
Abstract
Abstract
Objective:
To report our institutional experience with radiotracer-assisted localization of lung nodules (RALN) in combination with uniportal video-assisted thoracoscopic surgery (UVATS).
Methods:
We retrospectively reviewed electronic medical records and radiology images of 27 consecutive adult patients who underwent planned UVATS lung resections combined with RALN from January 2014 to May 2017. Based on preoperative imaging, 29 nondescript nodules were marked with technetium 99 m macroaggregated albumin under computed tomography guidance before resection. Perioperative outcomes were analyzed.
Results:
All 29 nodules were successfully marked and resected with negative margins by UVATS; 12 (41.5%) were pure ground-glass opacities. Three patients had prior ipsilateral lung resections. There were no conversions to multiport VATS or thoracotomy. The majority (86.5%) of the nodules were malignant. The median nodule size was 8 mm (range: 3–20 mm) and depth, 56 mm (range: 22–150 mm). The majority (21/27; 77.8%) of patients underwent wedge resections alone, while 6 patients had anatomical resections. Median times were as follows: radiotracer injection to surgery, 219 minutes (range: 139–487 minutes); operative time, 85.5 minutes (32–236 minutes); chest tube removal, 1 day (range: 1–2 days); and length of stay, 2 days (range: 1–4 days). Four patients (14.8%) had a pigtail catheter placed for pneumothorax after radiotracer injection. One patient was readmitted 1 week after discharge for a spontaneous pneumothorax. There were no other morbidities or any 90-day mortality.
Conclusion:
RALN can be combined with UVATS to effectively resect small, deep, or low-density lung lesions that are difficult to visualize or palpate by thoracoscopy.
Introduction
Uniportal video-assisted thoracoscopic surgery (UVATS) is gaining popularity worldwide as a minimally invasive technique to perform advanced pulmonary resections through a single-incision without the morbidity of a thoracotomy.1,2 While the spectrum of operations that can be done via UVATS has increased over time, 3 there are still certain challenges to be overcome when using this approach.
One limitation of thoracoscopy in general that is compounded by UVATS is the intraoperative localization of nondescript lung lesions. To facilitate the resection of such lesions using multiportal VATS (MVATS), various localization techniques have been developed and are well described in the medical literature. The more popular of these techniques include imaging or navigational bronchoscopy-guided placement of markers such as fiducials, 4 hook wires, 5 microcoils,6,7 and injection of dyes, 8 and radioactive tracers.9–11 On the contrary, there is very limited published data12–14 regarding the utility of these techniques during UVATS.
The purpose of this study was to evaluate our institutional experience with the novel combination of radiotracer-assisted localization of lung nodules (RALN) using technetium 99 m labeled macroaggregated albumin (99Tc-MAA) and UVATS, which to the best of our knowledge has not been described before.
Materials and Methods
The project was approved by the Mayo Clinic Institutional Review Board and informed consent was waived due to minimal risk. From January 2014 to May 2017, 27 consecutive combined RALN and UVATS operations were performed at Mayo Clinic in Jacksonville, Florida by 1 surgeon (M.T.). Electronic health records of these patients, including radiology images, were reviewed retrospectively. Our indication for localization is determined by the surgeon's estimate of the difficulty in completing the procedure by any thoracoscopic technique, whether UVATS or MVATS. These include the following lesions:
primarily ground-glass in nature, too deep for digital palpation and not expected to be easily visible on thoracoscopy, close to intersegmental boundaries when segmentectomies are considered, adjacent to other lesions that could interfere with thoracoscopic localization when a specific nodule is targeted for resection, likely to be obscured by severe pleural adhesions or scarring.
All operations were planned as UVATS with the patient's informed consent to convert to MVATS or thoracotomy if necessary. Patient variables that were collected included demographics, smoking history, body mass index (BMI), Charlson comorbidity scores, and lung function tests (forced expiratory volume in 1 minute and diffusing lung capacity for carbon monoxide). Variables related to the pulmonary lesions included size, density, and depth (the perpendicular distance from the skin at the level of the planned UVATS incision) as seen on preoperative computed tomography (CT) scans, and surgical pathology. The perioperative variables collected included time from tracer injection to surgery, operative times, type of resection performed, and complications.
Techniques
Preoperative radiotracer localization
Percutaneous CT-guided injection of the radiotracer is performed in the interventional radiology CT suite by a group of board-certified interventional radiologists (G.F., J.M., R.P., D.S., and B.T.) who follow an institutional protocol (Appendix). Radiotracer localization is performed the same day in the morning, before the scheduled surgery. Communication between the surgeon and the interventional radiologist is critical to confirm the location and number of lesions to be localized. This communication between surgeon and interventional radiologist is accomplished by phone call, e-mail, or electronic medical record messaging. Communication typically includes the date, series number, and image number of lesions to be localized.
Before radiotracer localization, a limited noncontrast CT of the thorax is performed to confirm the target (Fig. 1). CT imaging is performed on a Siemens Definition AS CT scanner at 120 mA, 120 kV, and slice reconstruction thickness of 5 mm. Scanner-specific dose optimization techniques are utilized. Local anesthetic is then administered to the chest wall and parietal pleura. Under intermittent CT fluoroscopic guidance (50 mA, 120 kV) and with sterile precautions, a 21-gauge Chiba needle is advanced just deep to the target lesion and 300 μCi 99Tc-MAA in 0.2 mL saline are injected into the lung parenchyma. The needle is then removed utilizing radioactive contamination precautions and a sterile dressing applied.
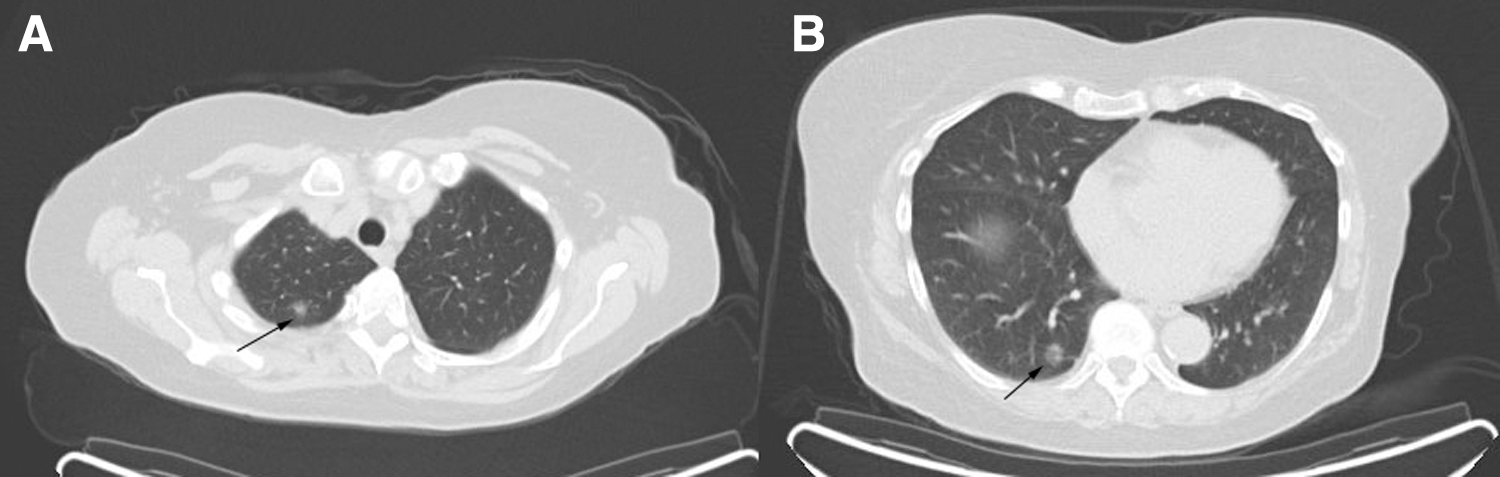
Preoperative computed tomography scan of the same patient showing two pulmonary nodules (arrows) in the right
CT fluoroscopic and/or helical imaging is utilized to evaluate for postlocalization pneumothorax or hemorrhage. If a significant (>20%) or symptomatic pneumothorax is present, a 10F pigtail catheter is placed in the affected pleural space and connected to a water-seal drainage system. Anteroposterior and lateral nuclear scintigrams (Philips BrightView XCT or Siemens Symbia; 300 seconds per image) are obtained to confirm focal intraparenchymal pulmonary placement of the radiotracer and exclude significant intravascular injection (Fig. 2).
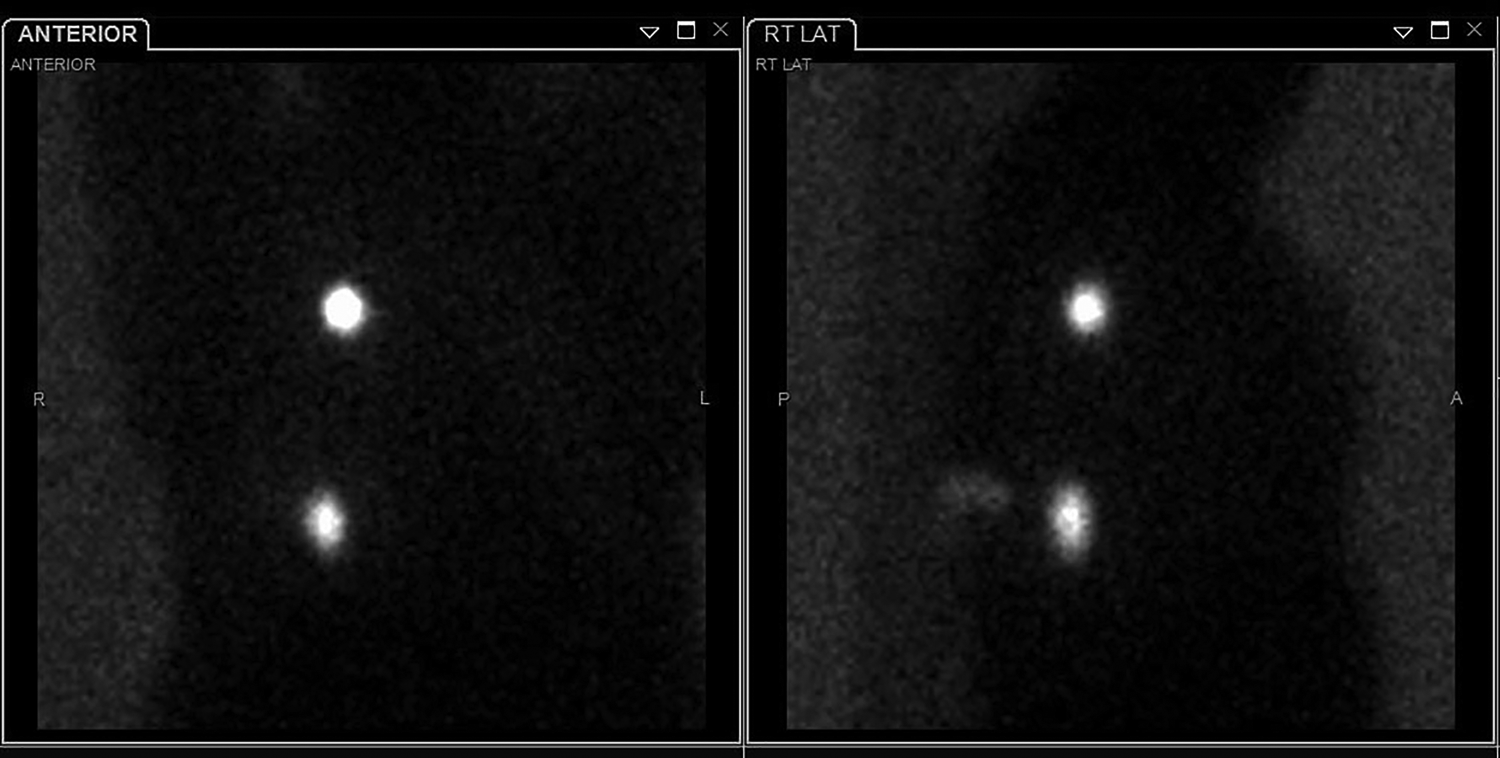
Scintigrams of the patient in Figure 1 immediately after radiotracer injection showing the well-localized radiotracer in the upper and lower lobes of the lung.
Surgical technique
Following radiotracer injection and scintigram, the patient is transported directly to the preoperative holding area and from there to the operating room at the earliest availability.
All UVATS operations at our institution are performed under general anesthesia and with single-lung ventilation. With the patient in a lateral decubitus position, a 3-cm incision is made in the 5th intercostal space between the anterior and midaxillary lines. A soft tissue wound protector (Alexis Wound Protector/Retractor™; Applied Medical Technology, Rancho Santa Margarita, CA) is used to prevent smudging of the camera. A 5 mm or 10 mm thoracoscope is then used to assess if the nodule can be visualized or palpated. A 31-cm long gamma radioactivity probe with a 30-degree angled head (Daniel Probe™; Dilon Diagnostics, Newport News, VA) covered with a sterile sheath and connected to a gamma-detector (Navigator GPS™ System; Dilon Diagnostics, Newport News, VA) is used to locate the area in the lung with the highest signal intensity (Fig. 3) under thoracoscopic visualization. This area is then marked either with a blue surgical marker or by superficially scoring with a long electrocautery knife. An automated stapling device (i-drive™; Covidien, Minneapolis, MN) is used to clamp the lung along the line of resection. To ensure that adequate negative margins are obtained, the stapler is fired while frequently using the gamma probe to confirm that the intensity of the radio signals in the nonresected lung are <10% of the highest signal.
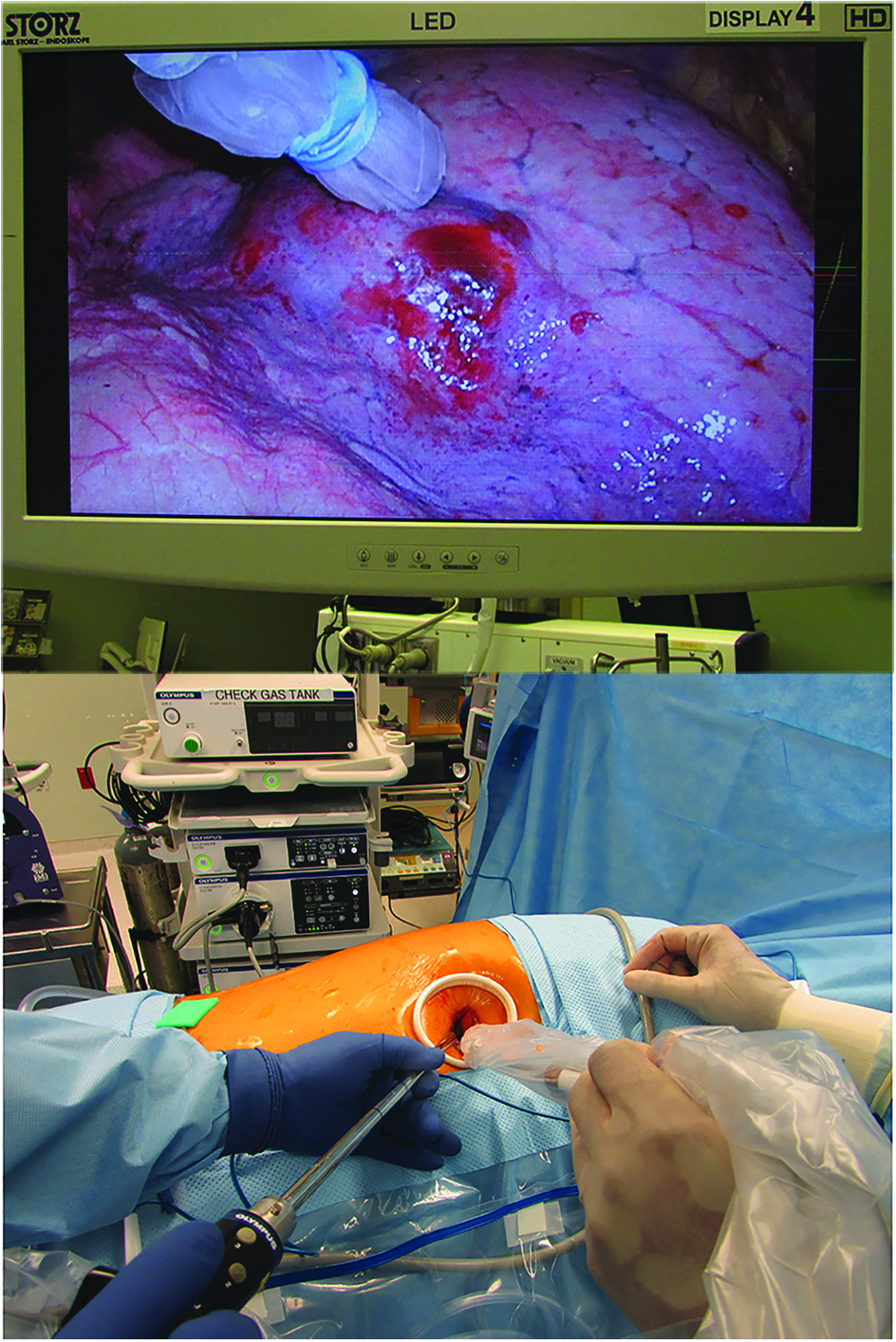
Intraoperative photograph of uniportal video-assisted thoracoscopic surgery technique using long angled gamma probe for localization of radiolabeled lung nodule.
A wedge resection is performed initially if adequate negative margins can be obtained; otherwise, a segmentectomy or lobectomy is considered. All specimens are then sent for intraoperative frozen section for diagnosis and margin analysis. Further resection and nodal dissection are performed as indicated, depending on the pathological diagnosis and adequacy of negative margin. We consider a negative margin of ≥2 times the size of the nodule in the case of primary lung cancer and >1 mm in the case of metastatic lesions to be adequate.
Results
Patient and nodule characteristics are shown in Table 1. A total of 29 lesions in 27 patients were marked with radiotracer injection, 100% of which were identified successfully and completely resected with microscopically negative margins (R0) via UVATS. Two patients had two separate ground-glass opacities (GGOs) in different ipsilateral lobes that were each marked with the radiotracer and resected at the same time.
Patient and Nodule Characteristics
BMI, body mass index; DLCO, diffusing lung capacity for carbon monoxide; FEV1, forced expiratory volume in 1 minute.
The tracer was focally present in the lung in all cases without any spillages into the pleural cavity. There were no conversions to either MVATS or thoracotomy. The median size of the nodules was 8 mm (range: 3–20 mm) and median depth was 56 mm (range: 22–150 mm); 12 (41.4%) nodules had a pure ground-glass appearance. Additional malignant micronodules that were not visible on preoperative CT scans were identified during pathologic examination of the resected specimens in 2 patients. The estimated upper limit of 95% confidence interval (CI) for 0 failed localization in 27 patients was 12%.
Three patients had previous ipsilateral lung resections, 2 of which had been done with UVATS. One patient underwent a right lower lobe wedge resection 18 months after previous UVATS right middle lobectomy for a stage 1a lung adenocarcinoma. Another patient who had a BMI of 51 and a history of colorectal cancer had undergone an attempt to resect a 9 mm right upper lobe nodule by UVATS without localization; the only nodule that could be identified and resected was a 9 mm, benign, intraparenchymal lymph node in the upper lobe. After a follow-up, CT scan 3 months later showed the initial nodule to be still present, and he underwent UVATS reoperation with RALN, with successful localization of the nodule, which was pathologically consistent with metastases from colorectal cancer.
The 3rd patient had a previous extensive chest wall and partial left lung resection via bilateral clamshell thoracotomy for a large mediastinal sarcoma and had extensive reconstruction of the chest wall followed by radiation. A year later, she developed a 7 mm metastatic left lower lobe nodule posteriorly, which, in our opinion, would have been challenging to localize even with a redo thoracotomy due to the extensive adhesions and pleural scarring tissue that were encountered. In her case, instead of the routine anterior UVATS incision, a 3 cm UVATS incision was made in the midaxillary line in the 8th intercostal space, through which the nodule was resected.
The majority (21/27; 77.8%) of patients underwent wedge resections alone, while anatomical resections were performed in 6 patients. These included four primary segmentectomies, one completion segmentectomies, and one completion lobectomy (Table 2). The RALN was used in three of the primary segmentectomies (one medial basal and two lower lobe superior segments) with deep GGOs to not only confirm their location but also to direct our line of resection. In the 4th patient, a diagnostic wedge resection of a nonpalpable GGO was initially planned, but based on the location of the RALN, we decided to perform a lower lobe superior segmentectomy upfront to ensure adequate margins. Even though the staple line did not traverse the nodule itself in any patient, additional staple line resections were performed in 2 patients to obtain a wider negative margin.
Type of Surgical Resections
UVATS, uniportal video-assisted thoracoscopic surgery.
In all patients with primary lung cancers, a complete lymph node dissection was performed. The majority of nodules (25/29; 86.2%; 95% CI 0.69–0.95) were confirmed to be malignant on final pathology; 24 out of 27 patients (88.9%; 95% CI 0.72–0.96) had confirmed malignancies.
Perioperative outcomes including complications
The median time from injection of the radiotracer to surgery was 219 minutes (range: 139–487 minutes) (Table 3). 99Tc-MAA has a half-life of 6 hours, and in 1 case that was delayed for 8 hours, no technical difficulty was encountered in localizing the nodule. The majority of patients (21/27; 77.8%) had their chest tubes removed on the postoperative day (POD) 1 and all the rest on POD 2.
Perioperative Variables
POD, postoperative day.
A significant pneumothorax was seen in 4 patients (14.8%) after radiotracer injection, and they all had pigtail catheters placed in the interventional radiology suite before surgery. One patient with severe emphysema who had undergone a wedge resection was readmitted 1 week after discharge for a sudden pneumothorax and required a chest tube. There were no other minor or major postoperative complications, including deaths in the first 90 days after surgery.
Discussion
The likelihood of successful resection of lung lesions via any minimally invasive surgical technique depends on a number of factors, including the size, depth, location, and density of the lesion. Small, deep, and low-density nodules and GGOs can often be difficult to visualize or locate with thoracoscopic instruments or by digital palpation. Failure to localize during VATS frequently requires conversion to a thoracotomy in 54%–63% of cases as reported by Suzuki et al. 15 Because of the spatial and visual limitations 16 encountered when attempting to palpate the lung through a single small incision, localization of nondescript lesions can be even more challenging with UVATS as we ourselves experienced in one of our morbidly obese patients described earlier.
When difficulty in localizing such lesions is anticipated based on preoperative imaging, the options include delaying resection until the lesion reaches a more tangible size and density, or using a localization technique. Our experience using RALN combined with UVATS shows that the technique is very safe and highly accurate in localizing poorly defined lung lesions. We were able to consistently resect the target nodule with negative margins using the combined technique without converting to MVATS or thoracotomy.
RALN is not a new technique and was first described by Chella et al., 17 who used 99Tc-labeled human serum albumin as a radioactive tracer for lung lesions. The same group then reported their 13-year experience using this technique in 211 patients with 99% success in localizing the lesion. 18 Due to the unavailability of human serum albumin in the United States, Daniel et al. 19 modified this technique and used 99Tc-MAA in humans for the same purpose. They later reported 99Tc-MAA to be an excellent radiotracer for lung lesions secondary to the larger size of the albumin particles (10–50 μm), which reduced the size of the inoculum and hence the radiation dose (0.1 mL/0.3 mCi); in addition there was slower dispersal of the radiotracer, allowing localization up to 18 hours later. 20 Since then, many other authors have reported using 99Tc-MAA for localization in MVATS with excellent results.10,21
One particular advantage of RALN compared to other localization techniques is that it is not necessary to infiltrate the target lesion directly and the radiotracer only needs to be injected close to the lesion. This allows the localization of lesions that may not be amenable to percutaneous lung biopsies because of their difficult location, such as under a rib or the scapula. We have also found the long narrow thoracic gamma probe used in RALN to be particularly suited for UVATS, as it can be easily placed alongside the camera in the single incision, and the angled head enables examination of the lung from different angles, even in deep recesses.
A true comparison between RALN and other localization techniques in UVATS is difficult due to the limited published data available in this area. To the best of our knowledge, only two other localization techniques using palpable microcoils 12 and patent blue dye 13 have been described in combination with UVATS in a large series of patients. While these techniques have been reported to have high success rates in localizing nodules closer to the periphery of the lung, unlike RALN, they have limited utility for lesions that are deep in the parenchyma or in areas of the lung that are hard to visualize. 5 In comparison, the deepest nodule localized with RALN in our patient cohort was located 15 cm from the skin incision.
The microcoil palpation technique described by Shi et al. 12 requires initial blind digital palpation, which in our opinion can not only be challenging but could also potentially dislodge the microcoil marker. As for the blue dye technique, inadvertent spillage into the pleural space not only defeats the purpose of localization but also causes discoloration of the entire pleural cavity and visceral pleura,22,23 which can be very disconcerting to the surgeon. On the contrary, if the radiotracer is spilled into the pleural cavity during RALN, the nodule can still be localized in the same setting by injecting additional quantities of radiotracer into the lung parenchyma. Intraoperatively, the pleural space is then irrigated with sterile water or saline to flush out the spilled tracer until the radio signals are minimal and the operation can then continue as planned.18,20
RALN does not require intraoperative fluoroscopy, CT scans, or large sophisticated equipment and is not subject to the risks of displacement of the marker due to coughing or lung movement unlike other localization techniques that use fiducials,24,25 intraparenchymal coils, or dyes. The overall radiation exposure to operating room and laboratory personnel is also very limited with RALN compared to intraoperative fluoroscopy or CT imaging.
Our study has some limitations that are mainly related to its retrospective nonrandomized nature and small size. The estimated upper bound of 95% CIs for 0 failed localization in 27 patients was 12%, indicating that larger studies are needed to confirm or refute our results. Nevertheless, we believe that it contributes significantly to the body of literature as the first reported study on the utility of combining RALN and UVATS.
Although RALN has shown to be safe and effective, it carries an inherent risk of pneumothorax and hemorrhage as with any other percutaneous intervention. Our reported rate of significant pneumothorax (14.8%) is less than the reported rate of 20%–33% for other non-RALN localization techniques 13 and comparable to the reported 5%–30% for RALN and MVATS.18,21,26 However, this complication was easily managed with a small pigtail catheter placed in the interventional radiology suite and did not adversely affect the postoperative course of the patients.
Failure to localize as a result of spillage of the radiotracer into the pleural cavity or chest wall has been described,18,20,26 although we did not encounter this issue. The radioactivity may also not be detectable if the radiotracer is inadvertently injected into a blood vessel or a central bronchus. We limit the procedure to be done by expert interventional radiologists who are familiar with the technique, which has helped us avoid these technical issues. Other limitations of RALN are related to the need for a specialized probe and a navigator, although these are easily acquired and relatively inexpensive compared to the equipment needed for the other localization techniques.
Conclusion
Low-density, deep, or small lung lesions can be effectively resected by UVATS when combined with CT-guided radiotracer localization. This technique can be useful in completing minimally invasive resection when difficulty in localizing the nodule via thoracoscopy is anticipated.
Footnotes
Acknowledgments
No funding was available for this study.
Disclosure Statement
The authors have no conflict of interest to disclose.