and prone to complications and failure.
Methods:
This study included 7 girls who underwent a laparoscopically assisted vaginal pull-through in the past 2 years. All cases included were diagnosed with congenital adrenal hyperplasia (CAH), with a high UGS, and a short urethra of ≤15 mm above the confluence. Patients were preoperatively assessed by genitography. Mobilization of the vagina was pursued until the confluence became visible and the vaginal caliber tapered off at its junction with the urethra. The connection was sutured or clipped and divided. Uterine round ligaments were divided to allow delivering the vagina to the perineum with minimum tension. The tract for the pull-through was created and the vagina was pulled outside and sutured to the perineal skin. Good vaginal mobilization allowed a direct perineal anastomosis without skin flap augmentation of the vaginal wall. Clitoroplasty and labiaplasty were deferred.
Results:
Mobilization of the vagina was possible in all cases attempted, without injuries to the adjacent pelvic structures. Calibration and dilatation started 2 weeks postoperatively. At 12-month follow-up, all the patients had a patent vagina with good caliber, and were able to retain urine without dribbling.
Conclusion:
The laparoscopically assisted vaginal pull-through approach provides optimal exposure, facilitates vaginal dissection, separation from the urethra, and avoids injuries to the urinary structures. This allows vaginal reconstruction without tension.
Introduction
T
Complete separation of the vagina from the UGS with a pull-through vaginoplasty, as proposed by Hendren and Crawford, 1 is logically the best solution to a high vaginal confluence, where separation of the vagina from the urethra, vaginal mobilization, and anastomosis to the perineum are the main steps. Braga and Salle 9 recommended it only when the UGS is longer than 3 cm. Fortunately, this complex situation is found in only ∼5% of patients with virilized congenital adrenal hyperplasia (CAH). This high confluence is more commonly seen in pure UGS abnormalities.6,10 The critical and most technically demanding aspect of a pull-through vaginoplasty is the separation of the anterior wall of the vagina from the urethra and bladder neck. There is no obvious plane of dissection perineally, and great caution must be exercised to avoid injury to the urinary tract and its sphincteric mechanisms. This area is also the most difficult to expose, with the potential for a stricture, fistula, or a retained diverticulum. 4 Furthermore, this is an area of complex nerve supply for the vagina and urethra. Most surgeons position the patient in the prone or lithotomy position. The anterior sagittal transanorectal approach or ASTRA (division of the anterior rectal wall) provides excellent exposure in the prone position for the separation of the vagina, and certainly could be considered for those patients with a very high vaginal confluence. 11
The aim of this study was to circumvent these complexities and difficulties by performing the pull-through laparoscopically, with superior exposure and magnification, allowing preservation of all the important structures.
Patients and Methods
Cases were prospectively included with the intention to produce this report. The clinical records of these 7 patients were retrospectively reviewed. The indications for surgery, operative technique, postoperative complications, and the outcome were recorded. The follow-up period for the reported cases was at least 12 months after surgery. All patients were evaluated by genitography before the definitive repair, and the length of the urethra and vagina were determined. 12 Cases included had a preconfluence urethra of <15 mm. We also assessed the confluence depth from the perineal skin surface 6 (Fig. 1).
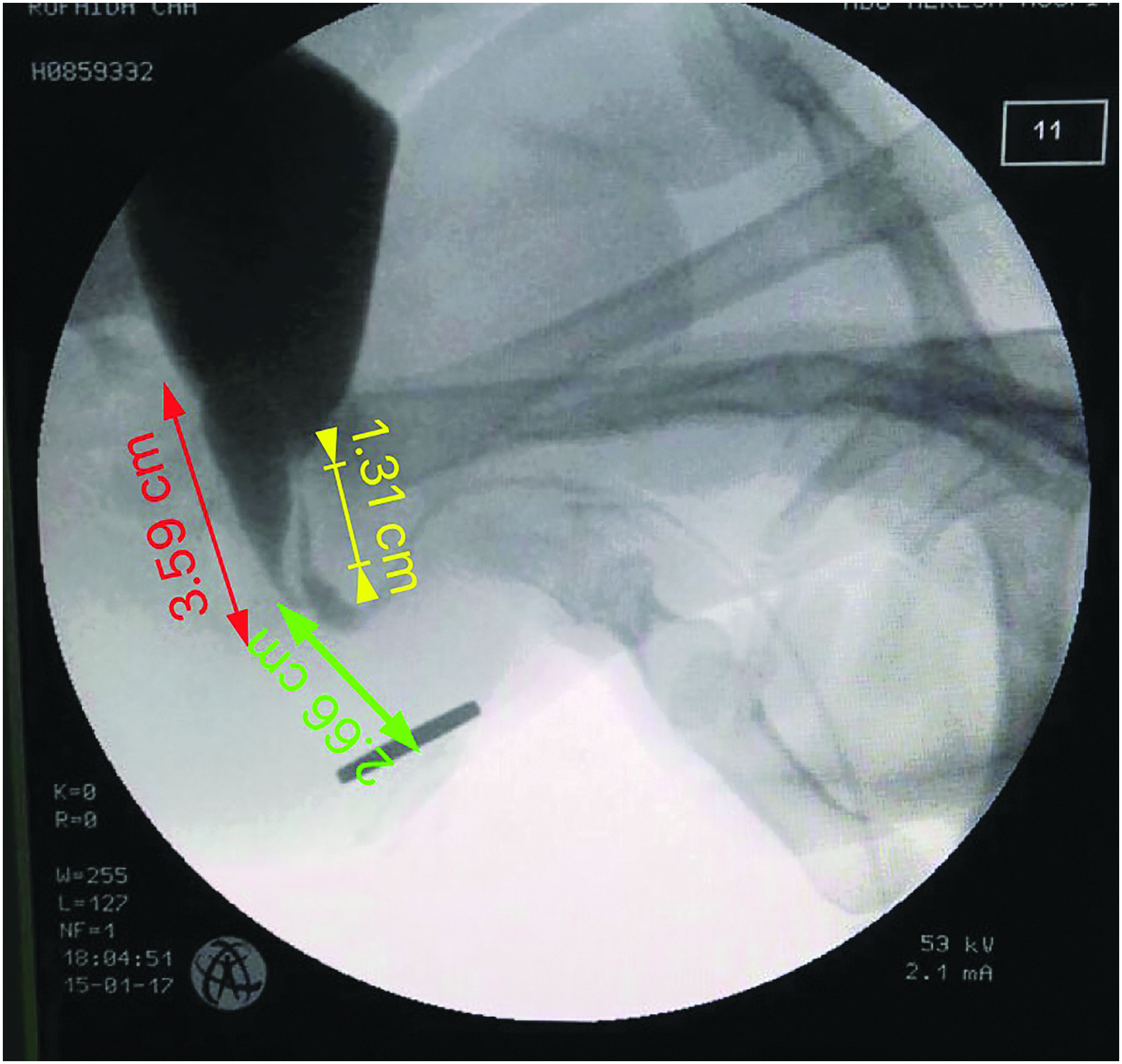
Lateral genitography showing the vaginal depth (green arrow), the vaginal length (red arrow), and the urethral length (yellow arrow).
Operative technique
All surgeries were carried out with the patient positioned supine with legs elevated. For the laparoscopic procedure, pneumoperitoneum was created by an open Hasson method. We used a 5 mm 30° telescope, inserted at the umbilicus. Two working instruments were placed on either side of the umbilicus at the midclavicular line, and a third instrument was used for retraction in the suprapubic area (Fig. 2).
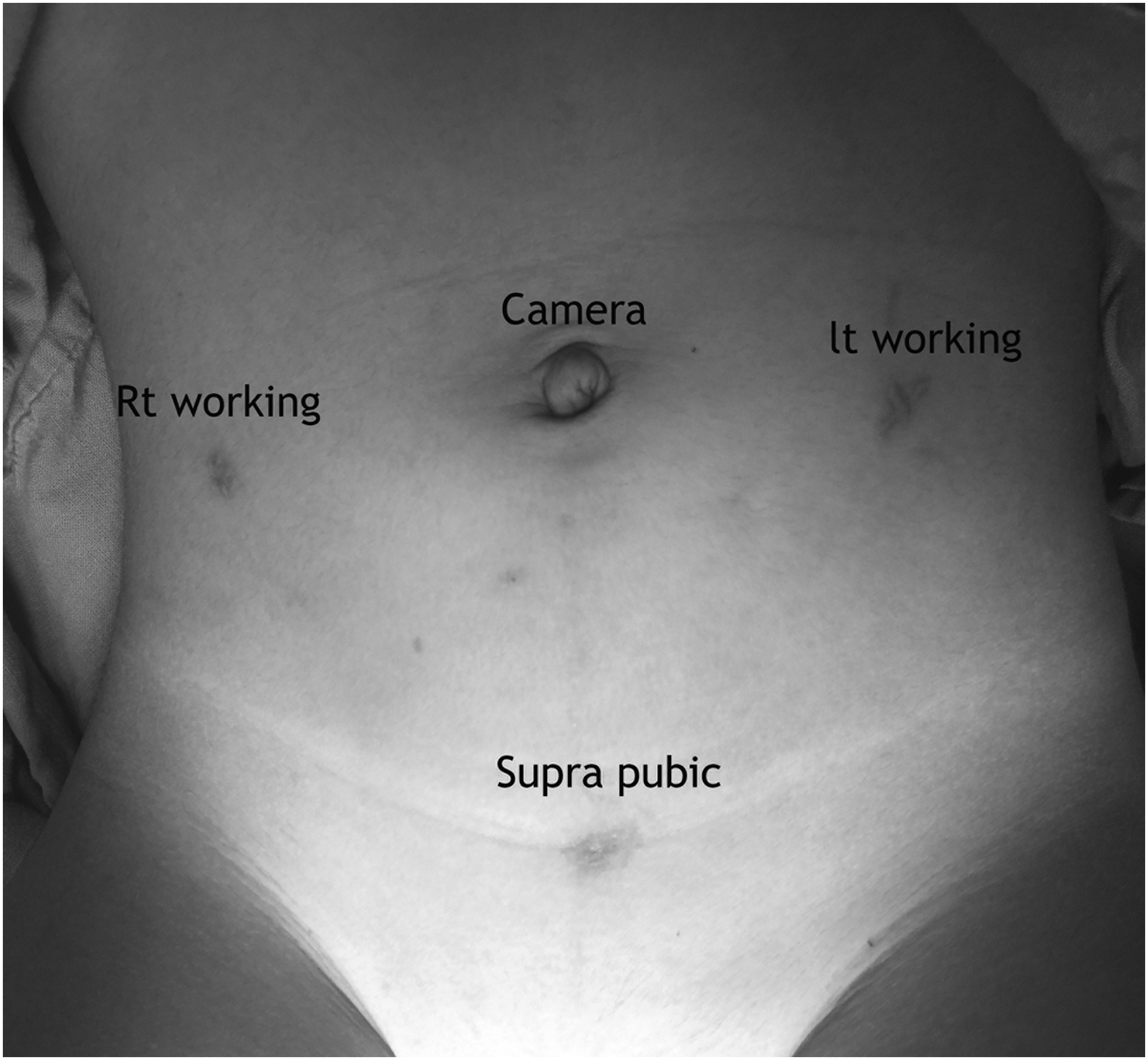
Port sites.
We performed dissection of the vagina anteriorly from the urinary bladder and urethra, creating the retrovesical space, then posteriorly from the rectum, creating the prerectal space. Dissection started by hook cautery using low settings on cutting mode, alternating with blunt dissection using Kelly or Maryland forceps. The dissection continued caudally till the confluence with the urethra became visible, and the vagina tapered down at its junction with the urethra. Extreme caution was exercised around the vaginal and uterine arteries on both sides (Fig. 3).
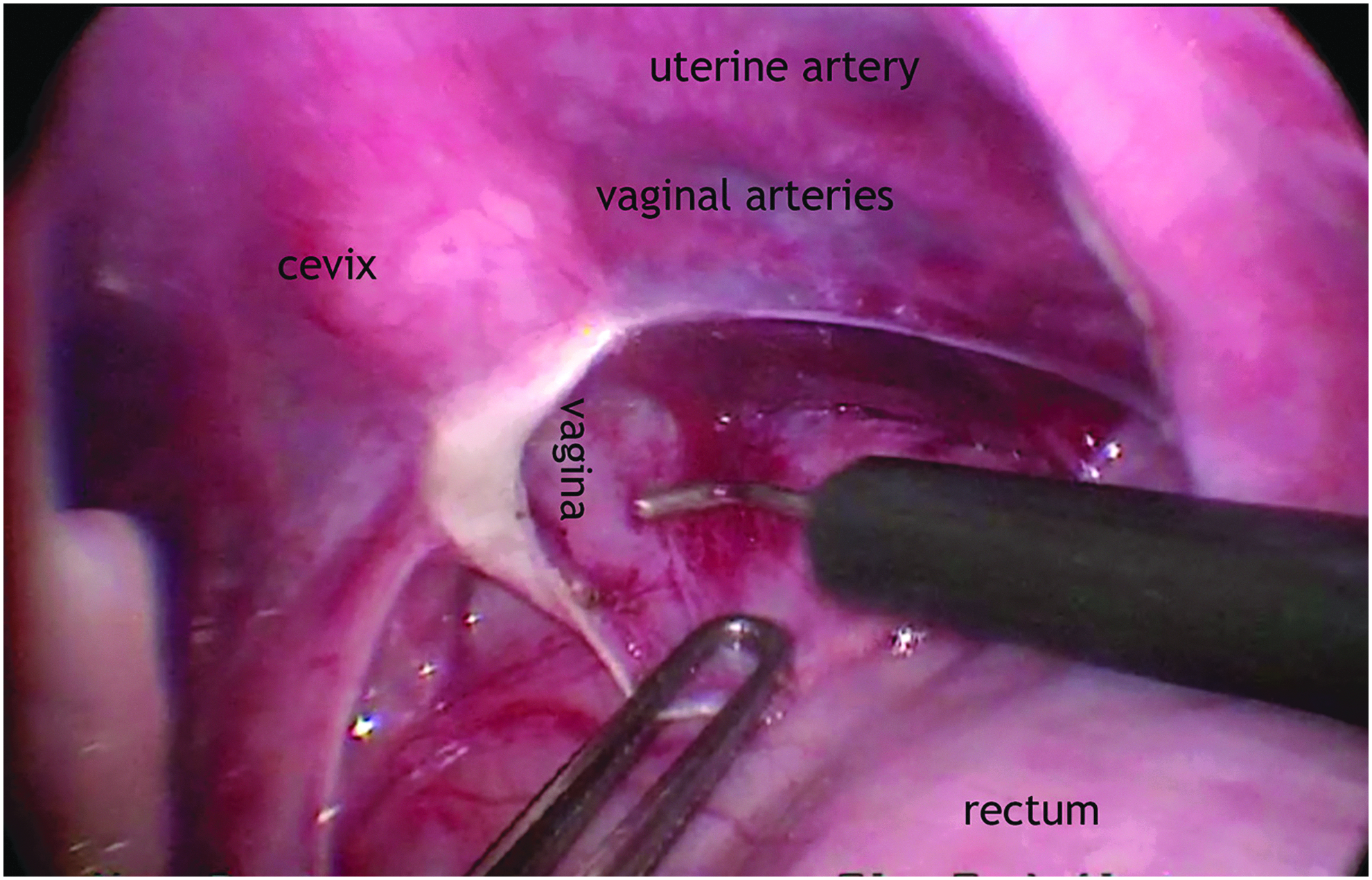
Rectovaginal pouch dissection. Taking care of the uterine artery and the vaginal arteries.
The connection is either sutured or clipped and then divided (Fig. 4). The round ligament of the uterus is divided on both sides. The tract for the vaginal pull-through is created from the perineum upward until seen laparoscopically. A clamp is passed upward from the perineum to the peritoneal cavity. The vagina is grasped and pulled outside and then sutured to the skin (Fig. 5). Sufficient vaginal mobilization was achieved in all cases, preserving the vaginal vascularity, and a direct perineal anastomosis was performed without skin flap augmentation of the vaginal wall. The clitoral reduction was not performed concomitantly.
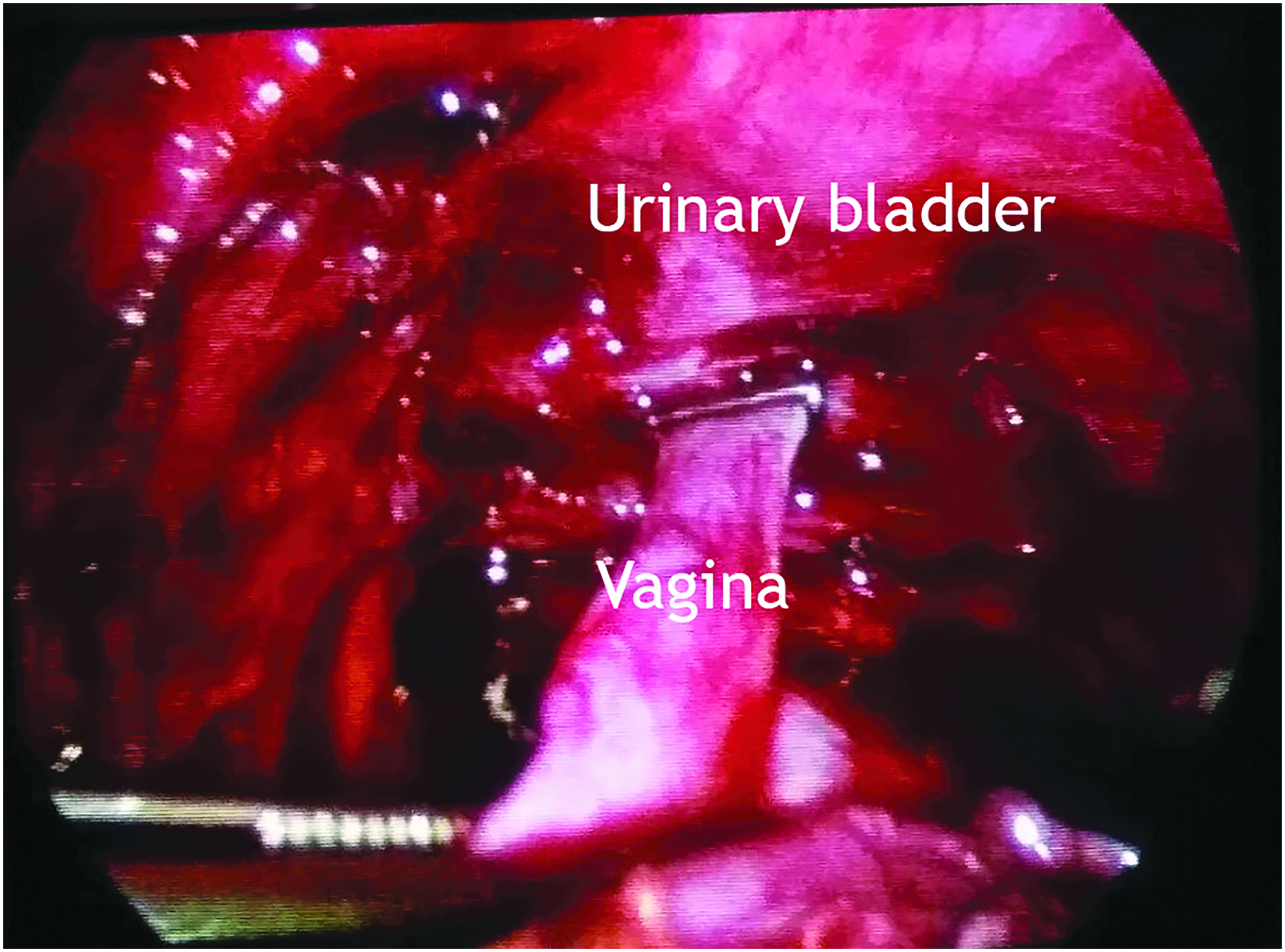
Clipping of the distal end of the vagina.
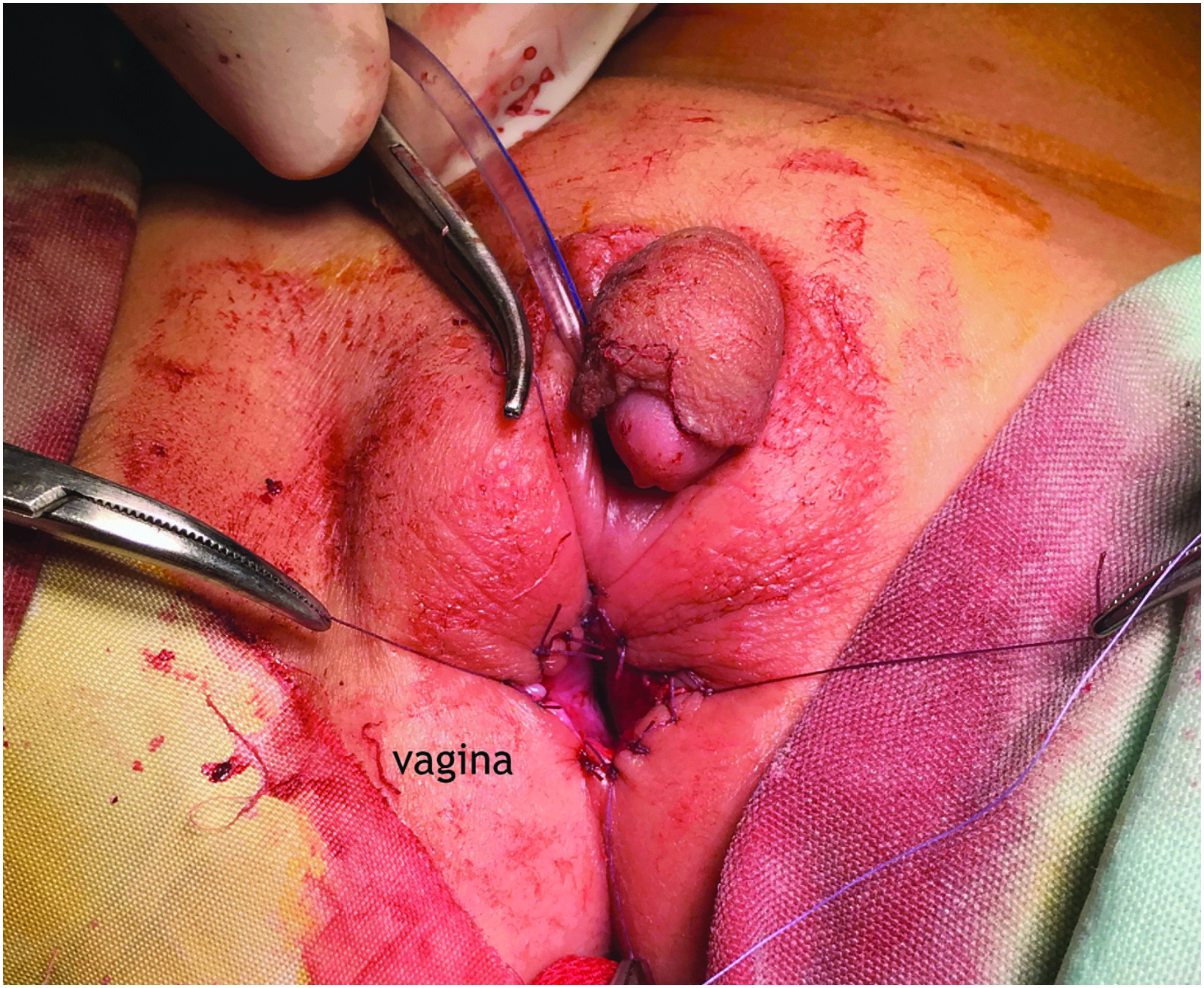
Suturing vagina to skin.
Follow-up
All cases were seen at 3, 6, and 12 months postoperatively. Clinical assessment was carried out at the 3- and 12-month appointments, and an examination under anesthesia with cystovaginoscopy and on-table cystogram and/or vaginogram were carried out at the 6-month appointment.
Results
The patients' age at the time of surgery ranged from 12 months to 5 years. All patients had a CAH. Genitography was performed for all patients preoperatively, under sedation. 12 The average length of the preconfluence urethra was 12.5 mm (range: 7–14.5 mm). In all the 7 cases, the operation was completed laparoscopically with no need for conversion. The mean operative time was 150 minutes (2 hours, 30 minutes). Intraoperative complications included injury to the vaginal wall in 2 cases. This was sutured on the outside from the perineum, after the pull-through. In 2 patients, the confluence-separation suture, at the junction with the urethra slipped intraoperatively, hence the urinary catheter was left for longer than the initially planned period (10 days after the operation); an early ascending urethrogram showed no fistulae or extravasation, and these 2 patients are currently voiding normally. There was no injury to nearby organs (rectum, ureter, urinary bladder, or the urethra). The vaginal anastomoses with the perineum was completed under minimal or no tension in all cases. A urinary catheter was left for 5 days postoperatively, in all except the 2 cases with a slipped suture, mentioned previously. No wound infection or dehiscence occurred in any case. Two weeks after surgery, the first calibration and dilatation of the vagina was carried out, and only 1 patient (14%) had vaginal stenosis. All patients had a separate urethral opening from the vagina that was easily visible in the vestibule. Follow-up ascending cystourethrography showed no stricture, fistula, or diverticula in any case. In all the 7 cases clinical assessment showed no lower urinary tract symptoms and no early signals of urinary continence problems after surgery. The mean follow-up was 15 months (range: 12–18 months).
Discussion
This study reports the early anatomical outcomes of laparoscopic assessment vaginal pull-through for high confluence UGS anomalies. This report included 7 patients followed up for 12 months or more after the reconstructive surgery. We selected the patients for this approach depending mainly on the preoperative genitography that was performed by our technique.12,13 We found this to be an accurate way of measuring the vaginal and urethral lengths, as was confirmed intraoperatively by laparoscopic findings.
The reported technique has the advantages of better visualization of the critical anatomical relationships of the vagina, as it approaches the bladder neck. It avoids detachment of the urethral sphincter complex from its fixation to the back of the pubis (as in total urogenital sinus mobilization [TUM]). This is analogous to the repair of imperforate anus and a high rectourinary fistula.14,15 We also found that access to the confluence was excellent, thus minimizing tissue damage by perineal dissection which is feared in other approaches.12,16 During dissection of the vagina from the urethra anteriorly, there were no injuries to the urinary tract and its sphincteric mechanism. And this can be attributed to the excellent exposure via laparoscopy.
UGS anomalies occur in a spectrum depending on the depth of the confluence from the perineum.6,7 Although we performed this technique mainly for the high urogenital confluence, its application could be extended to the intermediate cases, where the vagina would still be accessible laparoscopically and the vaginal length would allow a pull-through without any tension. It is arguable that the high UGS may require augmentation of the vaginal length with a distal colovaginoplasty to reach the perineum. However, we found that dividing the round ligaments on both sides as described by Fuchs et al. 15 provides an extra length of 2 cm. We believe this helped to reduce the incidence of stricture to only 1 of 7 cases, and in balance we preferred to avoid the added morbidity of including a bowel segment.
Vaginal stenosis and urinary incontinence are the most feared complications of surgical repairs of this anomaly. We reviewed results of other recent series of high confluence repairs, by alternative techniques. Al-Bassam and Gado 17 reported the development of vaginal stenosis in 16.2% of the patients who underwent either flap vaginoplasty or vaginal pull-through. Savanelli et al. 18 reported 1 case of distal vaginal stenosis, in a case with high confluence, out of 14 cases that had undergone a single-stage reconstruction. Bernabé et al. 19 encountered 2 cases of vaginal stenosis among 16 children who had feminizing genitoplasty, where vaginoplasty was performed in all of them perineally. Bailez et al. 7 and Kryger and González 20 reported a good outcome of continence after surgery for high and intermediate UGS using a combination of strategies as TUM, modified ASTRA, and the Hendren pull-through.
Laparoscopic vaginal pull-through may also have the advantage of saving the urethral sphincter and its innervations from perineal manipulations that can impair the patients' continence. Our postoperative follow-up involved cystovaginoscopy and cystograms, 6–12 months after surgery. One year after the operation, an excellent outcome was noted in 6 out of 7 cases, where the vagina showed an acceptable caliber and length for age. The urethral length was satisfactory in all cases, with no urethral stenosis or diverticulum.
This study is the first case series of vaginal pull-through for UGS performed by laparoscopy. Two cases were previously reported individually.15,21 Two cases have also been reported with a robotic-assisted similar technique. 22 The limitations of our study include the small number of patients in this cohort. However, it is known that this is a rare anomaly as the incidence of CAH is 1:15,000, and that high-confluence UGS is found in only 5% of female patients with CAH.10,23 In addition, the relatively short follow-up period limits this report to only assess feasibility and early results. Continence could not be assessed reliably in our patients as yet because of their age, but no significant lower urinary tract symptoms were reported.
Patients classified according to Prader's classification (from III to V degrees), would arguably need a form of clitoroplasty. 18 One of the established strategies is a single-stage early feminizing surgery, aiming to produce a feminine appearance, preserving the delicate genital nerve supply. 24 An important technical advantage of that is using precious tissues from the reduction clitoroplasty to reconstruct the labia minora and the vaginal vestibule. 25 This has been consistently our practice until recently, 23 aiming to confer an early physical appearance consistent with the female gender of rearing, and to cause less psychological stigmatization than with delayed surgery. 26 However, early genital reconstruction in disorder of sexual differentiation and development has become very controversial within the clinicians involved. Clitoroplasty is an irreversible procedure. There is a growing preference toward limiting surgical interventions in childhood especially for irreversible procedures or deferring them to when the child becomes an adolescent and can be more involved in gender assignment. 27 We acknowledge this and are adopting this careful approach when appropriate, despite the fact that within our society an argument against the rearing of virilized CAH female children toward the female gender is practically difficult, because of familial fixation on the 46, XX chromosomal pattern, and the reasonable likelihood of fertility and normalized life as females.
Our next step is to extend the utilization of this technique to intermediate cases and redo cases after failure of perineal approaches.
Conclusion
The laparoscopically assisted vaginal pull-through is a feasible procedure and a viable option in high UGS in female CAH children. This approach provides optimal exposure, facilitates vaginal dissection, separation of the vagina from the urethra, and reduces the chances of injury to the bladder neck and damage to the relevant innervation. This allows vaginal reconstruction without tension. Long-term follow-up is required to fully assess the outcome.
Footnotes
Acknowledgments
We are deeply grateful for the ongoing efforts of Professor Mohamed M. Elbarbary, Professor of Pediatric Surgery at Cairo University, as well as the staff members of the Diabetes, Endocrine and Metabolism Pediatric Unity (DEMPU) at Cairo University Children's Hospitals for their support to this work and their devotion to the DSD individuals and their families in Egypt.
Disclosure Statement
No competing financial interests exist.