
Abstract
Abstract
Background:
Anastomotic leakage is a severe complication after gastric cancer surgery. Inadequate blood supply is regarded as an important risk factor. The aim of the study was to evaluate the feasibility and usefulness of intraoperative assessment of anastomotic vascular perfusion in gastric cancer surgery using near-infrared (NIR) camera imaging with indocyanine green (ICG)-enhanced fluorescence technique.
Materials and Methods:
From March 2015 to 2016, 30 patients undergoing laparoscopic gastrectomy for gastric cancer were prospectively evaluated. After completing the anastomosis, 2.5–5.0 mg of ICG was injected via peripheral veins. All anastomoses and resection margins were investigated using NIR camera to assess anastomotic perfusion. The assessment was performed using the adopted perfusion score of fluorescence activity, which ranged from 1 to 5 (1 = no uptake, and 5 = iso-fluorescent to all other segments).
Results:
Twenty-six distal gastrectomy (20 gastroduodenostomies, 6 gastrojejunostomies), 3 total gastrectomies (TG), and 1 pylorus-preserving gastrectomy were performed. The gap of visualization was 4.1 ± 3.2 minutes (range, 2–15) after ICG injection. Twenty-three of 30 patients (76.7%) showed technically successful ICG visualization. Among gastroduodenostomies, the average scores for gastric and duodenal sides were 3.5 and 3.7. Among gastrojejunostomies, the average scores for gastric, jejunal, and duodenal stump sides were 3.5, 4.0, and 3.8 (jejunojejunostomy, 3.5). Among TG, the average scores for esophagojejunostomy, duodenal stump, and jejunojejunostomy were 3.7, 4.0, 4.0, and 4.7. One case of leakage occurred in this study. Other complications included fluid collection and stenosis in 1 patient each.
Conclusions:
This study showed intraoperative ICG angiography using NIR camera is feasible and provides imaging of anastomotic blood flow. Further studies are needed for practice.
Introduction
The effort to minimize postoperative complications is the fate of surgeons. In particular, the surgical technique for gastric cancer has been improved to introduce the minimally invasive surgery, but complications cannot be completely prevented.
Anastomotic leakage in gastric cancer surgery is a major complication associated with poor immediate clinical consequences, increased mortality, and poor long-term outcomes.1–3 The reported rate of leakage in gastric cancer surgery varies from 1.2% to 6.7%.4–8 There is an alternative method of ileostomy or colostomy for patients with leakage of the colorectal anastomosis. However, no such alternative is available for leakage after upper gastrointestinal surgery. Such patients may experience great difficulty in oral ingestion, and malnutrition caused by long-term parenteral nutrition can be fatal to death.
The essential elements of robust bowel anastomosis include proper perfusion, a tension-free state, accurate tissue apposition, and minimal spillage of bowel contents. 9 Most surgeons strive to keep these principles to reduce leakage. In particular, an inadequate blood supply is regarded as one of the most important risk factors for leakage, and surgeons attempt to measure perfusion by empirical methods such as pulse palpation, active bleeding at the cut edges, no tissue discoloration, and mobility of the intestines. In addition to these subjective evaluation methods, objective methods such as Doppler and fluorescein injection have been used. However, Doppler may not produce accurate results because of pulsation from neighboring large vessels, and fluorescein shows large deviations among studies, which is a limit to obtaining consistent results.10–12
Recently, a new technique involving indocyanine green (ICG)-enhanced fluorescence has been introduced to obtain detailed anatomical information during laparoscopic surgery.13,14 ICG is a dye with the ability to emit fluorescent light when exposed to near-infrared (NIR) rays (∼820 nm). This light cannot be detected visually; thus, the surgical anatomy can be visualized in real-time using an NIR-detecting camera.15,16
Therefore, we focused on the ability to identify the blood flow in the intestine using the fluorescent capability of the NIR wavelength of ICG to evaluate the degree of ICG expression to confirm the blood flow at the anastomotic site. The aim of this study was to evaluate the feasibility and usefulness of intraoperative assessment of anastomotic vascular perfusion in laparoscopic gastric cancer surgery using the NIR camera with an ICG-enhanced fluorescence technique.
Patients and Methods
Patients
This was a prospective exploratory study of laparoscopic gastrectomies. Thirty ICG-enhanced fluorescence-guided procedures were performed at Seoul National University Hospital using the laparoscopic system with an NIR function from March 2015 to 2016. All patients underwent elective surgery by three experienced gastric surgeons. The inclusion criteria were patients scheduled for laparoscopic gastrectomy as the primary treatment for gastric cancer with agreeing to the informed consent. We excluded patients with known iodide hypersensitivity. Institutional Review Board approval was obtained (IRB No. 1412-152-638).
Patient demographics were collected, which included age, sex, body mass index (BMI), underlying diseases, pathologic stage, and type of operation. All postoperative complications were recorded and graded according to the Clavien–Dindo classification. Any finding regarded as an adverse event relevant to ICG injection was recorded. Intraoperative factors, including the operative time and amount of blood loss, were also collected.
Indocyanine green
ICG is a sterile, water-soluble, and tricarbocyanine molecule with a molar mass of 774.96 g/mol. Clinical use of ICG began after obtaining U.S. Food and Drug Administration approval in 1959. 17 Following intravenous injection, ICG becomes rapidly bound to plasma proteins and confined to the vascular system. Nearly all excretion takes place in the liver through the bile within 3–8 minutes after injection without any metabolites.17,18 The standard clinical dose is 0.1–0.5 mg/mL/kg, much lower than the maximum daily dose of 2.0 mg/kg. 17 ICG becomes fluorescent by NIR light at wavelengths of about ≥820 nm. ICG absorbs light of 750–810 nm, emits NIR light of 830 nm, and requires specially designed scopes and a camera system for detection. 19
NIR camera system
In this study, a laparoscopic NIR camera system (Karl Storz Endoskope spies TM GmbH & Co. KG, Tuttlingen, Germany) was used. Image generation was performed by the high-end full-definition camera system connected to a laparoscope equipped with a specific filter for detection of NIR fluorescence and white light. 20 The xenon light source (D-LIGHT; Karl Storz) provides both NIR excitation light and visible light. The surgeons can easily switch from standard light to the NIR mode by pressing a pedal.
ICG injection and evaluation of perfusion grade
ICG was intravenously injected at a concentration of 2.5 mg/mL immediately after anastomosis. Bowel perfusion was clinically assessed and then measured using the NIR camera system. After assessment of gross findings, we changed the camera system to the NIR mode and recorded the time to initial expression of ICG. The fluorescence score was recorded at all anastomotic points. The perfusion grade was evaluated by the operating surgeon and video-recorded. For evaluation of the perfusion grade, we used the same scoring system reported by Sherwinter et al. 21 A fluorescence score of 1–5 (1 indicating no uptake and 5 indicating maximal uptake) for each anastomosis was assigned to each patient. A clinical score of 1–5 (1 indicating a dusky appearance and 5 indicating pinkish pulsatility of the mesenteric vessels and active bleeding from the cut edge) was also assigned (Table 1).
Perfusion Score Determined by Clinical and Fluorescence Assessmenta
Sherwinter et al. 21
Results
Demographics and clinical outcomes
During the study period, assessment of bowel perfusion was performed in 30 patients (mean age, 58.7 ± 11.0 years; 18 males and 12 females) who underwent distal gastrectomy (DG) with gastroduodenostomy (n = 20), gastrojejunostomy (n = 6), total gastrectomy (TG) (n = 3), and pylorus-preserving gastrectomy (PPG) (n = 1).
The average BMI of patients was 23.8 ± 3.6 kg/m2, and 56.7% of patients had comorbidities such as hypertension and/or diabetes. Most patients were diagnosed with early gastric cancer (93.3%) because this study included patients who were scheduled to undergo laparoscopic gastrectomy. No intraoperative adverse events or conversion to open surgery occurred. The mean postoperative hospital stay was 10.5 ± 16.2 days. The complication rate was 10% (3/30) and included fluid collection (n = 1), anastomotic stenosis (n = 1), and anastomotic leakage (n = 1) after gastroduodenostomy (Table 2).
Patient Demographics and Clinical Outcomes
All three complications were detected in patients who underwent gastroduodenostomy.
BMI, body mass index; DG, distal gastrectomy; SD, standard deviation.
Results related to ICG injection
After completion of the anastomosis, a bolus of 2.5–5.0 mg of ICG (concentration of 2.5 mg/mL and volume of 1 or 2 mL) was administered intravenously. The injection amount according to the operation type is summarized in Table 3. No ICG-related side effects occurred, such as hypersensitivity reaction. The mean time to the initial detect of ICG-enhanced fluorescence was 4.1 ± 3.2 (range, 2–15) minutes after injection. The mean time to initial detection according to the operation type was 4.5 (range, 2–15) minutes in gastroduodenostomy, 4.2 (range, 2–5) minutes in gastrojejunostomy, 3.0 (range, 2–4) minutes in TG, and 4.0 minutes in PPG.
Results Related to Indocyanine Green Injection
BI, Billroth I anastomosis; BII, Billroth II anastomosis; DG, distal gastrectomy; ICG, indocyanine green; PPG, pylorus-preserving gastrectomy; SD, standard deviation; TG, total gastrectomy with Roux-en-Y esophagojejunostomy.
ICG-enhanced fluorescence was detected in 100% of patients. However, when failure of ICG enhancement was defined as a perfusion score of <2 points for more than two sites for convenience, the success rate was 76.7% (23 of 30 patients). According to the operation type, successful expression of ICG was observed in 15/20 (75.0%) patients who underwent gastroduodenostomy, 4/6 (66.7%) who underwent gastrojejunostomy, 3/3 (100.0%) who underwent TG, and 1/1 (100.0%) who underwent PPG. The initial detection time and success rate were not statistically different when analyzed according to the operation type, BMI, age, sex, or presence of underlying disease.
Evaluation of perfusion according to clinical and fluorescence scores
All anastomoses were assessed for perfusion by gross visualization under white light mode and ICG uptake using NIR mode. Both clinical and fluorescence perfusion was well maintained in the healthy anastomosis site as shown in Figure 1.
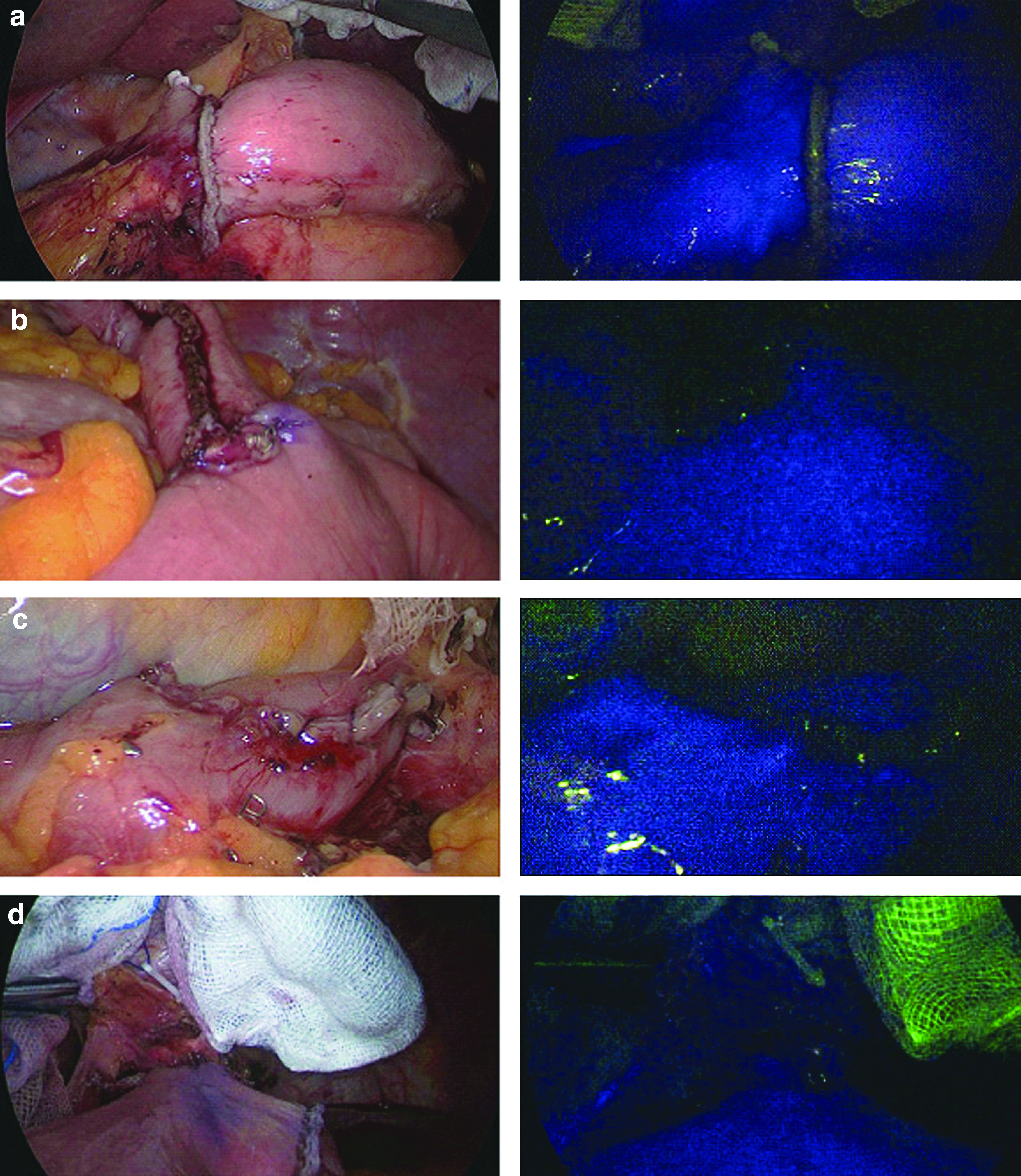
Photographs of healthy anastomosis sites with good perfusion as confirmed by a near-infrared camera. White-light view (left) and NIR mode (right).
The clinical and fluorescence scores of the cases except failure cases were summarized in Figure 2. In patients who underwent gastroduodenostomy, the mean clinical/fluorescence scores were 5.0 (range, 5)/3.5 (range, 3–5) on the stomach side of the gastroduodenostomy, 4.7 (range, 2–5)/3.7 (range, 2–5) on the duodenal side, and 5.0 (range, 5)/3.1 (range, 1–5) on the lesser curvature side, respectively. In patients who underwent gastrojejunostomy, all clinical scores were 5.0 points at each site, while the fluorescence scores ranged from 3.5 to 4.0. In patients who underwent TG and PPG, the clinical scores were as high as 5.0, but the fluorescence scores were relatively lower than the clinical scores.
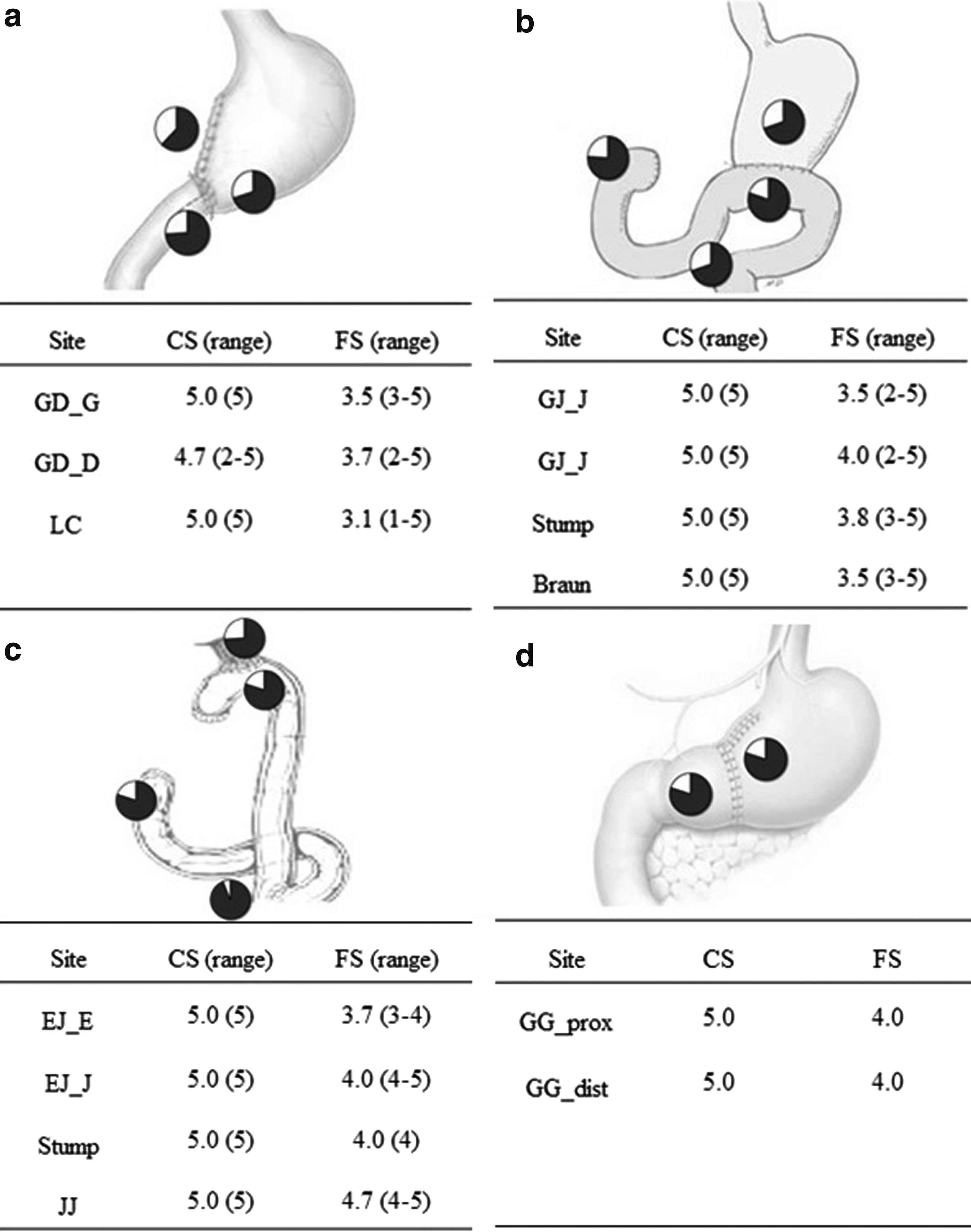
Assessment of perfusion grade, excluding cases of failure.
No change in the surgical plan occurred in this study because the clinical score was high (i.e., a pinkish color and pulsatility were observed, and no signs of ischemia were present, despite the fact that the fluorescence score was low). However, 1 patient experienced anastomotic leakage after gastroduodenostomy. His clinical perfusion scores were 4 on the duodenal side and 5 on the stomach side, and his fluorescence perfusion scores were 4 on the duodenal side and 3 on the stomach side. A review of the surgical video after development of the leakage revealed a focal perfusion defect only in the NIR mode around the gastroduodenostomy (Fig. 3). In addition, one stenosis also developed after gastroduodenostomy, and his clinical scores were both 5 on the duodenum and stomach side, however, his fluorescence scores were 5 and 3, respectively. Results related ICG injection and perfusion score of all patients are described in Supplementary table 1 and Supplementary figure 1.
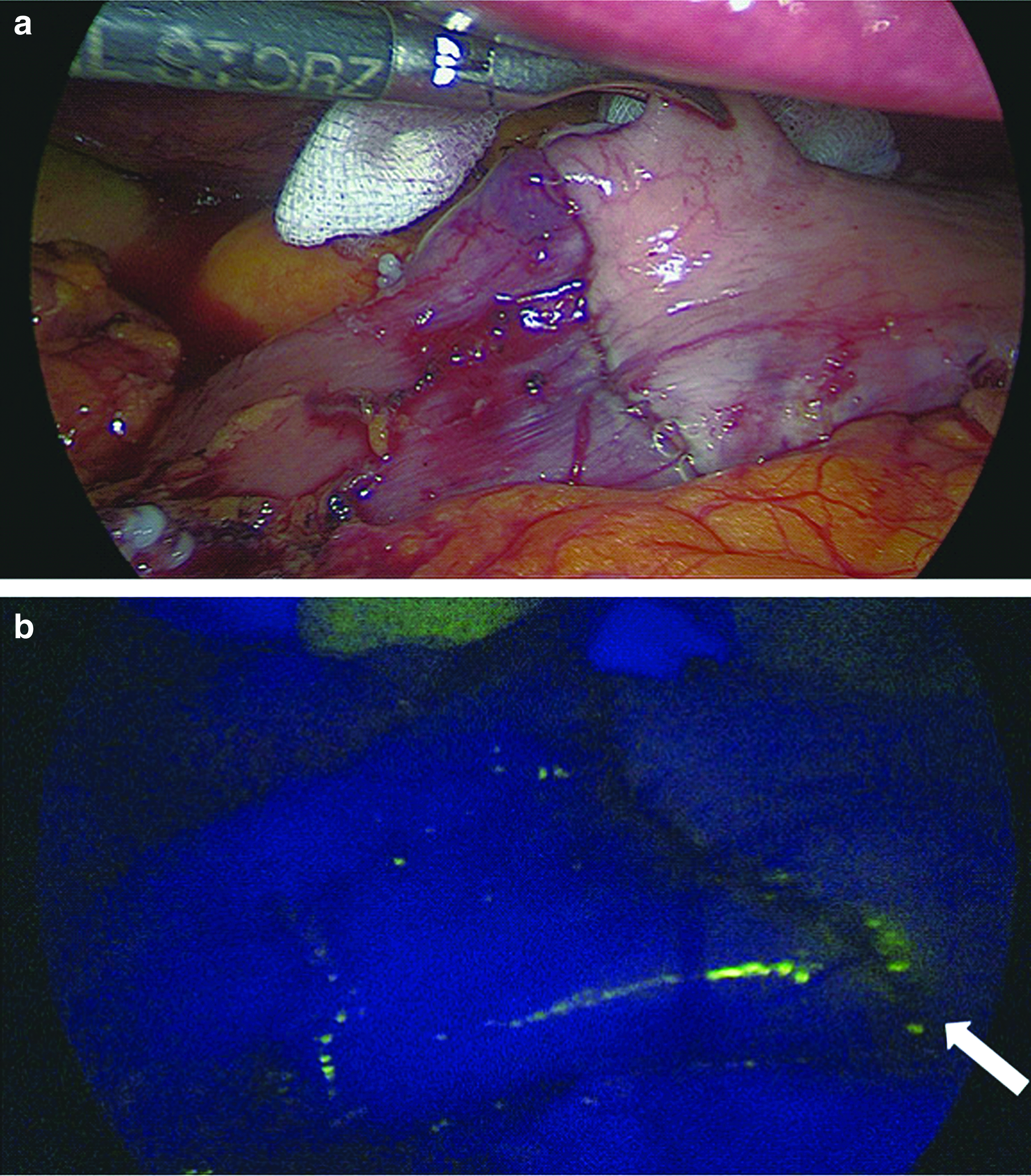
Photographs of the leakage after DG with gastroduodenostomy anastomosis.
Discussion
Assessment of perfusion at the anastomotic site cannot be reliably performed for several reasons. First, variations exist in patient factors such as the vascular anatomy and the presence of artherosclerotic vascular disease. 22 Second, surgical factors are included, such as excessive bowel manipulation, severe anastomotic tension, and aggressive dissection. Visual inspection is less predictable for confirmation of adequate blood flow to the anastomotic site. 23 Therefore, a reliable method for real-time accurate and consistent evaluation of anastomotic perfusion during surgery is needed. NIR fluorescence angiography has been used to assess tissue perfusion in several types of surgery such as colectomy, plastic reconstruction, and cardiac surgery.21,24,25
We thus hypothesized that an ICG-enhanced fluorescence technique using an NIR camera system would be effective in evaluating anastomotic perfusion after gastrectomy and ultimately help to reduce complications such as leakage.
This study has demonstrated the potential role of an ICG-enhanced fluorescence technique using an NIR camera system as an assessment tool for anastomotic vascular perfusion in laparoscopic gastric cancer surgery. This study is the first to show the clinical feasibility and usefulness of an ICG-enhanced fluorescence technique using an NIR camera system to determine the perfusion status at the anastomotic site during laparoscopic gastric cancer surgery.
In this study, we observed the expression of ICG fluorescence in all patients. However, the perfusion status of 5 patients who underwent gastroduodenostomy and 2 patients who underwent gastrojejunostomy was not clearly observed. There was no significant difference in age, body weight, BMI, underlying disease, sex, or injected dose between patients in whom the perfusion status was and was not successfully observed. In terms of the dose per body weight (mg/kg), we observed a tendency of a lower injection volume among patients in whom the perfusion status was not observed (0.037 mg/kg) than those in whom the perfusion status was observed (0.049 mg/kg) (P = .07). In future studies, it may be helpful to match the dose per body weight to obtain more accurate results regarding the perfusion status.
There was an anastomotic leakage in this study. The patient was a 78-year-old man with no underlying disease and a BMI of 23.1 kg/m2. DG with gastroduodenostomy was performed; the operation time was 260 minutes, the estimated blood loss was 50 mL, and no notable intraoperative events occurred. The clinical appearance of the stomach side of the gastroduodenostomy was healthy, and that of the duodenal side showed a relatively unhealthy appearance that was clinically concerning with respect to tissue viability. However, blood vessels were present around the anastomosis, and assessment via ICG fluorescence and the NIR camera showed that although the degree of expression was not high, even uptake was evident; therefore, no additional management such as reinforcement was performed. When we reviewed the operation video, we confirmed that focal uptake was reduced on the inferior side of the gastroduodenostomy. Leakage had occurred at this site, and the patient was discharged after a reoperation of gastrojejunostomy.
Notably, although overall perfusion is important, the anastomosis site itself requires careful observation and evaluation to determine whether focal uptake reduction has occurred. The hypothesis of this study was that the fluorescence assessment method after ICG injection can be an objective test to reduce the anastomotic leakage caused by poor blood supply by more accurate diagnosis of ischemia of poor perfusion with enhanced visual information. Based on our hypothesis, if blood flow is insufficient on the anastomotic site, the fluorescence assessment score will be low, and this may be the one of the objective tests that accurately diagnoses the possibility of ischemia-induced leakage among various causes of the anastomotic leakage.
The feasibility of this method was confirmed in this study, and if the effectiveness of this method is proved through further future studies, the following clinical application will be possible. If the fluorescence assessment shows good perfusion, the anastomosis can be regarded as healthy in terms of blood supply; however, the anastomotic site should be closely observed for focal changes. Conversely, if fluorescence assessment reveals poor perfusion, the clinician cannot conclude that all anastomoses are unhealthy. Instead, it may be necessary to observe the anastomotic site again and take additional precautionary measures.
Several methods have been used to assess the intraoperative perfusion status, including Doppler, laser Doppler flowmetry, fluorescein injection, and oxygen spectroscopy. 12 These techniques have not been widely accepted because they are not readily applicable in practice or their reliability has not been proved.
ICG-enhanced angiography is a more recently developed method that has been applied to patients undergoing colorectal resection. Boni et al. 26 reported that this method could provide more accurate information about the perfusion status of the bowel before bowel transection, after division of the mesentery, and before completion of the anastomosis. The authors predicted that this method could reduce the incidence of postoperative anastomotic leakage by helping to determine the surgical plan, including the extent of resection. Indeed, in a multicenter prospective study of 147 patients undergoing colorectal surgery, 11 patients (7.9%) changed their surgical plan based on abnormal ICG angiography results. The anastomotic leakage rate of that study (1.4%, 2 patients) was lower than the known leakage rate 27 because none of the 11 patients with a poor blood supply developed anastomotic leakage after anastomotic revision. 28
The herein-described ICG-enhanced angiography method using an NIR camera has several advantages: high tissue permeability, auto-fluorescence, and real-time imaging. This method can obtain more stable results because it differs from Doppler in that it is not disturbed by the interpretation of the results due to surrounding tissues or organs and is not influenced by the patients' individual factors such as underlying disease or body weight. In addition, as tactile sense cannot be used in laparoscopic surgery, the herein-described method using visual information has an advantage for laparoscopic surgery.
However, no consensus has been reached regarding the optimal dose for perfusion assessment to obtain a more clearly visualized image in laparoscopic gastrectomy.20,26,29 The authors performed this study according to previously reported doses 21 and obtained visualization in 100% of the patients. At 23.3%, however, no satisfactory images were obtained. If the dose is determined with a more accurate criterion of how much milligram is injected per kilogram, based on results with higher injection doses among previously published articles, a more consistent result can be obtained, leading to more effective assessment of the perfusion status. Another disadvantage is the lack of an accurate measurement tool with which to objectively quantify the signal intensity. As shown in Table 1, an objective tool introduced in other articles was used in the present study, but the final evaluation of the image was performed by the surgeon. To overcome this drawback, several surgeons participated in the evaluation to obtain the most objective results as many as possible.
The primary end points were the feasibility and usefulness of the ICG-enhanced fluorescence technique using the NIR camera during laparoscopic gastric cancer surgery. Although the perfusion status was successfully confirmed in only 76.7% of patients, fluorescence was detected in all patients, and the 1 patient with leakage showed reduced focal intensity. The feasibility and usefulness of this method were acceptable. In future studies, the effectiveness of this method should be evaluated by further validation and determination of the most appropriate dose. It will also be necessary to develop an objective analytic tool or share the objective imaging data according to the perfusion score. Through these efforts for improvement of this method, we believe that it is conceivable to perform reanastomosis or add reinforcement sutures when the perfusion score is less than a specific point. This method is not a royal road, but it provides additional information that can at least reduce the leakage rate.
In conclusion, the current study confirms that assessing intraoperative bowel perfusion with NIR camera imaging using an ICG-enhanced fluorescence technique during laparoscopic gastric cancer surgery is feasible and potentially useful. Although no definitive answers can be obtained regarding the optimal dose and predictive score for identifying defects in tissue perfusion that may lead to anastomotic leakage, the results of this study are encouraging and warrant further investigation.
Footnotes
Acknowledgment
This study was supported by the Seoul National University Hospital Research Fund (grant No. 04-2016-3090) and partly supported by Karl Storz, Inc. (grant No. 062014318).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.