
Abstract
Abstract
Purpose:
The aim of this study was to compare the safety and efficacy of single-incision laparoscopic-assisted anorectoplasty (SILAARP) to that of traditional three-port laparoscopic-assisted anorectoplasty (3-PLAARP) for persistent cloaca (PC) patients with mid to high rectal pouches in midterm follow-up.
Materials and Methods:
A study comparing 13 SILAARPs and 12 3-PLAARPs performed by a single surgeon from November 2005 to May 2016 was presented (laparoscopy was performed for anorectoplasty, and urethra vaginoplasty was performed perineally). Data including demographics and perioperative and midterm outcomes were retrospectively compared. Operative performances between the groups were compared using the Global Operative Assessment of Laparoscopic Skills (GOALS).
Results:
The two groups were comparable in terms of demographics. No significant difference was observed between SILAARP and 3-PLAARP groups in terms of median operative time, transfusion rates, intraoperative complications, time to resume diet, postoperative hospital stays, and GOALS scores. Postoperative outcomes included 1 patient with incomplete intestinal obstruction (SILAARP group), 1 patient requiring intermittent catherization to remain dry (3-PLAAR group), 2 patients with occasional urine incontinence (one in each group), and 5 girls with mild mucosal prolapse (2 and 3 in the SILAARP and 3-PLAAR groups, respectively); however, these did not differ significantly between groups. Trocar-related scars of the patient who was undergoing SILAARP were almost invisible. After 18 months follow-up, the rates of soiling and constipation were similar in both groups.
Conclusion:
The midterm outcomes of SILAARP were comparable to those of 3-PLAARP. It appears to be a safe and effective procedure with better cosmetic results for mid to high rectal pouches in PC children.
Introduction
Persistent cloaca (PC) is the most severe type of anorectal malformation (ARM). In a recent Japanese study, the incidence of PC from 1980 to 2012 was reported to be 0.97/100,000 live births. 1 Laparoscopic-assisted anorectoplasty has been recognized as common surgical technique for the treatment of ARMs in recent decades.2–4 In addition, with the rapid development of laparoscopic technology and the increasing improvement of postoperative quality of life, minimally invasive surgery has become the goal of modern surgery with the condition of ensuring the safety and of achieving similar curative effects.5,6 In addition, according to recent reports, Laparoscopic-assisted anorectoplasty appeared to be an effective and safe option for selected patients with PC.7,8 However, a comparison between single-incision laparoscopic-assisted anorectoplasty (SILAARP) and the three-port laparoscopic-assisted anorectoplasty (3-PLAARP) for PC has never been performed.
This present study was designed to compare the midterm outcomes of these two procedures for children with PC by a single surgeon (L.L.). We also objectively evaluated operative performance between the groups by completing the Global Operative Assessment of Laparoscopic Skills (GOALS)—a 5-item self-reported questionnaire. 9
Materials and Methods
Patients
The records of all 59 PC patients treated from November 2005 and May 2016 in our hospital were reviewed. All children underwent preoperative distal colostogram, renal ultrasonography, micturating cystogram, urethroscopy, and X-ray of the sacrococcygeal region to identify the type of PC, sacral ratios (SR), length of the common channel (CC), and associated anomalies.
The inclusion criteria for this study were as follows: (1) the patients' rectal pouches were higher than the pubococcygeal line; (2) anorectoplasty, vaginoplasty, and urethroplasty were carried out at the same stage; and (3) their parents agreed to complete this study requirement. Exclusion criteria were as follows: (1) patients with any contraindication or who were unsuitable for laparoscopy and (2) patients with a CC shorter than 1 cm.
Therefore, 25 patients were available for analysis, of which 13 patients were allocated to the SILAARP group and 12 patients were assigned to 3-PLAARP group. Colostomy was performed in all children. In the SILAARP group, the mean age of the patients at the time of operation was 9.38 ± 2.99 months (range 4–15 months). The median length of the CC was 2.28 ± 0.60 cm (range 1.5–3.5 cm). Associated anomalies were present in 10 patients (76.9%), including sacral spinal dysraphism (30.1%), hydronephrosis (23.1%), duplex uterus (23.1%), spina bifida occulta (23.1%), unilateral kidney (15.4%), horseshoe kidney (7.7%), and ureteral reflux (7.7%). Multiple anomalies were detected in 5 patients. In the 3-PLAARP group, the median age of the patients was 8.33 ± 5.26 months (range 5–24 months), and the mean length of the CC was 2.41 ± 0.78 cm (range 1.5–4.0 cm). Clean vaginal intermittent catheterization was found in 2 cases. Ten (83.3%) had associated anomalies, including duplex uterus (33.3%), hydronephrosis (25.0%), sacral spinal dysraphism (16.7%), spina bifida occulta (16.7%), double vagina (16.7%), ureteral reflux (16.7%), and unilateral kidney (8.3%). Multiple anomalies were detected in 5 patients. Two patients were managed with clean intermittent catheterization while waiting for surgical reconstruction. One was from the SILAARP group (CC = 3.0 cm) combined with spina bifida occulta and double vagina, the other was from the 3-PLAARP group (CC = 2.0 cm) with sacral spinal dysraphism, and their SR were both lower than 0.4 (0.38 and 0.36 in the SILAARP and 3-PLAARP groups, respectively).
Ethics approval from the Ethics Committee of the Capital Institute of Pediatrics was obtained. Written informed consents were obtained from the parents before the surgery.
Surgical technique
Operations were performed by a fixed surgical team. All patients in both groups were under general anesthesia and were placed in Trendelenburg position. A surgical towel roll was placed under children's buttocks to acquire better exposure (pelvic cavity). Before surgery, we examined the length of the CC and location of the fistula opening by urethral speculum. The bladder was catheterized with a suitable urinary catheter.
Single-incision laparoscopic-assisted anorectoplasty
A similar access technique for transumbilical laparoscopy was performed in children as described previously. 8 A 2 cm vertical umbilical incision was made and an extra long 5 mm 30° laparoscope was inserted with direct vision. After pneumoperitoneum was established at a pressure between 8 and 12 mmHg, the vertical umbilical incision was stretched horizontally for insertion of the other two 3 mm lateral ports. These three ports were placed in a horizontal line.
To better expose the operative field, a transabdominal retraction suture was placed through the uterine wall under laparoscopic vision. Laparoscopic rectal dissection was begun at the distal mesosigmoid and mesorectum. To gain adequate bowel length, we usually anatomized the sigmoid mesocolon and rectal mesentery and divided the terminal branches of the sigmoid and rectal arteries, while ensuring that the blood supply to the distal rectum was preserved. Then, circumferential dissection around the rectal pouch was performed until the junction of the fistula and urogenital sinus was identified. Dissection was performed adjacent to the rectal wall to avoid subsidiary injury to the surrounding structures such as the ureters and iliac vessels. Next, the fistula was ligated with a Hem-o-Lock clip or 5-0 PDS horizontal running suture that was close to the urogenital sinus. After the terminal rectal pouch was separated, we appropriately excised fat tissue to expose the pelvic floor striated muscle.
The perineal procedure was implemented with the baby's legs flexed. A 1-cm midline skin incision was made at the site of the future anal orifice and the center of the external sphincter was mapped with a transcutaneous electrostimulator bluntly under laparoscopic guidance. Next, a “potential tunnel” penetrating the center of the sphincter complex to the pelvis was created with mosquito forceps and seven-inch artery forceps successively under the guidance of the laparoscope, and the tunnel was further dilated with a Hegar dilator up to 12 mm. The separated terminal rectal pouch was pulled down through the muscle complex to the perineum without tension. The megarectosigmoid with weak peristaltic function would be resected and sent for pathological examination. Anastomosis between the rectum and the anus was performed with absorbable interrupted 5-0 PDS sutures.
Urethroplasty and vaginoplasty were simultaneously performed with anorectoplasty. After the posterior wall of the CC was incised longitudinally to expose the urethral and vaginal orifices, we meticulously dissected the posterior and lateral walls of the CC to extend the urethra and vagina, while the anterior wall of the CC was left intact. Two 6–8 French urinary catheters were inserted into the urethra and vagina, respectively, as stents. The lateral walls were divided into two parts. The anterior parts and the anterior walls of the CC were mobilized to form a flap that was used to extend the length of urethra by wrapping around the urinary catheter with multiple 6-0 PDS stitches. Similarly, the posterior part of the lateral walls and the posterior walls of CC were constructed to repair the vagina length. A 5 mm septum between the urethra and the vagina was rebuilt by approximating the tissue on each side. The reconstructed urethra and vagina were sutured to the skin without tension (Fig. 1). Finally, a 12 French urinary catheter was placed to stent the reconstructed anus, and all urinary catheters would be removed at the 14th day after operation.

External appearance of the anus, urethra, and vagina after the repair of persistent cloaca.
Three-port laparoscopic-assisted anorectoplasty
The technique involved inserting a 5 mm trocar through the umbilicus for the 30° laparoscope, and two 3 mm trocars at both the left and right iliac fossae for the instruments. Pneumoperitoneum was established at a pressure between 8 and 12 mmHg, and the laparoscopic and perineal procedures were similar to those of the SILAARP procedure.
Anorectal dilation was started at 2 weeks after operation and lasted for half a year. The size of the dilator was gradually increased until it reached suitable size. All patients would undergo routine micturating cystogram on the tenth day after operation. A visible urethral meatus and almost normal-appearing genitalia without edema were verified before the urethral catheter was removed. Our routine was to close the colostomy at ∼2 months postoperatively when the anus had reached the desired size. Distal colostogram and micturating cystogram were performed before colostomy closure.
Follow-up
The children were followed up in our clinic at 1, 3, 6, and 12 months postoperatively and every 6 months thereafter. Physical examination, micturating cystogram, and distal colostogram were routinely carried out before colostomy closure. Perioperative data, including age at the time of the operation, operative time, time to resumption of diet, length of hospital stay, and intraoperative complications were collected and evaluated. For the sake of better comparison of the efficacy and safety of these two procedures, we selected 18 months postoperatively as a midterm follow-up time point. All patients' postoperative complications and postoperative bowel functions (Krickenbeck classification) were collected at this point to evaluate the midterm outcome of each procedure. We did not evaluate the index of voluntary bowel movements since most of children (24/25) were not beyond 3 years of age. Urinary continence was defined as dry intervals greater than 4 hours (totally continent). Patients unable to hold urine for at least 2 hours were considered incontinent. 10 The operative performance evaluated with the GOALS score were self-reported by surgeon immediately after completion of surgery or reviewing the surgical video.
Statistical analyses
All statistical analyses were performed using SPSS 17.0 software (Chicago, IL). Continuous data were expressed as the mean ± SD. Comparisons of categorical data between the two groups were made using the Fisher exact test. Continuous data were compared using the two-tailed t test. A P value <.05 was considered statistically significant.
Results
The patients' demographic and clinical characteristics of the two groups were comparable with respect to age, SR, associated anomalies, and the length of the CC (Table 1).
Patient Characteristics, Perioperative Variables, and Outcomes Between the Two Groups
Data are presented as the mean ± SD or number (percentage).
Trocar-related cosmetic results.
New-onset complication after surgery.
SILAARP, single-incision laparoscopic-assisted anorectoplasty; 3-PLAARP, three-port laparoscopic-assisted anorectoplasty; CIC, clean intermittent catheterization.
Surgeries were successfully performed in all cases and intraoperative blood loss was minimal. Anorectoplasty, vaginoplasty, and urethroplasty were carried out at the same stage. None of the SILAARP groups required an additional extraincisional trocar. The scars on the patients who underwent SILAARP were almost invisible. MRI showed a centrally placed rectum within the muscle complex in all patients of the two groups.
The perioperative parameters for the two groups are listed in Table 1. There was no statistically significant difference between the SILAARP and 3-PLAARP groups in terms of median operating time (122.54 ± 9.47 versus 126.25 ± 7.82 minutes; P = .30), transfusion rate (0% for both; P = 1.00), intraoperative complications (0% for both; P = 1.00), time to resumption of diet (9.92 ± 1.75 versus 10.75 ± 2.30 hours; P = .33), or postoperative hospital stay (6.46 ± 1.20 versus 6.17 ± 1.03 days; P = .52). The operative performance evaluated with the GOALS score is shown in Figure 2. The depth perception, bimanual dexterity, efficiency, tissue handling, and autonomy did not differ significantly between groups.
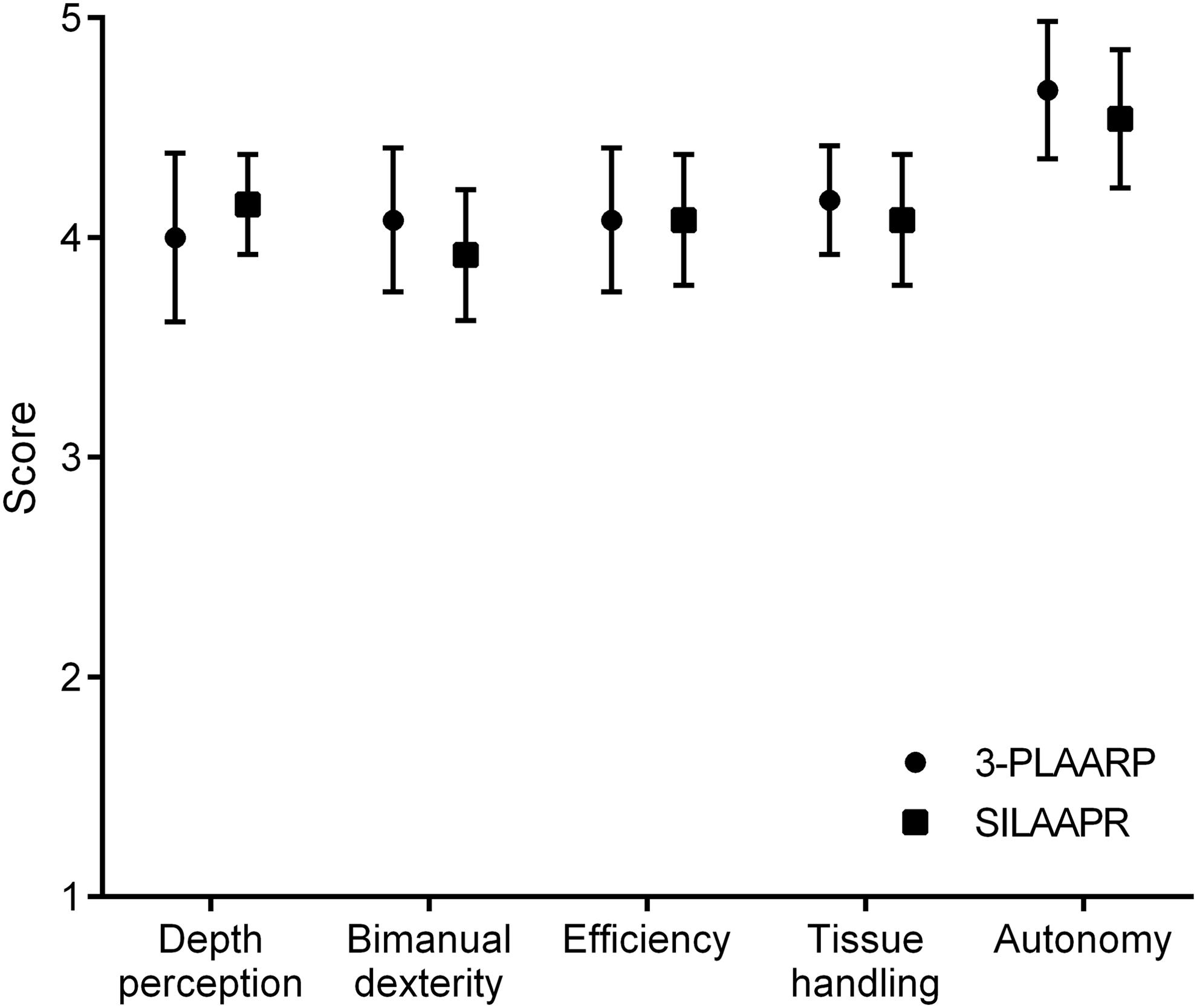
Operative performance with GOALS between groups. Higher scores indicate better performance. Pairs of shapes show scores for SILAARP (circle) and 3-PLAARP (square). Shapes and whiskers indicate mean values and 95% confidence intervals, respectively. The scores regarding depth perception, bimanual dexterity, efficiency, and tissue handling did not differ significantly between groups (P > .05). GOALS, Global Operative Assessment of Laparoscopic Skills; SILAARP, single-incision laparoscopic-assisted anorectoplasty; 3-PLAARP, three-port laparoscopic-assisted anorectoplasty.
Megarectum was found in 9 (69.2%) and 8 (66.7%) children in SILAARP and 3-PLAARP groups, respectively; however, pathological examination showed that roughly normal ganglionic cells and myenteric plexuses were found in all specimens (Fig. 3).

Pathological examination of excised megarectum.
Postoperative complications did not differ significantly between groups (Table 1), including one 4-month-old girl in the SILAARP group who developed incomplete intestinal obstruction on the fourth day after surgery, and successfully recovered with conservative therapy (fasting, gastrointestinal decompression, and enema therapy); 2 girls in the SILAARP group developed mild mucosal prolapse, whereas in the 3-PLAARP group, this number was three, but none required surgical intervention. A total of 3 patients (12%) developed postoperative new-onset urinary dysfunction, and all were combined with some degree of sacral dysplasia. Among them, 1 was from the 3-PLAARP group (CC = 3.5 cm, SR = 0.57 combined with spina bifida occulta and hydronephrosis) and needing intermittent catherization to remain dry. Occasional urinary incontinence was found in 1 patient in the SILAARP group (combined with unilateral kidney and sacral spinal dysraphism, CC = 3.0 cm, SR = 0.51) and 1 patient in the 3-PLAARP group (combined with spina bifida occulta and double vagina, CC = 1.5 cm, SR = 0.34). There was no wound infection, retraction, port-site hernia, urethrovaginal fistula, acquired anorectal atresia, or urethral injury in either group.
The Krickenbeck classification was used to assess postoperative bowel function. By the 18-month follow-up, the mean age of patients in the SILAARP and 3-PLAARP groups was 27.38 ± 2.99 months (range 22–33 months) and 26.33 ± 5.26 months (range 23–42 months), respectively, and all children had started potty training. There were no significant differences with respect to soiling and constipation between the two groups (Table 2). We considered those presenting with Grade 3 soiling to have incontinence, however, none of the patients was labeled having this grade of soiling. Although no noticeable incontinence was observed in any of the children, occasional or daily soiling was observed in 7 patients in the SILAARP group and in 4 patients in the 3-PLAARP group. Constipation occurred in 5 patients in both the SILAARP and 3-PLAARP groups that could be alleviated by nonsurgical methods. Among the 11 children with soiling and 10 children with constipation, 72.7% (8/11) and 70.0% (7/10) of them were combined with various sacral and/or spinal malformations, respectively. Statistical analysis showed no difference between children with and without sacral and/or spinal malformation in terms of the incidence of constipation (P = .059). However, significant difference in terms of the incidence of soiling was seen between the subgroups (P = .046) (Table 3).
Functional Results of Patients Between the Two Groups
Data are presented as number (percentage).
SILAARP, single-incision laparoscopic-assisted anorectoplasty; 3-PLAARP, three-port laparoscopic-assisted anorectoplasty.
Relationship Between Bowel Functional and the Status of the Sacrum and Spine
Data are presented as number (percentage).
For all patients in the SILAARP group, there were no visible trocar-related scars on the abdomen. Incisions were hidden in the umbilical fold, whereas obvious trocar-related scars could be seen on the abdomens of all 3-PLAARP group children (P < .05).
Discussion
Transumbilical endoscopic surgery that achieves excellent cosmesis by hiding umbilical wounds inside the umbilicus has become increasingly pervasive. 11 In recent years, single-incision laparoscopic surgery has been adopted at several centers treating pediatric surgical diseases. Our center also reported short-term outcomes of SILAARP for 5 children with PC, a rare and complex form of ARM. 8 To the best of our knowledge, however, this study was the first series to compare the safety and the efficacy of SILAARP and 3-PLAARP for children with PC.
For most PC children, despite the largest scar often being stoma take-down scar, reducing trocar-related scars could nevertheless beautify abdomen to some extent. Moreover, surgeons could further lessen stoma take-down scars using improved closure methods such as the purse-string closure technique. 12
Although SILAARP provided a better cosmetic outcome, it may carry some drawbacks, including the loss of triangulation with conventional instruments, a challenging work angle, difficulty of achieving correct exposure, and relative small working space. 13 In the field of pediatric laparoscopic surgery, however, most of the performance evaluations of operations are assessed by unilateral subjective description. Therefore, we evaluated the operative performance with GOALS scores, which have been supported as an objective assessment tool for laparoscopic technical skills.14,15
In our study, SILAARP and 3-PLAARP had similar performances in terms of depth perception, bimanual dexterity, efficiency, tissue handling, and autonomy. The reason might be that the trocars were placed in a line through the incision rather than in an inverted triangle in the umbilicus. This assignment, which increases the freedom of motion and the depth of instruments able to reach by enlarging the horizontal distance between trocars, makes SILS as convenient as traditional laparoscopic surgery, especially for fistula dissection and meticulous suture closure in PC. In addition, in a developing country such as China, anorectoplasty is not yet routinely available in rural areas, and most of the PC newborns will undergo a colostomy before transferring them to a superior hospital. The stoma in different positions might make the placement of 3 mm trocar difficult in multi-incision laparoscopic surgery, further interfering with surgical performance. Nevertheless, in SILS, all trocars were placed in the umbilicus and the effect of stoma position on trocar setup was relatively small. Furthermore, those unaccustomed to SILS initially could adapt through strict training. Therefore, in the hands of an experienced pediatric surgeon, the SILAARP procedure would not be affected by the so-called drawbacks, and its operative performance would be similar to 3-PLAARP.
In laparoscopic-assisted anorectoplasty for the treatment of PC, careful patient selection is quite important. Cloacae with a CC shorter than 1 cm are treated almost like those who are born with a rectovestibular fistula and most of them can be treated with a posterior sagittal procedure. 16 For patients with a low rectal pouch, laparoscopy is also not required for these patients. For the urethra vaginoplasty procedure, our technique is also not suitable for a child with severe vaginal agenesis, presenting with a CC longer than 5 cm (meaning she always has a shorter common wall between the vagina and the urinary tract) or those without enough tissue to extend the urethra and vagina simultaneously. This is because the positional relationship between the end of the rectum and the pelvic floor muscles has a great influence on operative procedure. We use the terminal position of the rectum as an important index to distinguish the type of ARM. When the rectal pouch is above the pubococcygeal line (i.e., mid to high rectal pouch) for perineal surgical procedures such as posterior sagittal anorectoplasty, it might be hard to complete terminal rectum dissection to achieve tension-free anoplasty. It should be noted that, while many cloacae can also be repaired from a posterior sagittal incision alone without transabdominal access, with the help of laparoscopic-assisted surgery, surgeons can not only acquire excellent visualization of the pelvic cavity and adequately mobilize the gap between the rectum and the posterior wall of the CC but they can also reduce surgical trauma and achieve accurate placement of the rectum into the muscle complex8,17 (Fig. 4).
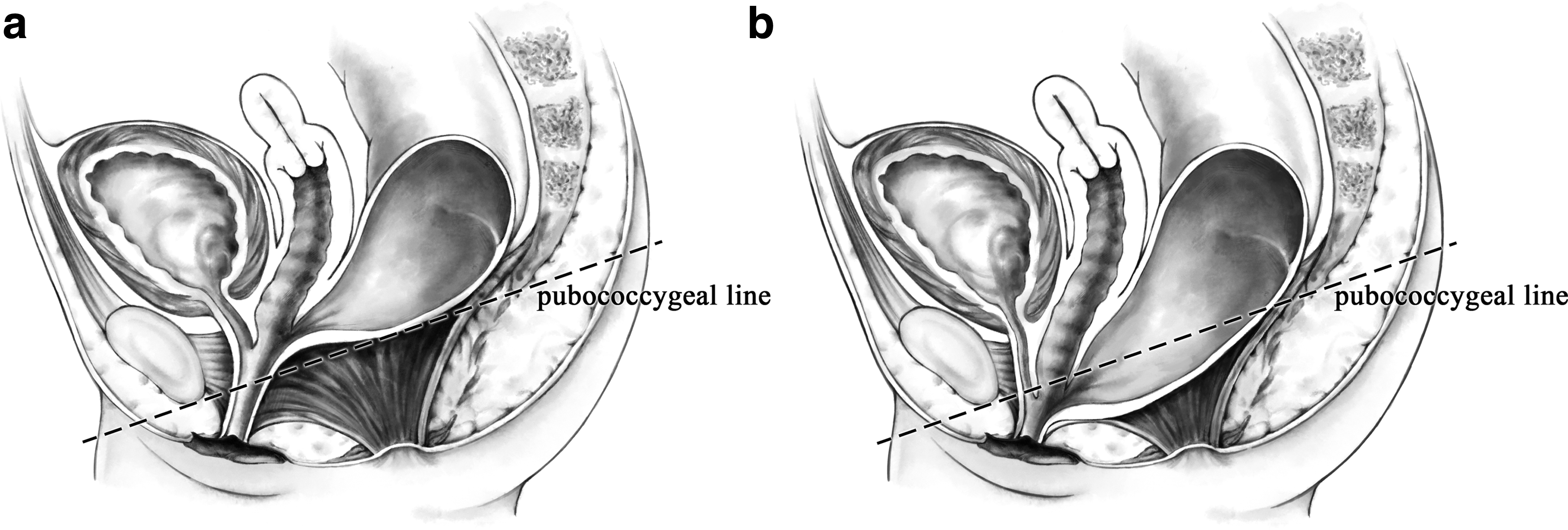
The relationship between the terminal position of the rectum and pubococcygeal line.
As with other researchers,18,19 we prefer to repair the entire cloacal defect at one setting rather than to delay the urogenital repair to a later date. It appears that the rectal component of PC is the easiest part to repair and some researchers might be tempted to repair only the rectal aspect and delay the urogenital work. However, definitive surgical reconstruction with one-stage surgery offers many benefits to the PC patients. First, the scarring and anatomical changes that might be left from first-stage repair could increase the difficulty of dissection and the risk of accidental injury to the surrounding tissue during later urethra vaginoplasty; one-stage surgery could avoid these disadvantages. Second, early initiation of toilet training for urine might be associated with early urinary continence and does not appear to be associated with bladder dysfunction, 20 hence, the one-stage surgery may be thought of as crucial for improving not merely bowel function but also bladder function during the corresponding period. Third, the one-stage surgery avoids physical and psychological stresses of repeated anesthesia and surgeries. Therefore, we commend repair of the entire cloacal defect simultaneously.
The incidence of complications was similar in both groups. Rectal prolapse occurred in 5 (20.0%) patients, more than reported in other studies with the rates of 2%–12%.21,22 This may be explained by the fact that younger children with flatter sacra usually have larger anorectal angles and weakness of the perianorectal tissue. Thus, we recommended carefully suturing the seromuscular layer of the rectum to the presacral fascia and appropriately excising excess terminal rectum. In our study, however, the symptoms of rectal prolapse were relatively mild and no patients required surgical interference.
In a systematic review of urinary tract function in PC, intermittent catheterization to empty the bladder was found in 42% (141/332) of patients and urinary incontinence developed in 23%. 23 In our series, however, only 1 (4.0%) patient required intermittent catherization (new-onset after surgery). Occasional urinary incontinence was discovered in only 2 (8.0%) children. This may be because our technique avoids the extensive dissection of the bladder neck and the anterior wall of the urethra, thus further minimizing destruction of bladder innervation. 8 A recent study reported that the total urogenital mobilization technique might lose limited urethra tissue and increase the risk of urinary leakage in some short urethra patients. 24 Indeed, the urethral length might be too short in these children to perform urethroplasty without tension using the traditional perineal procedure. Therefore, we recommend a urogenital separation technique that fully mobilizes the CC to lengthen the urethra for these short urethra patients; the urethral length should be an important indicator in cloacal reconstruction. Some researchers showed that sacral anomalies have not been as reliable for the prediction of urinary continence, development of neurogenic bladder, or need for intermittent catheterization.25–27 Interestingly, all the patients with urinary dysfunction in our study had varying degrees of spinal deformities, suggesting that the cause of the urine incontinence and need for intermittent catheterization may be associated with spinal abnormalities.
To achieve adequate anorectal function is an important goal for surgical reconstruction of cloacal malformations. There were reports regarding degrees of improvement in the bowel function in patients with ARMs appearing with age28–30 ; therefore, we disregarded the role of aging in relationship to bowel functional outcomes and chose 18 months postoperatively as a midterm follow-up time point to evaluate postoperative bowel function. There were no significant differences between groups in terms of anorectal function with regard to soiling and constipation.
A collective review 31 reported that 71% and 51% of the patients developed some degree of fecal soiling and constipation, respectively. In our cohort, soiling and constipation were found in 44% and 40%, respectively, when all children were analyzed together. The difference may be attributed to (1) the minimal damage to the sphincter muscles and tiny nerves during laparoscopic surgery; (2) inclusion and exclusion criteria for our study, suggesting well-selected children for our procedure; and (3) the resection of the megarectum in our procedure. Although all the specimens of megarectum had roughly normal ganglionic cells and myenteric plexus, we believed that this pathological change of the terminal rectum is an important factor in constipation. 32 Hence, we recommend removing dilated megarectums and rectums with weak peristaltic function; it is easier to remove the distended rectal pouch under the guidance of laparoscopy than with posterior sagittal anorectoplasty and laparotomy.
Moreover, it was reported that sacrovertebral status might have an impact on fecal prognosis of patients with ARM and PC.33,34 In the present study, sacral and spinal status were certainly key factors for soiling prognosis in patients with PC. However, although children with sacral and/or spinal malformations showed high incidence of constipation, the difference did not reach statistical significance, possibly because of the small sampling of patients (Table 3). Because of the limitation of sample sizes, these initial conclusions are worthy of further study.
Our study has some limitations. First, this was a single-center, retrospective, nonrandomized study, inevitably prone to selection bias. Second, the follow-up time was relatively short and the postoperative voluntary bowel movements were not assessed. Third, these two types of procedures were not performed at strictly the same periods, and surgical skills increase with time.
Conclusion
Our findings suggested that SILAARP was a potentially safe and effective procedure for PC children with mid- to high rectal pouches. SILAARP not only achieved better cosmetic results but it also achieved comparable perioperative and midterm outcomes as those who underwent 3-PLAARP. However, randomized controlled trials to compare SILAARP and 3-PLAARP for PC with a long follow-up time are needed to validate the true benefits of SILAARP. We propose that SILAARP is potentially an effective treatment option for children with PC.
Footnotes
Acknowledgments
The work was supported by the Department of Pediatric Surgery, Capital Institute of Pediatrics, Beijing, People's Republic of China. The authors thank Dr. Li Long and Dr. Cheng Wei for their support and mentorship.
Disclosure Statement
No competing financial interests exist.