
Abstract
Abstract
Background:
The value of laparoscopic liver resection (LLR) for difficult lesions (located in segments I, IVa, VII, and VIII) is still controversial nowadays. The aim of this study was to summarize quantitatively the evidence related to this issue.
Materials and Methods:
Two investigators independently searched the Medline, Embase, Science Citation Index Expanded, and Cochrane Library databases for eligible studies published before December 2017. The RevMan 5.3 software was utilized for statistical meta-analysis. Weighted mean differences (WMDs) and odds ratios (ORs) were calculated for continuous and dichotomous variables, respectively.
Results:
Five studies with a total number of 638 patients were included in the present meta-analysis, with 274 patients in the LLR group and 364 in the open liver resection (OLR) group. The LLR did not increase the operative time (WMD 12.42 minutes; 95% confidence interval [CI] −8.54 to 33.38 minutes; P = .25) or blood transfusion requirement (OR 0.81; 95% CI 0.40–1.64; P = .57) compared with OLR. Conversely, LLR was associated with significantly lower intraoperative blood loss (WMD −140.57 mL; 95% CI −203.39 to −77.76 mL; P < .001), shorter hospital stay (WMD −2.88 days; 95% CI −4.84 to −0.92 days; P = .004), and lower overall morbidity (OR 0.43; 95% CI 0.28–0.65; P < .001). The oncologic outcomes of R0 resection rate, surgical margin, and tumor recurrence were comparable in the two groups.
Conclusion:
LLR for difficult lesions in selected patients is safe, technically feasible, and advantageous when performed by experienced surgeons.
Introduction
The laparoscopy was first used for liver resection by Reich in 1991 during laparoscopic surgery for gynecologic symptoms. 1 Since then, laparoscopic liver resection (LLR) has been gradually introduced by hepatopancreaticobiliary surgeons worldwide due to its inherent advantages. The benefits of LLR included less blood loss, smaller incisions, lower postoperative morbidity, and shorter length of stay compared with open liver resection (OLR).2–4 At present, the total number of LLR worldwide has rapidly increased to more than 9000 cases. 4 Moreover, the minor LLRs which mainly included the anterior and inferior segments had been recommended to be a standard practice during the second international consensus conference held in Morioka. Nevertheless, laparoscopic major hepatectomies and LLRs for difficult lesions (segments 1, 4a, 7, and 8) were still considered as innovative procedures, which were reserved for surgeons with advanced experiences in LLRs. 5
The posterosuperior (PS) segments (segments 4a, 7, and 8) of the liver are deeply located in right subphrenic space and surrounded by the ribs and diaphragm, which are difficult to access through laparoscopic surgery. Thus, LLR for the PS segments could be more challenging and potentially more dangerous than other segmentectomies because of the limited visualization and difficulty in bleeding control. 6 Moreover, the newly proposed difficulty scoring system grades tumors in PS segments with the highest score.7,8 The caudate lobe is situated posteriorly to the liver and directly over the inferior vena cava, which is difficult to access and obtain a good view. In addition, an international survey suggested that surgeons performed LLR less frequently for the PS segments and caudate lobe than for other favorable segments. 9 These facts showed that LLR for difficult lesions should be considered a technically complex operation.
In recent years, with the advancements in the design of laparoscopic surgical instruments and the introduction of novel techniques (such as the use of an additional intercostal trocar), the laparoscopic resection of difficult lesions has been increasingly proposed as a safe and efficient method in appropriately selected patients.10–12 Recently, a meta-analysis 13 was performed to evaluate the safety and feasibility of LLR for difficult lesions by comparing perioperative results in patients undergoing PS and anterolateral procedures. Finally, the study revealed that LLR was technically feasible and safe for selected patients with lesions in the PS segments of the liver. Moreover, to assess the value of LLR for difficult lesions, several recent studies14–18 had directly compared LLR with OLR of lesion in these segments. However, some outcomes of these studies were conflicting due to the relatively small sample size of a single study. Nevertheless, the traditional OLR remains the standard procedure for tumor located in these segments at present. Therefore, the value of LLR for difficult lesions is still under debate. The purpose of this meta-analysis is to evaluate the safety and efficacy of LLR for difficult lesions compared to OLR.
Materials and Methods
Study design and literature search
This meta-analysis was designed according to the PRISMA guidelines, 19 and the PRISMA flow diagram is presented in Figure 1.

The literature search and study selection procedures according to the PRISMA statement.
Systematic searches for all articles published before December 2017 comparing LLR and OLR for difficult lesions were applied to the following electronic databases: Medline, Embase, Science Citation Index Expanded, and Cochrane Library. The following keywords were used: (LAPAROSCOPIC or MINIMALLY INVASIVE SURGERY), (HEPATECTOMY or LIVER RESECTION), (DIFFICULT LESION or POSTEROSUPERIOR or CAUDATE LOBE or SEGMENT1 or SEGMENT4a or SEGMENT7 or SEGMENT8 or INTER-COSTAL). The search was done with language restriction in English and for studies conducted on human subjects. The reference lists of reviews and retrieved articles were hand-searched simultaneously. Abstracts or unpublished reports were not considered.
Inclusion and exclusion criteria
We reviewed abstracts of all citations and retrieved studies. The criteria used to include published studies were as follows:
(1) Observational studies and/or randomized trials comparing LLR versus OLR for difficult lesions. (2) Clear definition of the difficult lesions (located in segments I, IVa, VII, and VIII). (3) The short-term and/or long-term outcomes were mentioned. (4) Sufficient data were presented to calculate the statistics.
The major reasons for exclusion of studies were as follows:
(1) Studies with no clearly reported outcomes of interest. (2) Duplicated studies.
Data extraction and quality assessment
Two investigators (F.L. and Q.L.) extracted information from all eligible publications independently according to the prespecified selection criteria listed above. Any disagreement was resolved by discussion. The following characteristics were collected from each study: the first author's name, year of publication, the country of participants, study design, location of the lesion, number of cases and controls, study population characteristics, surgical parameters, postoperative outcomes, oncological outcomes, and other such data. The quality of studies was assessed using the Newcastle–Ottawa Scale (NOS), 20 by examining three factors: patient selection, comparability of the study groups, and assessment of outcome. A score of 0–9 was allocated to each study based on these parameters, while studies achieving six or more scores were considered to be of higher quality. 21
Statistical analysis
The statistical analysis was performed by use of RevMan 5.3 software, which was provided by Cochrane Collaboration. Dichotomous variables were presented as the odds ratio (OR) with a 95% confidence interval (CI), while continuous variables were expressed with weighted mean difference (WMD) and 95% CI. A P < .05 was considered statistically significant. For some studies without mean and standard deviation, we calculated them by the sample size, median, and range under the guidances of the literatures.22,23 Both the Cochran's Q statistic 24 to test for heterogeneity and the I2 statistic to quantify the proportion of the total variation due to heterogeneity 25 were calculated. A P value of more than the nominal level of 0.10 for the Q statistic indicated a lack of heterogeneity across studies, allowing for the use of a fixed-effects model (the Mantel–Haenszel method) 26 ; otherwise, the random-effects model (the DerSimonian and Laird method) was used. 27 Several methods were used to assess the potential publication bias. Visual inspection of funnel plot asymmetry was conducted. The Begg's rank correlation method 28 and the Egger's weighted regression method 29 were used to statistically assess publication bias (A P < .05 was considered statistically significant).
Results
Study and patient characteristics
A total of 261 published studies were initially presented (Fig. 1) after searching the electronic databases. Through the steps of removing duplicates, screening the title, reading the abstract, and reading the entire article, seven potentially eligible studies were left. However, two studies which compared LLR versus OLR for hepatocellular carcinoma (HCC) located in the right-posterior segments were excluded because the HCC was located in both segment VI and VII. Finally, five studies14–18 which included a total of 836 cases were found to match our inclusion criteria. Studies had been carried out during 2015–2017 in China, Korea, Belgium/Canada, multiple European countries, and the United States. The types of studies included retrospective cohort and propensity score matching studies from single and multiple centers. Overall quality of the included studies was of good quality that the NOS scores varied between 7 and 8. The detailed characteristics of studies included in the meta-analysis are presented in Table 1.
Characteristics of Studies Included in this Meta-Analysis
Lap, laparoscopic; NA, not available; NOS, Newcastle–Ottawa scale; PSM, propensity score matching.
The characteristics of patients included in the meta-analysis are summarized in Table 2. The five studies included 274 patients in the LLR group and 364 patients in the OLR group. The indications for operation were HCC, colorectal liver metastasis, central cholangiocarcinoma, noncolorectal liver metastases, other malignant tumors, and benign lesions. Cumulative reported conversion rates in the LLR groups were 2.6% (7/274). There is no in-hospital mortality in the LLR group, while the mortality rate was 0.55% (2/364) in the OLR group. During the follow-up period, malignancies recurred in 47.8% (55/115) of the patients in the LLR group and 36.5% (42/115) of the patients in the OLR group.
Patient Characteristics (Laparoscopic Versus Open Liver Resection)
ASA, American Society of Anesthesiologists; BMI, body mass index; CCC, central cholangiocarcinoma; CLM, colorectal liver metastasis; F, female; HCC, hepatocellular carcinoma; M, male; NA, not available; NCLM, noncolorectal liver metastases.
Quantitative data synthesis
Operative outcomes
The literatures reported operative outcomes which mainly included the operative time, blood loss, and the rate of blood transfusion. With regard to operative time, five retrospective studies,14–18 including 274 LLRs and 364 OLRs, were estimated. The test for heterogeneity among studies was statistically significant (P = .08, I2 = 52%), so the random-effects model was used. The combined results based on the above studies showed that the LLR did not increase the operative time (WMD 12.42 minutes; 95% CI −8.54 to 33.38 minutes; P = .25; Fig. 2A). Nevertheless, the pooled results showed that the intraoperative blood loss was significantly lower in LLR group than that in OLR group (trials: 5; WMDfixed −140.57 mL; 95% CI −203.39 to −77.76 mL; P < .001, Fig. 2B). There were four studies15–18 which had been performed to focus on the rate of blood transfusion for patients undergoing LLR and OLR. The study of Scuderi et al. 14 was excluded from the analysis because the transfusion rate was not available for this analysis. The test for heterogeneity among studies was not statistically significant (P = .44, I2 = 0%), so the fixed-effects model was used. There was no significant difference in transfusion rate between the two ways of treatments when the four studies were analyzed (OR 0.81; 95% CI 0.40–1.64; P = .57, Fig. 2C).
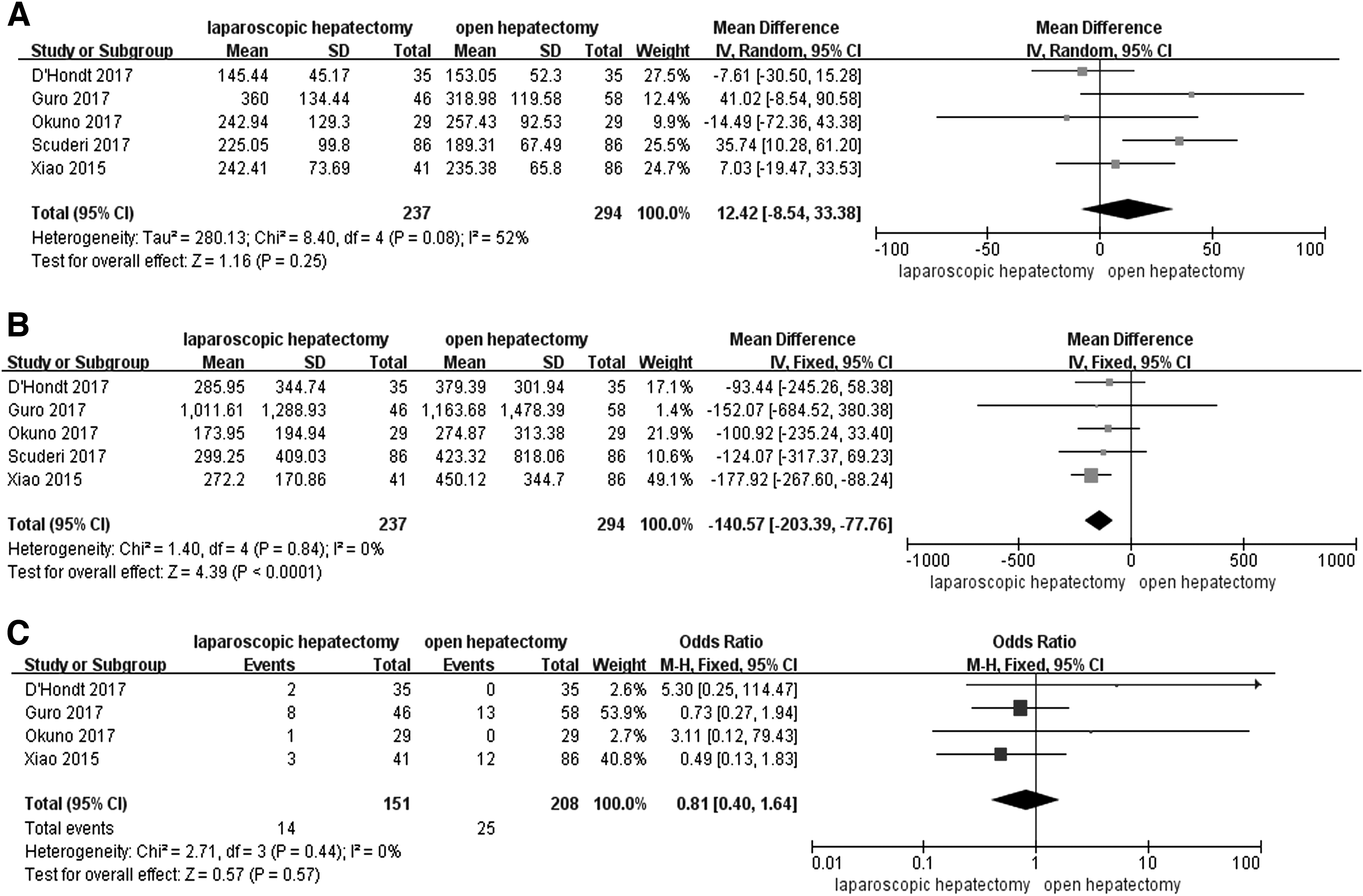
Forest plots displayed intraoperative outcomes of LLR versus OLR for difficult lesions:
Postoperative outcomes
In postoperative overall complication analysis, five retrospective studies,14–18 including 274 patients in LLR group and 364 patients in OLR group, were estimated. In the LLR group, postoperative overall complications ranged from 14.0% to 25.7% compared with a range from 27.9% to 41.4% in the OLR group. The test for heterogeneity among studies was not statistically significant (P = .84, I2 = 0%), so the fixed-effects model was used. The combined results based on the above studies showed that the postoperative overall morbidity in the LLR group was significantly lower than that in OLR group (OR 0.43; 95% CI 0.28–0.65; P < .001; Fig. 3A). According to Clavien–Dindo grade, we also pay attentions to the complications with Clavien–Dindo grade III and above. The pooled results showed that the difference of complications with Clavien–Dindo grade III and above between the two groups was not statistically significant (trials: 5; ORfixed 0.53; 95% CI 0.27–1.04; P = .06). Moreover, the pooled results showed that the hospital stay was significantly shorter in LLR group than in OLR group (trials: 5; WMDrandom −2.88 days; 95% CI −4.84 to −0.92 days; P = .004; Fig. 3B).
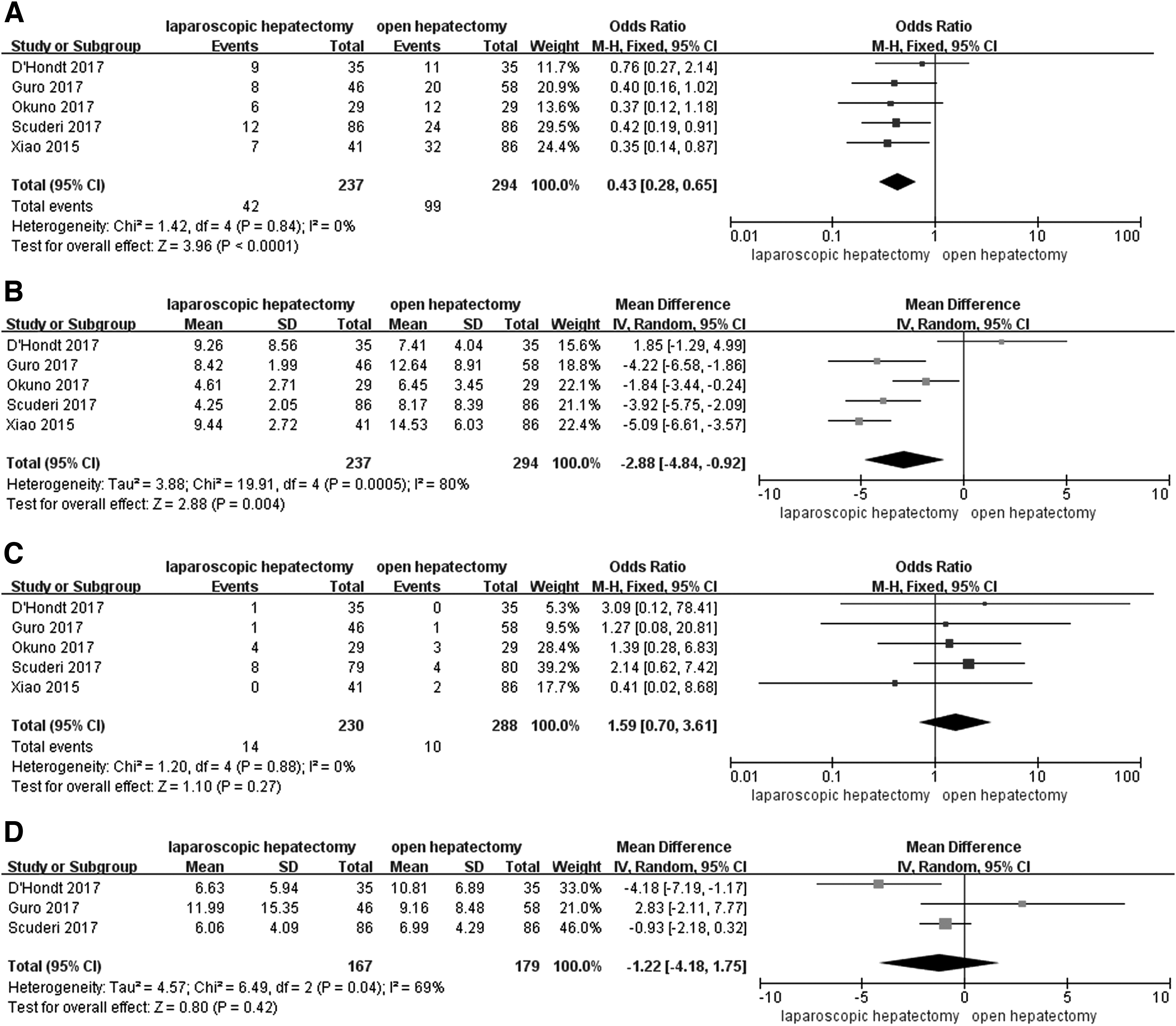
Forest plots displayed postoperative and oncologic outcomes of LLR versus OLR for difficult lesions:
Oncologic outcomes
With regard to R0 resection, five retrospective studies,14–18 including 274 patients in LLR and 364 patients in OLR, were estimated. The test for heterogeneity among studies was not statistically significant (P = .88, I2 = 0%), so the fixed-effects model was used. There was no significant difference in R0 resection rate between the two ways of treatments when the five studies were analyzed (OR 1.59; 95% CI 0.70–3.61; P = .27, Fig. 3C). Furthermore, meta-analysis of the pooled data showed that the surgical margin was also comparable in the two groups (trials: 3; WMDrandom −1.22 mm; 95% CI −4.18 to 1.75 mm; P = .42; Fig. 3D). The data on tumor recurrence were available in only two studies.14,18 The pooled results showed that there was no significant difference in the rate of tumor recurrence (OR 1.78; 95% CI 0.99–3.22; P = .06).
Publication bias
Funnel plot and Begg's and Egger's tests were performed to evaluate publication bias of the included literatures. Figure 4 displayed funnel plot that was based on the operative time in the meta-analysis. The shape of funnel plots did not reveal any evidence of funnel plot asymmetry. The statistical results still did not show publication bias (Begg's test: P = 1.00; Egger's test: P = .73).

Funnel plot of the operative time in the included studies showing no evidence of publication bias. The circles were symmetrically distributed at the two sides of the dotted line, which suggested no evidence of publication bias.
Discussion
LLR for difficult lesions is a challenging technique for surgeons owing to the limited working space, difficulties in evaluating the resection margin, and control of bleeding. In earlier studies, patients with lesions in PS segments had been considered poor candidates for LLR.30,31 In recent years, with the introduction of novel techniques, such as the left lateral decubitus position and the use of an additional intercostal trocar, the laparoscopic resection of the difficult lesions had been increasingly proposed as a safe and efficient method in appropriately selected patients.10–12 Nevertheless, the traditional OLR remains the standard procedure for tumor located in the PS segments at present. For new surgical procedures to become widely adopted as standard operations, they should first be compared with established procedures and shown to be superior in at least some respects. 32 Therefore, several recent studies14–18 had directly compared LLR with OLR for difficult lesions. However, most of the studies were retrospective with a small number of patients, which may have insufficient statistical power to detect the effect or may have generated a fluctuated risk estimate. To derive a more comprehensive estimation of the value of LLR for difficult lesions, we have endeavored to pool all the relevant available data and perform a meta-analysis.
The present meta-analysis quantitatively summarizes the evidence related to the safety and efficacy of LLR for lesions located in difficult liver segments. To the best of our knowledge, the present study is the first meta-analysis to compare intraoperative, postoperative, and oncologic outcomes between LLR and OLR for difficult lesions. The results from this analysis suggested that LLR could be successfully completed in most of patients by experienced surgeons, with a lower rate of conversion to open surgery (cumulative rate 2.6%). Meanwhile, we found that the LLR did not increase the operative time or blood transfusion requirement compared with OLR. Conversely, LLR for difficult lesions was associated with significantly lower intraoperative blood loss, shorter hospital stay, and lower overall morbidity. Moreover, the oncological outcomes of R0 resection rate, surgical margin, and tumor recurrence were comparable in the two ways of treatments. These results indicated that LLR for difficult lesions in selected patients was technically feasible and associated with a series of advantages.
Consistent with some previous meta-analysis studies33,34 which compared the outcomes of laparoscopic versus OLR, we found that there was no significant difference in the mean operative time between the two groups. Although initially laparoscopic resections were more time consuming, evolution in parenchyma-transecting devices along with laparoscopic proficiency had resulted in shorter resection times. 34 Furthermore, the operative time of laparoscopic resection in cirrhotic patients was longer than open approach because transection of hepatic parenchyma needed to proceed with caution due to the fear of bleeding, which had been confirmed by our previous study. 35 Nevertheless, the proportion of patients with cirrhosis in both LLR and OLR groups in the current study was relatively low (30.8% versus 34.9%, respectively, Table 2), which may have little effect on the operative time. In addition, the deep learning curve of LLR may also affect the operative time. A previous study on learning curve had recommended at least 45–75 cases to ensure stability in performing major LLR. 36 However, the LLRs included in this meta-analysis were mainly performed by experienced surgeons from high volume centers, for whom the learning curve of LLR had passed during the research period.
Bleeding control was one of technical challenges associated with laparoscopic resection of the difficult lesions because of the poor visualization and limited working space. Interestingly, the pooled results showed that the intraoperative blood loss was significantly lower in LLR group than that in OLR group. The similar outcome of decreased blood loss with the laparoscopic approach had been reported in most of previous studies but not in difficult lesions. The following possible reasons for this should be noticed. First, the laparoscope could offer a magnified view in LLR. The caudal–cranial transection of the hepatic parenchyma with magnification in LLR might result in better identification of intraparenchymal vascular structures compared to the open anterior approach. 17 Second, the raised intra-abdominal pressure from pneumoperitoneum in LLR also contributed to less blood loss. Because hemorrhage during hepatectomy was mainly due to damage of the vessels from the hepatic vein inside the liver parenchyma,37,38 the CO2 pneumoperitoneum in LLR was advantageous to the reduction of venous bleeding from the cut surface. Furthermore, the especial patient position in LLR may also result in decreased blood loss. The patients were always placed in a semiprone position or left lateral decubitus position when the laparoscopic approach was used for liver resection in PS segments.14–18 Under the circumstances, the right hepatic vein was in a higher position than the inferior vena cava, which will reduce bleeding from right hepatic vein in LLR for the PS segments. 32
There are increasing evidences to suggest that LLR was associated with less postoperative morbidity, even for difficult lesions.14,15,39 The pooled data in this study also showed that the overall rate of postoperative complications were significantly lower in patients who underwent LLR than OLR for difficult lesions. As reported by the literature, 40 cut surface fluid collection was the most common complication after resection of these segments, because these segments of the liver are located deep within the liver and between the liver and the diaphragm. Moreover, this kind of complication can lead to other related complications, such as reactive pleural effusion, atelectasis, and cut surface infections. To obtain good access, OLR for PS segments requires a large skin incision that extends to the patient's right side, and sometimes the combination of a large laparotomy and thoracotomy incision was needed. 41 Nevertheless, LLR for PS segments caused milder postoperative pain because of less invasiveness in the abdominal wall, which allowed patients to resume walking activity earlier after surgery. The early mobilization of the patient after LLR can facilitate drainage of cut surface effusion, thereby reducing the incidence of postoperative cut surface effusion. 15 Moreover, laparoscopic operations have the advantages of preservation of the abdominal wall collaterals and less manipulation, which may lead to decrease the incidence of postoperative ascites, 14 especially for cirrhotic patients. In addition, reduced complications and early ambulation after surgery were contributed to a shorter hospital stay in the LLR group.
There was a main concern that LLR for difficult lesions would decrease the tumor-free surgical margin because of limited working space and the lack of palpation. However, the results of the current meta-analysis found that there was no significant difference between the LLR and OLR groups regarding the surgical margin or R0 resection rate. Moreover, no significant difference in tumor recurrence rate was observed between the two groups. The satisfactory results of the oncologic outcomes would be contributed to the routine use of intraoperative ultrasonography in both LLR and OLR, which could provide a precise evaluation of tumor location and the information of borders for nontumorous tissue, hence obtaining an adequate tumor-free margin. 42
In this study, several limitations need to be addressed. First, all of the studies included were retrospective trials, although some trials were multicentric and propensity score matching studies. The retrospective nature inevitably adds a degree of selection bias to the results and can lead to over/underestimation of the measured effect. Second, some between-study heterogeneity was observed in certain outcome comparisons. Although the random-effects model was used to diminish the effects of the observed heterogeneity, it was impossible to investigate the source of heterogeneity using meta-regression method due to the small number of studies. Last but not least, the indications of LLR and OLR for PS was inhomogeneous, including HCC, colorectal liver metastasis, central cholangiocarcinoma, noncolorectal liver metastases, other malignant tumors, and benign lesions. However, our study was indispensable because quantitative data summarizing LLR versus OLR for difficult lesions are scarce at present.
In conclusion, the results of this comprehensive meta-analysis indicated that LLR for difficult lesions was technically feasible and as safe as OLR. Moreover, LLR for these segments could offer comparable oncologic outcomes as OLR, while being associated with a series of advantages in short-term outcomes. Certainly, these results of the LLR for difficult lesions were based on appropriately selected patients and experienced surgeons in high volume centers. Further studies with well-designed (randomized controlled trials) and a larger sample size are needed to confirm our results.
Footnotes
Disclosure Statement
No competing financial interests exist.