
Abstract
Abstract
For over two decades, enhanced recovery pathways have been implemented in many surgical disciplines, most notably in colorectal surgery. Since 2001, the Enhanced Recovery After Surgery (ERAS®) Study Group has developed a main protocol comprising 24 evidence-based core items. While these core items unite similar preoperative, intraoperative, and postoperative principles across surgical subspecialties, variations and modifications exist to these core items based on unique considerations for each surgical subspecialty. This overview will summarize overarching principles for ERAS within hepatopancreaticobiliary (HPB) surgery, first summarizing Pancreaticoduodenectomy and Hepatectomy ERAS Society Guidelines. Specifically, principles and areas of current debate regarding preoperative oral carbohydrate loading/fasting, perioperative fluid management, and analgesia will be discussed. While institutions are beginning to realize both clinical and financial benefits of ERAS within HPB surgery, enhanced recovery remains a relatively recent phenomenon within the field. The complex patient population, high morbidity, and resource-intensive care involved in HPB surgery certainly warrant special consideration. To continue to promote improved clinical outcomes in a cost-effective manner, the ERAS Society will continue to actively address concerns and ensure all recommendations are based on the most up-to-date scientific evidence within the field of HPB surgery.
Introduction
For over two decades, enhanced recovery pathways have been implemented in many surgical disciplines, most notably in colorectal surgery.1,2 The Enhanced Recovery After Surgery (ERAS®) generic protocol was developed by a group of European academic surgeons in 2001 when they formed the ERAS Study Group. 3
The main protocol components comprised (1) an evidence-based approach to preoperative, intraoperative, and postoperative medical issues that delay postoperative recovery; (2) multimodal, multidisciplinary team solutions, including anesthesiologists, surgeons, nurses, and other health care professionals; and (3) utilization of interactive and continuous audit of ERAS item compliance and postoperative complications. There are 24 core items of ERAS care supported by scientific evidence. These items are distributed along the patient's perioperative journey and delivered by various health care professionals. 4
Different types of surgical procedures employ variations of (and occasionally additions to) the aforementioned 24 core items. Currently, 12 ERAS official guideline sets exist, including 1 for pancreaticoduodenectomy and 1 for hepatectomy. This brief overview will address general principles related to ERAS guidelines within hepatopancreaticobiliary (HPB) surgery for pancreaticoduodenectomy and hepatectomy, including overarching themes, current areas of debate, and benefits observed to date.
The pancreaticoduodenectomy ERAS society guidelines
The pancreaticoduodenectomy ERAS Society guidelines were published in two major medical journals in 2012 and in 2013.5,6 They comprised 27 items—8 preoperative, 8 intraoperative, and 11 postoperative. To compile the 27 recommendations, all co-authors screened Web-based databases for relevant archives. Emphasis was given to publications of better quality (randomized trials, systematic reviews, and meta-analyses). Quality of evidence and recommendations was evaluated according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system: quality of evidence was categorized as High, Moderate, Low, and Very Low, whereas recommendations were categorized as Strong or Weak. 7 The strength of recommendation for each guideline item was decided unanimously among the authors.
A few of these 27 evidence-based recommendations, such as the avoidance of preoperative biliary drainage (item 2), the immediate postoperative removal of the nasogastric tube (item 18), or the early removal of the operative anastomotic drain (item 20), were initially approached with caution by the HPB surgeons. However, 5 years later, most major centers of HPB Surgery utilized them uniformly. 8 On the other hand, despite the strong recommendation by the ERAS Society guidelines, other items are still debated and not widely applied. 9 Common examples include the limitation of preoperative fasting in patients with preoperative gastroparesis and oral carbohydrate loading in diabetics (item 7).
Although progressive, the ERAS Society guidelines for pancreaticoduodenectomy are already 5 years old. Like all evidence-based recommendations on medical practices, they should be constantly revisited and revised as new evidence appears or new observations are made. Areas that will need to be addressed in the next guideline revision include the observation that delayed gastric emptying is reported to be increased in HPB centers that advocate for early removal of the nasogastric tube; guidelines will also need to address the postoperative pancreatic enzyme supplementation. 10
The hepatectomy ERAS society guidelines
The hepatectomy ERAS Society guidelines were published in 2016, although there have been earlier reports on liver resection results from centers that apply generic ERAS principles.11,12 They comprise 23 items—5 preoperative, 9 intraoperative, and 9 postoperative. The drafting process was somewhat different than previous ERAS guidelines with the initial literature search carried out by five ERAS International Society appointed members. After identifying 1867 relevant records and eventually analyzing 37 studies, the appointed members came up with recommendations on the aforementioned 23 items.
The recommendations were then sent to seven international experts within the field of HPB surgery. Through a three-round Web-based modified Delphi approach, a consensus was reached and recommendations were made based on the GRADE system: once again, quality of evidence was categorized as High, Moderate, and Low, whereas recommendations were categorized as Strong or Weak. 7 Of note, these ERAS guidelines do not apply to cirrhotic patients undergoing hepatectomy.
Some interesting, and until recently not widely appreciated, recommendations were made unanimously, such as employment of minimally invasive hepatectomy for tumors in segments 2, 3, 4b, 5, and 6 (item 11) and utilization of an omental flap to prevent postoperative delayed gastric emptying (item 17). On the other hand, there was significant amount of skepticism regarding the use of thoracic epidural catheters (item 20) in major liver resections (due to possible hepatic failure and subsequent hemorrhage). In addition, posthepatectomy goal-directed resuscitation (item 22) stirred some controversy, up to the point that it reached the third round of the Delphi process before achieving a consensus for recommendation.
Besides prospective validation of the already existing hepatectomy ERAS Society guidelines by many centers around the world, the obvious next step is the development of similar recommendations for cirrhotic patients undergoing hepatectomy. This is an attainable goal that will likely be realized in the next 18 to 24 months.
ERAS principles and areas of debate within HPB surgery
Preoperative fasting and oral carbohydrate load
Prolonged fasting before elective surgery has been the historical standard to help ensure an empty stomach to reduce the likelihood of regurgitation of gastric contents during the induction of anesthesia and possibly resulting in aspiration pneumonitis and pneumonia. With the advent of ERAS programs, fasting intervals have been reduced to a recommendation of 2-hour fasting for clear liquids. 13 In addition to reduced fasting intervals for clear liquids, enhanced recovery patients are encouraged to consume a clear, complex carbohydrate drink 2 hours before the induction of anesthesia. 14 This carbohydrate load has been shown to reduce thirst and anxiety as well as insulin resistance.15,16 In addition, the consumption of a carbohydrate drink has been shown to reduce hospital length of stay. 17
In patients with normal gastric emptying, this practice does not alter gastric volume or pH, or increase the risk aspiration; however, patients with obstructive masses or ascites may be at an increased risk for delayed gastric emptying, reflux, and regurgitation during induction of anesthesia.18,19 In these patients, the fasting interval may need to be increased and the carbohydrate clear liquid consumption omitted in patients deemed to be at an increased risk of aspiration. Specifically, for patients undergoing pancreatectomy, we must be cautious of the especially high incidence of preexisting or new-onset diabetes in the perioperative period. 20 Patients with diabetes will be at a higher risk for gastroparesis, perhaps precluding preoperative carbohydrate loading. 21 For patients undergoing hepatectomy, poor perioperative glycemic control has been associated with impaired regeneration of the liver remnant. 22
Intraoperative and postoperative fluid management
Intraoperative fluid management has been identified as a key component of enhanced recovery success in a colon rectal surgery. 23 Specific goal directed fluid therapy (GDFT), defined as the use of relatively small fluid colloid boluses over small background crystalloid infusions intended to increase stroke volume and cardiac output, has been associated with increased gut perfusion and decreased gut mucosal acidosis. 24 Recent studies have suggested when less invasive procedures are used and conventional, somewhat restricted fluid management strategies are employed, there may be less advantage to GDFT. 25
Intraoperative fluid management may be even more important when caring for patients undergoing pancreaticoduodenectomy with the risk of pancreatic fistula formation associated with intraoperative fluid excess. 26 Similar benefits have been observed for hepatic resection with goal-directed fluid resuscitation associated with improved liver function following hepatectomy with decreased perioperative complications. 27 Proper fluid management begins with liberalization of access to clear fluids up to 2 hours before the induction of anesthesia in patients with normal gastric emptying. With limited or iso-osmotic bowel preparation, there is no fluid deficit requiring crystalloid replenishment. Fluid replacement should be conservative, but not overly restrictive. The surgical and anesthesia teams should have preagreed, acceptable hemodynamic and urine output parameters. When clinically warranted, advance hemodynamic monitoring equipment and arterial blood sampling of acid base status and hemoglobin determination can direct fluid therapy. Perioperative cumulative fluid balance has been associated with adverse outcomes when there is a significant positive fluid balance. 28
Accurate determination of fluid balance is problematic with difficulty estimating intraoperative blood loss and tissue fluid accumulation due to surgical manipulation. Fluid replacement strategies that involve minimal crystalloid administration with one to one colloid replacement of blood loss are a good starting point. Hemodynamic parameters, urine output, and acid-base status may dictate more aggressive volume replacement, particularly after completion of the reconstructive phase of the procedure.
Analgesia
Adequate pain control after surgery, which allows sufficient patient comfort to allow for rapid functional recovery after surgery, is a crucial component of ERAS programs. Multimodal pain therapies involving nonopioid pain medications, judicious use of small amounts of short-acting narcotics, and regional pain management techniques promote patient satisfaction, reduced narcotic-related complications, and earlier discharge. 29 The United States is in the midst of an opioid crisis. A recent study showed 1 in 30 narcotic-naive patients continue to use opioids for more than 3 months after major surgery. 30 ERAS patients treated with multimodal pain protocols have significantly reduced requirements and rates of opioid use on discharge. 31
Preemptive analgesia with acetaminophen, cyclooxygenase-2 inhibitors, gabapentinoids, and ketamine reduce opioid consumption and opioid-related side effects. 32 As an analgesia adjunct, intravenous infusions of xylocaine reduce opioid requirements, improve return of bowel function, and shorten length of hospital stay in some groups. Xylocaine infusions are useful when regional anesthesia is not clinically feasible or when more minimally invasive procedures are used. Xylocaine clearance may be altered in patients with significant hepatic dysfunction and should be used cautiously, and at reduced infusion rates, in these patients. 33
Thoracic epidural analgesia continues to be a major component of pain management for hepatopancreatobiliary surgical patients, particularly when cases are performed using significant incisions. Thoracic epidural analgesia has been shown to provide superior analgesia when compared to intravenous narcotics, including studies when patient-controlled analgesia is the technique of choice. 34 Epidural analgesia has been shown to reduce pulmonary complications, reduce insulin resistance, and decrease the prevalence of ileus. However, thoracic epidural analgesia has been associated with more hemodynamic instability and may be problematic in patients with coagulopathy associated with liver disease. 35
Clinical outcomes after implementation of ERAS society guidelines for HPB surgery
Pancreatoduodenectomy is a highly complex procedure that carries significant perioperative mortality and morbidity, 5% and up to 60%, respectively. In addition, median length of stay can be as long as 20 days. A systematic review and meta-analysis of enhanced recovery after pancreaticoduodenectomy by Coolsen et al. revealed that ERAS Society guidelines were associated with a significant decrease in length of stay, up to 6 days without an increase in readmission rate. In this particular meta-analysis, differences in rates of pancreatic fistula and delayed gastric emptying were not statistically significant; however, no discrete compliance elements were recorded. 36 On the other hand, it has recently been shown that reaching an overall compliance of 70% in pancreatoduodenectomy ERAS Society guidelines items can improve key metrics, such as 30-day readmission rate (35% from 53%) and 30-day reoperation rate (8% from 20%). 37
Although the hepatectomy ERAS Society guidelines were published within the last year, their possible benefit can be inferred by earlier publications that employ similar enhanced recovery pathways demonstrating decreased complications and length of stay. 38 In fact, there was already enough evidence to perform a meta-analysis of randomized trials of enhanced recovery programs versus traditional care in hepatectomy, reporting a decrease by more than 2 days in length of stay and by 34% in rate of complications. 39
On the other hand, one of the centers that co-authored the hepatectomy ERAS Society guidelines recently published their experience in liver resections following the 23-item recommendations with a compliance rate exceeding 70%. The reported decrease in rate of complications was 16%, and the reported decrease in intensive care unit length of stay was 2 days. 12
Financial implications after implementation of ERAS society guidelines for HPB surgery
Since the development of the ERAS protocol in 2001 by the ERAS Study Group, there has been continuous reporting of not only important clinical but also financial benefits. Most reports of ERAS-related financial benefits for various types of operative procedures come from single institutions; there is a positive correlation between ERAS item compliance rates and favorable financial outcomes. The same is true in HPB Surgery. For example, Joliat et al. demonstrated a decrease of pancreaticoduodenectomy mean cost from €63,821 to €56,083, after implementation of the ERAS guidelines with a 70% item compliance rate. 40 In addition, a cost-benefit analysis after adoption of ERAS hepatectomy guidelines, coming from Switzerland, revealed a €3,630 cost saving per patient. 12 Most recently, Wang et al., in a meta-analysis of five studies with complete financial data, reported a 31% decrease in total cost for hepatectomy after enhanced recovery pathway implementation. 41
Another financial implication of ERAS guideline implementation in the field of resource-intensive HPB Surgery pertains to the itemized structure of the guidelines themselves, a detail that facilitates monitoring the impact of any newly adopted intervention or policy. For example, Tezber et al. utilized institutional analytic algorithms to identify patients at low risk of severe complications after pancreaticoduodenectomy and hepatectomy; these low-risk patients received reduced sets of laboratory blood draws for hematologic and biochemical profile evaluation. 42 This resource restrictive practice was incorporated within the ERAS pathways for the two procedures and therefore implemented, monitored, and assessed in the same way as the remaining ERAS items. After 1 year of adoption, out of 183 patients (79 pancreaticoduodenectomies and 104 hepatectomies), 121 received the reduced blood draws, resulting in almost $350,000 saving in patient charges (Fig. 1).
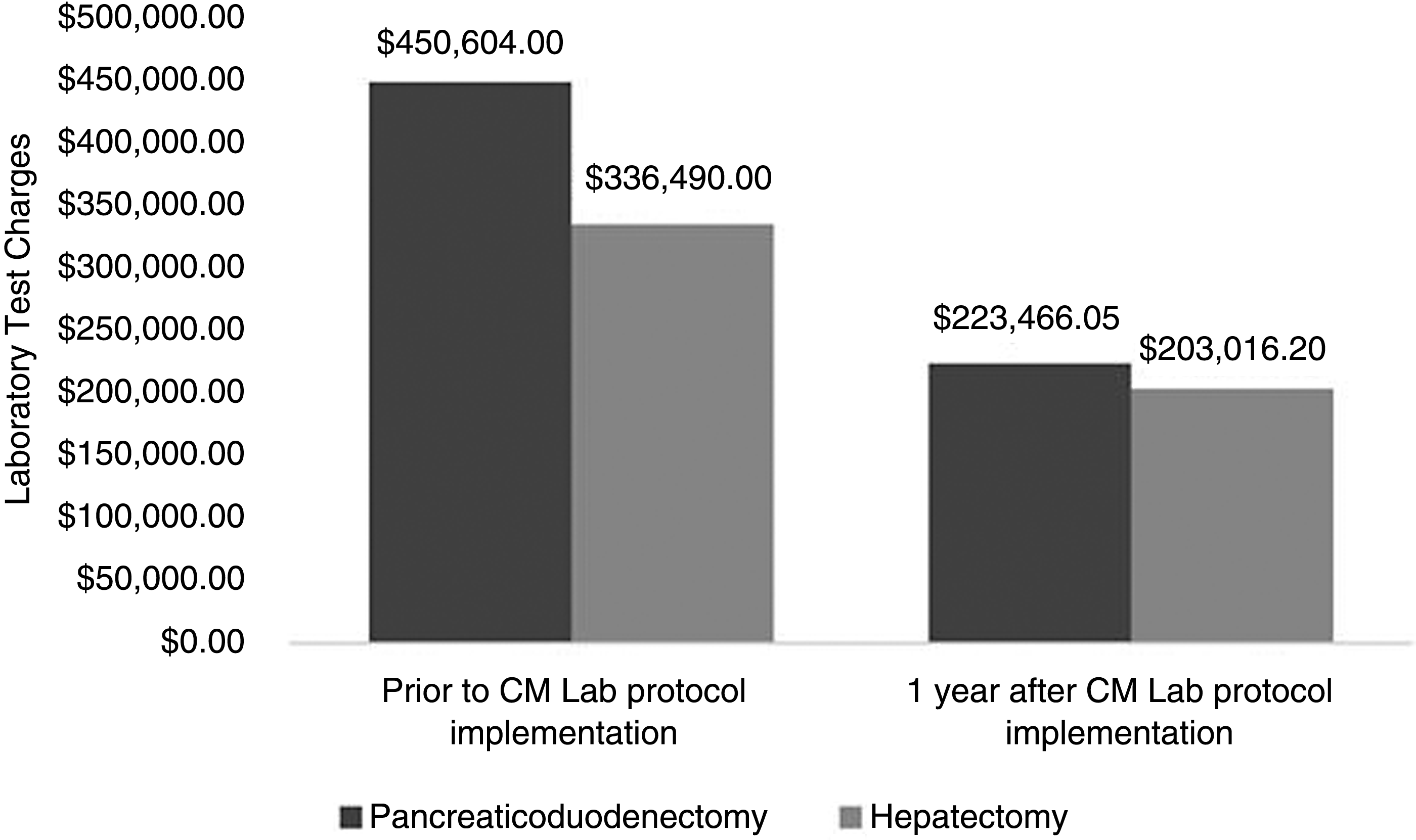
Savings in patient charges over 1 year after adoption of Clinically Meaningful Laboratory Evaluation Initiative in the setting of ERAS® guidelines for pancreaticoduodenectomy (n = 79) and major hepatectomy (n = 104). Reprinted with permission. ERAS, enhanced recovery after surgery.
Conclusions
ERAS guidelines for HPB surgery have the potential to optimize surgical outcomes in a cost-effective manner for patients with a historically high rate of postoperative morbidity and mortality. While specific items within the pancreaticoduodenectomy and hepatectomy guidelines continue to be a topic of debate between major HPB centers, results of recent meta-analyses have shown favorable outcomes, both clinically and financially, with enhanced recovery pathways. Recognizing that guidelines should continue to remain at the forefront of evidence-based surgical care, the ERAS Society is actively addressing topics of debate as well as limitations of current guidelines. Given that the specialty of HPB Surgery is a highly complex, morbid, and resource-intensive surgical discipline, the ability to improve clinical outcomes, while simultaneously conserving limited resources in health care, solidifies ERAS as a key component of perioperative care in the current era of value-based care in medicine.
Footnotes
Acknowledgment
All work related to this project is internally funded within the Division of HPB surgery and Department of Surgery at Carolinas Medical Center.
Disclosure Statement
No competing financial interests exist.