
Abstract
Abstract
Purpose:
Acquiring laparoscopic skills occurs at different rates among trainees. We conducted a pilot study to determine whether variation in laparoscopic skill acquisition was associated with subject's learning styles.
Materials and Methods:
Nineteen medical students performed 10 repetitions of the object transfer task over a period of 4 weeks using a validated laparoscopic simulator. The main exposure was participants' learning style categorized according to the Fleming VARK-learning style inventory. VARK (V = visual, A = aural, R = read/write, K = kinesthetic) is a validated learning style model that identifies four different learning styles. The main outcome measures that reflected laparoscopic skill acquisition were task completion time (<107 seconds) and total instrument distance (<2.03 m) obtained from SurgTrac® motion analysis software. To determine whether participants' laparoscopic proficiency was associated with learning style we used chi-square tests for categorical variables and t-tests for continuous variables.
Results:
Nineteen participants completed the inventory, 37% (7) were classified as kinesthetic and/or visual style learners, while 63% (12) were considered multimodal or reading/writing style learners. Participants classified as visual/kinesthetic were ∼4 years older than participants classified as multimodal or reading/writing style learners. No gender differences were observed between the groups. Eighty-five percent (6) of participants with a kinesthetic and/or visual learning style reached the proficiency level for task completion time while only 17% (2) of participants with multimodal or read/write learning style performed the task in <107 seconds (χ2 = 8.7; P = .003). Regarding total instrument distance, 85% (6) of participants classified as kinesthetic and/or visual learners and 67% (8) of participants classified as multimodal or read/write learners performed the task in <2.03 m (P = .36).
Conclusions:
This is the first study to investigate the correlation between trainees' VARK-learning style and their ability to acquire laparoscopic skills. This pilot study suggests that trainees' learning style may affect the ability to acquire laparoscopic skill proficiency. Larger studies are needed to confirm these preliminary observations.
Introduction
L
A learning style is the learner's method for efficiently and effectively perceiving, processing, storing, and recalling information. Learning styles are widely used in higher education to tailor the learning experience for students.6,7 To the best of our knowledge, no study has ever determined whether learning style is associated with becoming proficient at laparoscopy.
The aim of this pilot study was to determine whether a subject learning style was associated with the ability to become proficient at laparoscopy.
Materials and Methods
To accomplish the study aim, we recruited 19 medical students, who were naïve to surgery, to participate in a series of 10 laparoscopy simulation trials. The participants were identified among medical students from University of Manitoba. Our inclusion criteria were as follows: (1) no laparoscopic experience; (2) right-handed subjects (to avoid handedness bias); (3) no video gamers (less than 1 hour/week). We excluded students who were (1) left handed subjects and (2) video gamers (more than 1 hour/week). All trainees provided informed consent before participating in accordance with the Declaration of Helsinki. The study was approved by the local Research Ethics Board (REB no. HS20361).
Main exposure: learning style assessment
Learning style was established in each participant using the Fleming VARK (V = visual, A = aural, R = read/write or K = kinesthetic) Questionnaire version 7.1.* The Fleming VARK learning style inventory is a validated learning style model consisting of 16 multiple-choice questions. Each question has four possible responses, each participant could select one, more than one, or none of the possible choices. The VARK inventories were then scored to determine the learning style preferences for each subject. Participants were categorized as having a unimodal (V = visual, A = aural, R = read/write or K = kinesthetic), bimodal, or multimodal learning style preference. 8 To minimize any potential bias, participants completed the questionnaire after the last training session.
Main outcome measure: laparoscopic tasks and performance recording
Each participant performed the object transfer task 10 times, using a previously validate pediatric laparoscopic box. 9 The task consisted of threading a string through hoops using 3 mm laparoscopic instruments working in a reduced laparoscopic space to reproduce an infant abdomen (Fig. 1).
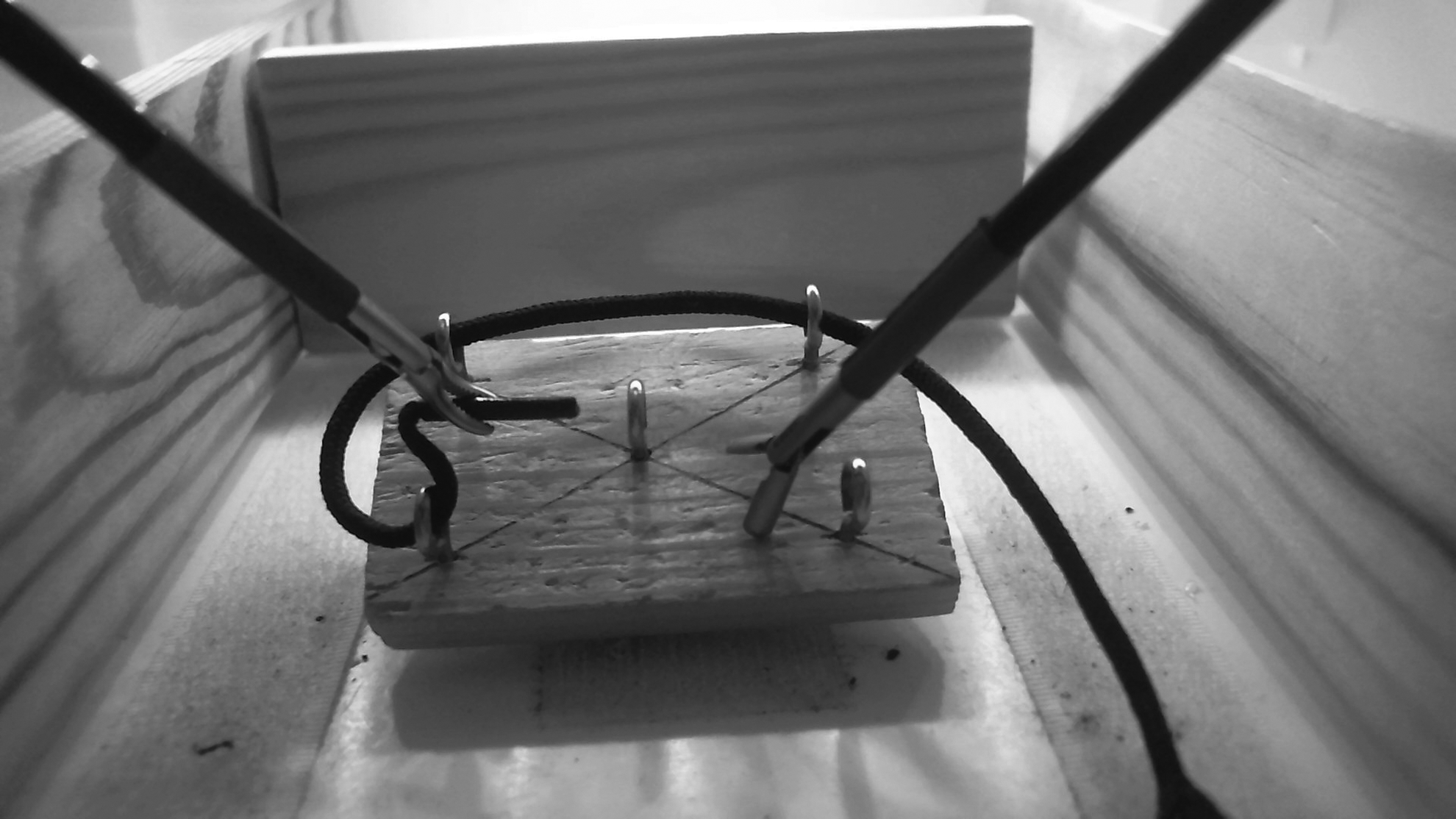
Object transfer task.
To standardize the learning curve of the subjects, each participant could not perform more than two training sessions per day, and each session had to be performed more than 1 hour apart. All participants had to complete the 10 training sessions within a period of 4 weeks. 10
Each participant watched a video explaining “how to perform the laparoscopic task” before starting the training sessions; everyone had verbal supervision to complete the task during the first three repetitions.
Laparoscopic skill acquisition was quantified using a commercial motion analysis software (SurgTrac®, software able to track the movements of the instruments), 11 according to proficiency criteria established in a previous study (task completion time <107 seconds and total instrument distance <2.03 m) by a member of the research team. 9 Thresholds were obtained in a previous study by comparing expert, intermediate, and novice performances. Construct validity was demonstrated with respect to both task completion time and total instrument distance. Thresholds were defined as the mean expert value for each metric plus two standard deviations. As the participants were medical students, they did not perform any laparoscopic procedure as first operator in the operating room during the data collection and we asked them to not play videogames.
Statistical analysis
Descriptive and outcome measures were compared across learning styles using t-tests for continuous variables and chi-square tests for proportions. The two main outcomes that reflected laparoscopic task proficiency, time to completion and total instrument distance, were categorized as binary measures with thresholds set at <107 seconds and <2.03 m as previously described. 9 We used chi-square tests to test for differences in time to completion and total instrument distance between trainees classified as “unimodal” learners and those considered “multimodal” learners. We repeated analyses using logistic regression analyses adjusting for age. We set an α threshold of <0.05 to consider group wise differences in outcome measures meaningful.
Results
Twenty-eight medical students responded to advertisements. Six failed to present for testing. Three participants were not able to complete the 10 repetitions in less than a month and they were excluded from the study. Nineteen medical students performed the object transfer task 10 times in less than 1 month and the Fleming VARK questionnaire after the last training session. Based on the scores from the VARK questionnaire, 11 (58%) were classified as having a multimodal learning style (9 VARK and 2 VRK), 2 (11%) were considered bimodal Visual-Kinesthetic, and all the rest were unimodal as follows: 1 (5%) Visual, 1 (5%) Read/Write and 4 (21%) Kinesthetic (Fig. 2). Unimodal and bimodal leaners were ∼4 years older (28 years versus 24 years, P < .05) than multimodal learners VARK or VRK or Read/Write learning style. There were no gender differences between the groups.
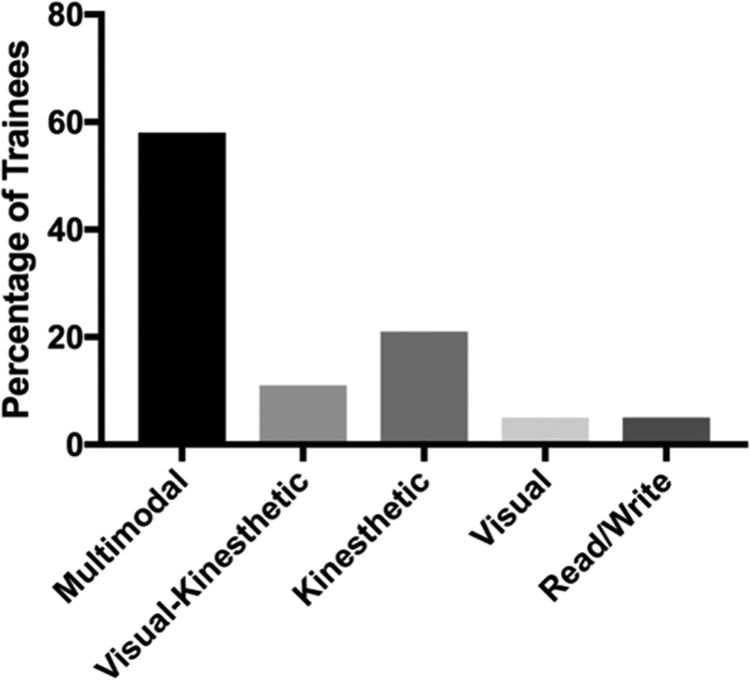
Learning styles distribution.
For the primary outcome measures, 85% (n = 6) of participants categorized as unimodal learners achieved proficiency for the task completion time while only 17% (n = 2 medical students) of multimodal learners could perform the object transfer task in less than 107 seconds (χ 2 = 8.7; P = .003) (Table 1). This remained significant after adjusting for differences in age.
Statistically significant difference.
For the outcome measure of total instrument distance, 85% (n = 6) of participants with bimodal VK or unimodal Kinesthetic and Visual learning style reached the proficiency level while 67% (n = 8) of the participants classified as multimodal or Read/Write learners reached proficiency after 10 trials (P = .36).
Discussion
This pilot study provides preliminary evidence that acquiring laparoscopic skills may be associated with the subject's learning style. Larger observational and experimental studies are needed to confirm these initial observations.
The concept of learning styles is widely used in higher education to optimize the learning experience of students.6,7 Conventional wisdom for skill acquisition among surgical residents, is that some “have good hands” while others do not. Few empirical studies have attempted to quantify the ability to acquire surgical skills.1,12,13 Considering the enormous time and resources dedicated to training surgical residents, methods to categorize learning styles and tailor the learning experience to those styles may be an attractive option for departments to consider.
Learning style is defined as the ability of an individual to acquire new skills and adjust existing behaviors or the way an individual can efficiently and effectively perceive, process, store, and recall information. Establishing the learning style of a surgical resident could help to improve his or her learning experience and give some suggestions to the surgical educator on how to improve the trainee learning experience.4,14 Larger trials are needed to confirm this theory.
Assessing learning style among medical trainees has been studied extensively.15,16 These studies suggest that students prefer receiving education training tailored to their learning style. Most studies have relied in the Fleming VARK scale to assess learning style, however, other learning style inventories exist. 7 David Kolb's “Experiential Learning Theory” proposes that learners must grasp and transform experience to produce new knowledge, engaging into Kolb's Learning Cycle. 17 In his initial work, Kolb defined four different types of learning styles: Accommodating, Diverging, Assimilating, and Converging. These learning styles are defined following the learner's way to acquire and elaborate the experience through the learning cycle; for example, if a subject perceives the experience using “concrete experience” and transform it through “active experimentation,” we are going to identify an Accommodating learning style (Fig. 3).
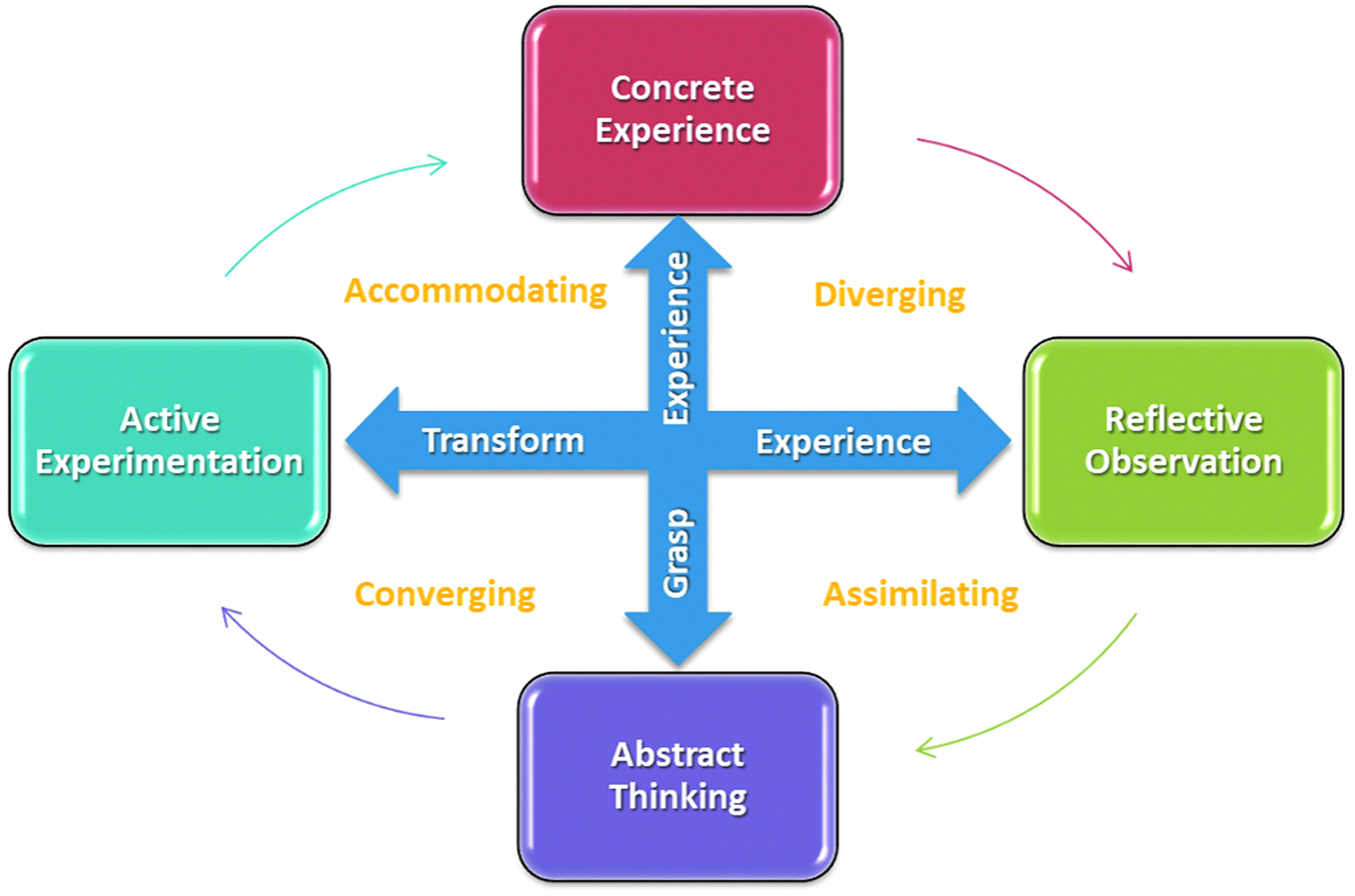
Kolb's Learning Cycle adapted from Kolb. 17
After the last major review of Kolb's Learning Styles Inventory (LSI 4.0) 18 the number of learning styles increased up to nine: Initiating, Experiencing, Imagining, Acting, Balancing, Reflecting, Deciding, Thinking, and Analyzing.
An ideal learning experience occurs when the learner goes through all the learning cycle steeps using multiple learning styles. In reality, this is difficult to achieve and everyone uses a preferred learning style to elaborate the learning experience, using only a part of the learning cycle.
We thought that the classical learning styles proposed by Kolb could be less meaningful to our study, and we felt more appropriate to use a sensorial-based learning style inventory such as the Fleming VARK to correlate with the laparoscopic performance of our participants.
The Fleming VARK learning style is a free, easy-access, validated learning style inventory that has been previously used to assess general surgery and other specialities residents' learning style and their academic and career achievements.19,20 It has never been used to assess the ability to learn laparoscopic skills.
The abbreviation VARK means: Visual, Aural, Read/Write, and Kinesthetic. The Read/Write section is sometime omitted. Fleming decided to add the Read/Write learning style as second visual modality because he noticed some learners have a distinct preference for the written words while other subjects, with Visual learning style modality, prefer proper images such as pictures, diagrams, and so on. 21 Learners can learn better if they are exposed to activities that are related to their learning style. Visual learners tend to learn best when they are seeing the tasks that are required of them. Aural learners benefit from hearing what is required. Read/Write learners do better when they can read and/or write about the topic. Kinesthetic learners tend to learn better once they have experienced what is required of them.
It is common experience to feel that some trainees can learn and perform better than others. Even though our sample size is small, our results suggest that the way we learn may affect the way we perform. Currently, we are not able to predict candidates' aptitude for a surgical career. Some authors suggested that not everybody can reach a proficiency level in laparoscopy and that it is not currently possible to predict surgical technical aptitudes.1,5
The current pilot study has limitations that need to be acknowledged. The sample size was small and the participant studies were only studied over the course of 4 weeks. The study is strengthened by the use of objective measures of surgical performance and a well accepted method to categorize learners. The data presented here should be interpreted with caution and inform future trials that could provide more conclusive evidence to inform surgical education and training practices.
In conclusion, there is preliminary evidence that acquiring laparoscopic skills is associated with trainees' learning style. These findings demonstrate the need for further studies in surgical trainees' learning style and design studies to determine whether assessing trainees' learning style can improve the training and selection process of surgical residents.
Footnotes
Disclosure Statement
No competing financial interests exist.