
Abstract
Abstract
Background:
The purpose of this study was to examine ventilation patterns, including tidal volume (TV) and positive end-expiratory pressure (PEEP) selection in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy.
Methods:
Intraoperative ventilation data, including TV and PEEP, were abstracted from the electronic anesthesia record (Metavision) at Brigham and Women's Hospital. Ideal body weight (IBW) was calculated using the Devine formula, and TV per kg IBW was calculated for each patient.
Results:
The mean TV delivered per kg IBW was 7.35 ± 1.07 mL/kg, and 24% (281/1186) of patients received TVs of >8 mL/kg IBW. The median PEEP applied was 5.5 ± 0.6 cmH2O, and 87% (1035/1186) of patients received PEEP >0 cmH2O. There was significant variation in both TV and PEEP selection.
Conclusions:
The significant variation in TV per kg IBW as well as in PEEP values at our institution may reflect the lack of well-established guidelines for intraoperative ventilation. Many patients in this study received inappropriately large TVs (>8 mL/kg IBW), which may be due to calculation of TVs based on total body weight rather than IBW. Patients of shorter stature and higher body mass index appear to be at higher risk for ventilation with inappropriately large TVs.
Introduction
The evergrowing population of obese patients undergoing general anesthesia requires that providers understand the unique challenges associated with the anesthetic care of this population, especially pertaining to intraoperative ventilation. It is well known that obese patients have reduced lung volumes, are prone to developing significant atelectasis, have increased airway resistance, and have reduced respiratory compliance. Furthermore, associated comorbidities such as obstructive sleep apnea and pulmonary disease increase the risk of perioperative complications such as postoperative hypoxemia.1–5 Ventilation for laparoscopic bariatric surgery presents challenges beyond those for other surgical procedures in obese patients. Laparoscopic bariatric surgery involves insufflation of gas into the abdominal cavity (pneumoperitoneum), which increases pressure on the diaphragm. The resulting upward shift leads to decreased lung volumes, which can result in reduced oxygenation capacity and favor atelectasis. In addition, airway pressures rise due to decreases in lung and chest wall compliance.6,7 Commonly employed methods to address these physiological challenges include the application of positive end-expiratory pressure (PEEP) to prevent airway collapse and atelectasis, use of reverse-Trendelenburg position to reduce upward pressure on the diaphragm, as well as the periodic employment of recruitment maneuvers. 8 Careful selection of ventilation mode and tidal volumes (TVs) is also central to effective management of these patients to reduce lung injury.
Lung-protective ventilation is a well-known ventilation strategy in the intensive care setting to manage patients with existing lung injury. 2 This method of ventilation uses lower mean TVs (<8 mL/kg) and low plateau pressures (<30 cmH2O), and applies PEEP (of 5 cmH2O or more). 2 Avoiding large TVs in this way may prevent alveolar overdistension, atelectotrauma, oxygen toxicity, localized inflammation, and release of cytokines.1,3 Application of lung protective ventilation in the operating room setting has shown mixed results. One study found that lung protective practice helped decrease postoperative pulmonary complications (PPCs) and length of hospital stay in healthy, nonobese patients undergoing abdominal surgery. 3 However, another study in obese (body mass index [BMI] >35) patients undergoing gynecological laparoscopic surgery showed that a lung-protective strategy did not lead to significant differences in postoperative oxygenation and respiratory function. 9 A separate study found that the use of periodic recruitment maneuvers and PEEP of 10 cmH2O led to reduced lung atelectasis, shorter post-anesthesia care unit (PACU) stay, improved oxygenation intraoperatively and postoperatively, and fewer pulmonary complications in the bariatric population. 10
While lung protective ventilation practices such as those described have become more commonplace in the operating room (OR) setting, 2 it is unclear if these practices are being applied uniformly across different patient populations, including in obese patients undergoing laparoscopic procedures. As has been documented previously, obese patients are often ventilated with large TVs despite there being no evidence of improved oxygenation and some evidence of pulmonary complications.6,11,12 Patients of shorter stature and female gender may be especially at risk. 11 It has been hypothesized that larger TVs observed in actual clinical practice for obese patients may be the result of TV calculations based on total body weight (TBW) rather than ideal body weight (IBW). 11 Fernandez-Bustamante et al. conducted a review of current intraoperative ventilation practices in 2015 for obese patients and recommended the use of protective ventilation with low TVs based on IBW (6–8 mL/kg IBW), with application of PEEP and recruitment maneuvers. 13 However, the benefits of this method and its adoption rates remain poorly characterized. Given the lack of clear guidelines and observed variation in ventilation practices, there remains the need for further investigation to define current practice trends.
In this observational, retrospective analysis, we aimed to describe current patterns in intraoperative ventilation practices for morbidly obese patients undergoing laparoscopic bariatric surgery. We hypothesize that there is significant variability in TV and PEEP ventilation practices, which may be especially pronounced at extremes of BMI and height. This variation may be due to calculation of TVs based on TBW or other weight calculation rather than IBW.
Methods
Study data were gathered from the electronic anesthesia record (Metavision, Wakefield, MA) at one institution (Brigham and Women's Hospital, Boston, MA) from January 1, 2010, to May 29, 2015. The study period was defined by the timeframe of utilization of this electronic anesthesia record system. Institutional Review Board approval was obtained for analysis of data and was exempted from the consent requirement due to the de-identified nature of the data. For every surgical case abstracted from the electronic system, data were obtained regarding the patient's age, sex, American Society of Anesthesiologists classification, height, weight, surgical service, and surgical procedure. IBW was calculated using the Devine formula. 14 Ventilator data, including TV and PEEP settings, were abstracted from the electronic anesthesia record at 5-minute intervals. Figure graphics were created using R version 3.2.3.
Intraoperative management considerations
Patients at Brigham and Women's Hospital undergoing bariatric surgery are treated according to an intraoperative protocol developed for this patient population and designed to address risks regarding intraoperative anesthesia, postoperative analgesia, and postoperative respiratory depression (Appendix 1). However, the protocol does not specify ventilator strategies, focusing predominately on medication management. The use of a standard anesthetic protocol increases standardization in patient management, and may minimize the impact of unrecorded variables on study results.
Inclusion and exclusion criteria
To provide the most specific focus on bariatric surgery, the study group was limited to Roux-en-Y gastric bypass operations and sleeve gastrectomies by our bariatric surgery group. Cases were identified by the presence of the laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy in the mapped text values based on the ICD-9-CM codes recorded in the electronic anesthesia record, thereby excluding all cases in which conversion to an open operation occurred. After inclusion and exclusion criteria, a total of 1186 cases were included in the analysis.
Results
Demographics
Demographic information is shown in Table 1. A total of 1186 cases were identified with a mean patient age of 43.4 ± 12.2 years and mean BMI of 45.0 ± 11.9 kg/m2. Of those patients, 60.2% underwent laparoscopic sleeve gastrectomy and 39.8% underwent a laparoscopic Roux-en-Y gastric bypass with a mean anesthesia control time of 109.2 ± 46.5 minutes.
Patient Demographics and Surgical Procedure Performed
ASA PS, American Society of Anesthesiologists Physical Status; SD, standard deviation.
Tidal volumes
As shown in Table 2, the mean TV delivered for all patients was 588.63 ± 60.92 mL. TVs per kg IBW were calculated to assess ventilatory settings based on total and IBWs using height data from the intraoperative anesthesia record. These calculations yielded a mean TV of 7.35 ± 1.07 mL/kg IBW, and a mean of 4.98 ± 1.00 mL/kg TBW. The distribution of TVs per IBW and TBW is shown in Figure 1 (center and right, respectively). TV ranges were defined as <6 mL/kg IBW, between 6 and 8 mL/kg IBW, and >8 mL/kg IBW. The percentage of all TVs that fell into each range was calculated: 9% (106/1186) of patients received TVs of <6 mL/kg IBW, 67% (796/1186) received between 6 and 8 mL/kg IBW, and 24% received (281/1186) >8 mL/kg IBW. Subgroup analysis by gender is shown in Table 3. The mean TV for men was 6.84 ± 0.92 mL/kg IBW and 4.67 ± 0.85 mL/kg TBW. The mean TV for women was 7.48 ± 1.07 mL/kg IBW and 5.06 ± 1.01 mL/kg TBW. Figures 2 and 3 show scatter plots with data grouped into hexagonal bins based on the frequency of results. In Figure 2 (TV per kg IBW versus BMI), the highest frequency bins are concentrated between BMI values of 30 and 60 kg/m2, and TVs between 6 and 8 mL/kg IBW. The TVs in the 10 mL/kg IBW or greater range correspond to patients with BMIs mostly >40 kg/m2. In Figure 3 (TV per kg IBW versus height), most patients between 150 and 170 cm in height received TVs between 6 and 8 mL/kg IBW, while for patients <150 cm, there was an increased frequency of TV >8 mL/kg IBW.

Frequency distribution of tidal volumes selected by anesthesia provider. At left, median total tidal volumes (mL). Center, mean tidal volumes (mL) per kg of IBW. Right, mean tidal volumes (mL) per kg total body weight. IBW, ideal body weight.

Body mass index (kg/m2) versus tidal volumes (mL) per kg IBW.
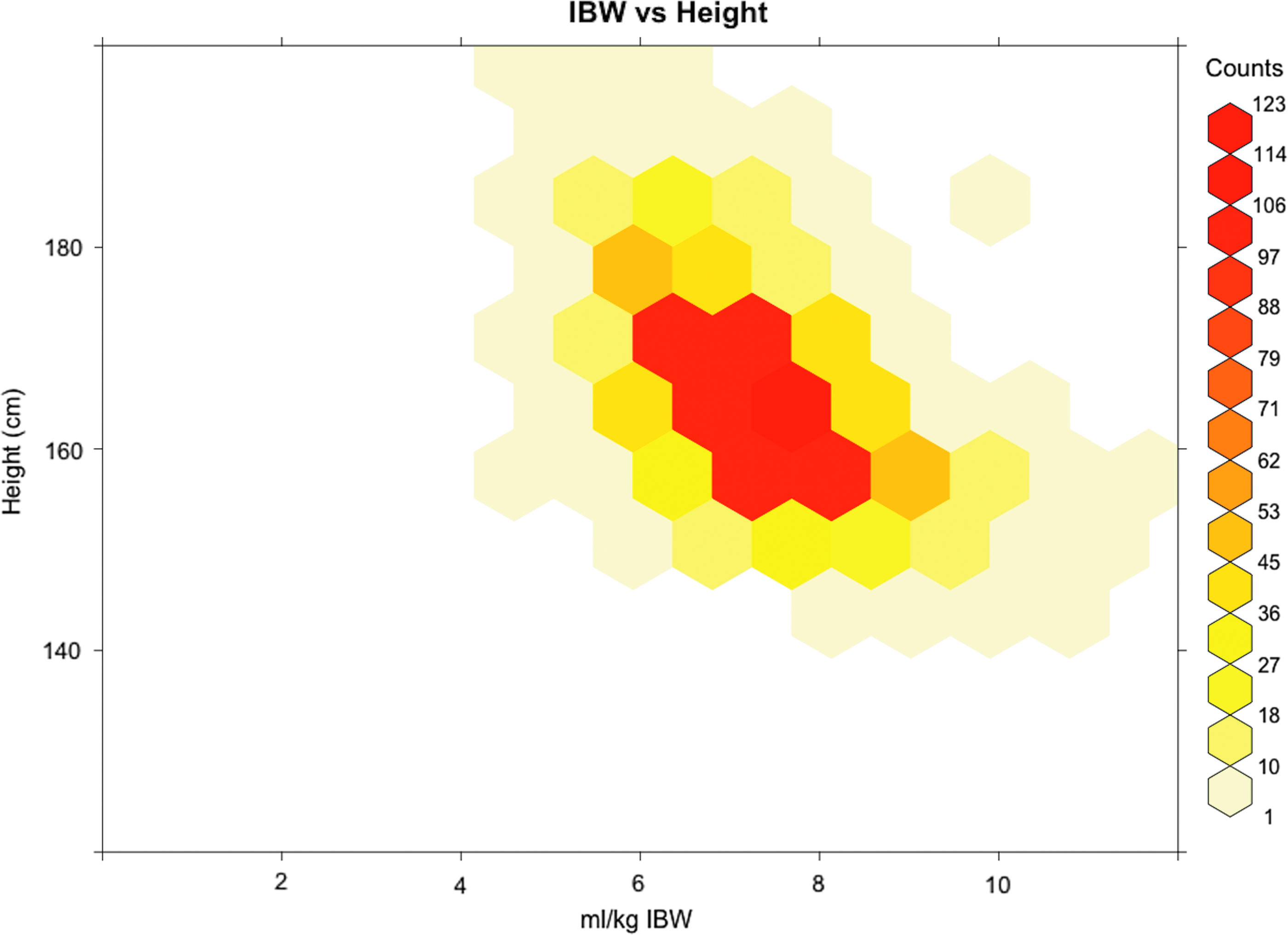
Height (cm) versus tidal volumes (mL) per kg IBW.
Mean Tidal Volumes (Overall and Per Kilogram Ideal Body Weight and Total Body Weight), Positive End-Expiratory Pressure, Peak Airway Pressure, and Endotracheal Tube Size
TV, tidal volume; IBW, ideal body weight; TBW, total body weight; SD, standard deviation; IQR, interquartile range, PEEP, positive end-expiratory pressure; ETT, endotracheal tube.
Subgroup Analysis by Gender of Tidal Volume per Kilogram Ideal Body Weight and Total Body Weight
SD, standard deviation.
Positive end-expiratory pressure
The median PEEP was 5.5 ± 0.6 cmH2O. Figure 4 shows the distribution of PEEP values ranging from 0 to 15 cmH2O, with data points falling between 3 and 10 cmH2O. Eighty-seven percent (1035/1186) of patients received PEEP >0, while 4% (48/1186) received 0 PEEP. One hundred three (8.7%) received an unknown amount of PEEP. Sixty-six percent (778/1186) of patients received both TV <8 mL/kg and at least some amount of PEEP.
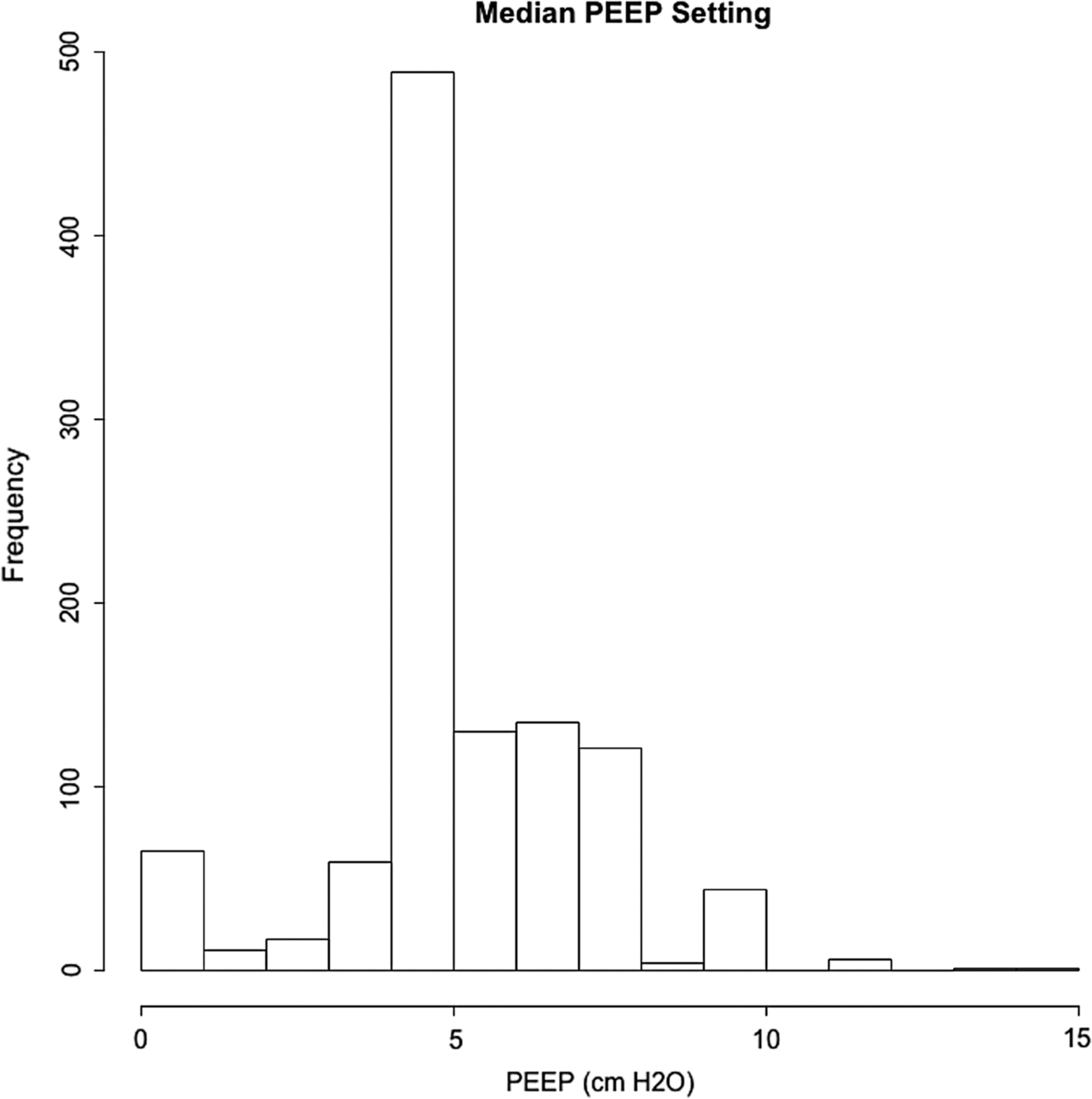
Frequency of positive end-expiratory pressure values in cmH2O.
Other results
The mean peak airway pressure was 30 ± 3 cmH2O. The average endotracheal tube inner diameter was 7 mm (interquartile range: 7–7.5 mm).
Discussion
The results of our study demonstrate that at our institution, there remains significant variation in TV and PEEP selection. A significant percentage (24%) of bariatric patients undergoing either laparoscopic Roux-en-Y bypass or laparoscopic sleeve gastrectomy were ventilated with large TVs (>8 mL/kg IBW), with some patients receiving above 10 mL/kg IBW. There also continues to be a variation in PEEP selection, possibly due to recently published outcomes data with conflicting results.3,15 In addition, our results suggest that those patients with shorter stature, both extremes of BMI, and female gender may continue to be at risk for ventilation with TVs >8 mL/kg.
To place the results of this study in context requires a discussion of current best practices for ventilation in the OR setting. As documented by Wanderer et al., protective lung ventilation strategies have become increasingly common over time in the intraoperative setting, even though there are no well-established guidelines based on intraoperative data to guide this practice. 16 There have been various recommendations made in recent years related to intraoperative TVs. Schultz et al. recommended in their 2007 review to use TVs ≤10 mL/kg IBW for patients with normal lungs and ≤6 mL/kg for patients with abnormal lungs or those at risk for acute lung injury. 17 Despite these recommendations, Fernandez-Bustamante et al. found in their 2011 study that 17.5% of patients received TVs >10 mL/kg IBW, 11 demonstrating that ventilation with inappropriately large TVs remained common. Other more recent studies have defined a TV range of 6–8 mL/kg IBW as “protective” in the operative setting.3,16,18 In Wanderer et al., it was found that 14.9% of all cases received TVs of >10 mL/kg IBW, suggesting that inappropriately large TVs continue to be selected despite attempts to define protective intraoperative TV ranges. 16
Ventilation during laparoscopic surgery in the bariatric patient population presents additional challenges due to the surgical need for pneumoperitoneum. Increased intraabdominal pressure due to insufflation of the abdomen increases the airway pressures necessary to generate the desired TVs. In practice, ventilating these patients often requires frequent adjustment of ventilatory parameters (i.e., switching to a pressure-controlled volume guaranteed mode) to achieve the desired TVs. In addition, ventilation under these circumstances, while maintaining airway pressure in the lung-protective range (<30 cmH2O), can result in minute volumes lower than necessary to maintain physiologic end-tidal CO2 values. Many providers will allow the resultant hypercapnia to persist in this setting as long as oxygenation remains acceptable (permissive hypercapnia). The ventilation challenges posed by pneumoperitoneum on top of the preexisting altered pulmonary mechanics of the bariatric patient population make this an especially interesting cohort to study regarding current ventilation practices.
As seen in the IBW graph (Fig. 1, center), there remains significant variation in how our anesthesia providers are ventilating the bariatric patient population. In addition, as noted above, roughly ¼ of the patients in this study received large TVs (>8 mL/kg IBW). Aside from the lack of clear guidelines, one explanation for this variation is that TVs are being calculated erroneously based on TBW rather than IBW. In high BMI patients like the population under study, this practice will invariably lead to inappropriately large TVs relative to IBW. This trend can be observed in Figure 2, which plots BMI against TV per kg IBW; most of the patients receiving >10 mL/kg IBW have a BMI of >40 kg/m2. It is also possible that providers are following the outdated practice of purposely selecting larger TVs (>8 mL/kg IBW), believing that this prevents hypoxemia and/or atelectasis in the setting of abdominal surgery. As discussed previously, studies have shown that TVs such as those in the 10–15 mL/kg IBW range have no benefit in terms of postoperative oxygenation status or complications, and have been associated with increased levels of serum inflammatory markers postoperatively.1,3,19 In either case, TVs >8 mL/kg IBW represent inappropriately large TVs relative to IBW, and are inconsistent with any definition of intraoperative lung protective ventilation suggested in the literature thus far.
In addition to increased BMI, prior studies have shown poor compliance with lung protective practices in patients of shorter stature and female gender.11,16,20 Height has long been accepted as one of the most accurate physiologic proxies for lung volume. However, as can be seen in Figure 3, there is a negative correlation between height and TV per kg IBW; as the height decreases, the TV per mL/kg IBW increases. Since height is an essential part of the IBW formula, these results again suggest that providers may not be appropriately using IBW to calculate TVs. By ignoring IBW in these patients of shorter stature and higher BMI, providers may be unintentionally and disproportionally overestimating TVs in this population. We also examined patient gender with respect to TV selection. Women received a mean TV of 7.48 ± 1.07 mL/kg IBW, whereas the mean TV for men was 6.84 ± 0.92 mL/kg IBW. This difference could again be explained by providers using TBW instead of IBW to calculate TVs. As discussed above, there appears to be a negative correlation between height and TV per kg IBW (as height decreases, TV per kg IBW seems to increase). Thus, it is possible that women are being disproportionally affected by ignoring IBW since they are on average shorter than men. In addition, it could be that providers are overestimating IBW for women. It is known that on average, given a female and male of the same height, the female will have smaller lung volumes (thus the differing IBW formulas for men versus women). The larger mean TV per kg IBW for women compared to men is consistent with prior studies.11,16,20 These trends indicate the need for further study as well as the need for provider education with respect to calculating IBW, especially in patients of shorter stature, higher BMI, and female gender.
Finally, we examined intraoperative PEEP selection. As seen in Figure 4, the median PEEP of 5 cmH2O is by far the most frequently chosen PEEP value, likely because this is the default initial PEEP setting on ventilators at our institution. In our study, 87% of patients received at least some PEEP, similar to the 83.3% found by Wanderer et al. 16 In addition, 66% of patients in this study received both TV <8 mL/kg IBW and at least some amount of PEEP compared to 51% found by Wanderer et al. 16 Even though these results indicate that most patients are being ventilated with the application of PEEP and in accordance with lung protective practices, there is still a wide variation in PEEP selection, as can be seen in Figure 4, especially in the 5–10 cmH2O range. This could be partially explained by recent conflicting literature regarding optimal intraoperative PEEP settings outlined below.
In 2007, Schultz et al. advocated for PEEP of ≥5 cm H2O for all patients, 17 and the 2013 IMPROVE trial defined optimal PEEP as between 6 and 8 cmH2O. 3 There were also shown to be more PPCs in the low PEEP high TV group versus the lung protective group (Peep 0 and TV 10–12 mL/kg IBW versus Peep 6–8 and TV 6–8 mL/kg IBW, respectively), 3 although the PROVHILO trial showed no difference in complications between high and low PEEP (12 cmH2O versus ≤2 cmH2O, respectively). 15 In addition, in the PROVHILO trial, there were more interventions required for hypotension in the high PEEP cohort. 15 This lack of consensus may explain the variation in PEEP selection seen in this study, and suggests the need for further study to define these guidelines. It is important to note that the IMPROVE and PROVHILO trials do not specifically focus on the obese patient population, although the currently ongoing PROBESE trial will examine outcomes in obese patients ventilated with higher versus lower PEEP. 21
Limitations of our study include that we examined ventilation practices at only one academic medical center, and thus our findings may not be generalizable across all large academic facilities, or across community hospitals or ambulatory surgery centers. Our institution also has anesthesia resident trainees who are supervised by an attending anesthesiologist, making our results difficult to compare to institutions without an anesthesia residency program. As we only examined laparoscopic bariatric procedures, the results are not directly generalizable to all procedures performed in the obese population. This study also did not examine perioperative outcomes in relation to TV and PEEP settings. Last, we did not examine other aspects of ventilation such as FiO2, plateau pressure, and mean airway pressure, which constitute other important components of lung protective ventilation practice that could influence perioperative outcomes.
In conclusion, the intraoperative ventilation patterns in our study display continued significant noncompliance with lung protective practices in morbidly obese patients undergoing laparoscopic bariatric surgery, and show significant variation in TV and PEEP selection. In addition to patients with high BMI, patients of female gender and shorter stature appear to be especially at risk for ventilation with inappropriately large TVs. These findings highlight the need to further investigate the influence of patient factors on TV selection, as well as any relationship between TVs and adverse perioperative outcomes.
Footnotes
Disclosure Statement
E.Y.B., C.A.F., A.H.S., and E.E.W. have no conflict of interests. R.D.U. has received research funding for unrelated work from Merck, Mallinckrodt, and Medtronic and honorarium from 3M. The article is not under consideration for publication elsewhere and it has never been partially published.