
Abstract
Abstract
Purpose:
In some patients with recurrent inguinal hernias who have undergone previous laparoscopic herniorrhaphy, dissecting the entire posterior wall is difficult due to mesh adhesion. We applied a novel transabdominal preperitoneal (TAPP) hernioplasty technique that involves closing of the hernia defect and implantation of a newly added mesh while preserving the pre-existing mesh for inguinal hernia recurrence after laparoscopic herniorrhaphy. This study was performed to evaluate this novel technique for treatment of recurrent inguinal hernias.
Methods:
We evaluated 24 adult patients (23 male, 1 female; mean age, 55.8 ± 14.0 years; range, 26–77 years) with recurring inguinal hernias. A modified TAPP (mTAPP) procedure involving closing of the defect and implantation of an 8 × 6-cm2 newly added mesh was performed. The new technique covered the whole posterior wall with pre-existing mesh.
Results:
Among the 24 patients, there were 12 direct hernias and 12 indirect hernias. The mean postoperative pain scores after 1 week were 2.5 and 2.0 in patients with direct and indirect hernias, respectively, and the mean duration until return to normal activities was 8.5 and 7.5 days in patients with direct and indirect hernias, respectively. The mean follow-up period was 21.0 ± 17.0 (range, 2–56) months. No chronic inguinodynia or rerecurrence was observed.
Conclusions:
In this novel mTAPP procedure for recurring inguinal hernias, closing sutures prevented mesh migration, and complete posterior wall overlap was possible using the pre-existing mesh and newly added mesh. The mTAPP procedure was an effective operation with few recurrences and complications.
Introduction
Surgical management of recurrent inguinal hernias is challenging. The current guidelines recommend a laparoscopic operation and large-sized mesh for the treatment of recurrent inguinal hernias originally repaired with a primary open approach, and an open approach for the treatment of recurrent inguinal hernias originally repaired with a primary laparoscopic operation.1–4 Nonetheless, successful treatment of recurrent hernias using laparoscopic procedures for subsequent hernia repairs after a primary laparoscopic operation has also been reported.5–11 Although laparoscopic transabdominal preperitoneal (TAPP) hernioplasty is widely accepted due to its various advantages such as accurate identification of the defect site with low postoperative pain, an associated major problem is the requirement for wide preperitoneal dissection for mesh implantation. In some patients with recurrent hernias who have previously undergone primary laparoscopic herniorrhaphy, dissection of the entire posterior wall is difficult because of pre-existing mesh adhesion. Therefore, implantation of new large-sized mesh is difficult in some patients with recurrent hernias. Furthermore, removal of the pre-existing implanted mesh is not easy. Although the defect wall-closing technique is another treatment option for ventral hernias and groin hernias,12–14 no studies have evaluated this method for recurrent inguinal hernias. Therefore, we applied a novel technique in which suture closing of the hernia defect is combined with implantation of a newly added mesh for the treatment of recurrent inguinal hernias. The new technique covers the whole posterior wall with pre-existing mesh in a pants-and-vest shape (Fig. 1). This procedure also allows for reinforcement of the entire posterior wall. Therefore, the same effect as in repair using large mesh according to the current guideline can be observed. The aim of this study was to evaluate this novel technique for treatment of recurrent inguinal hernias. We evaluated the recurrence rate, postoperative course, and complications.
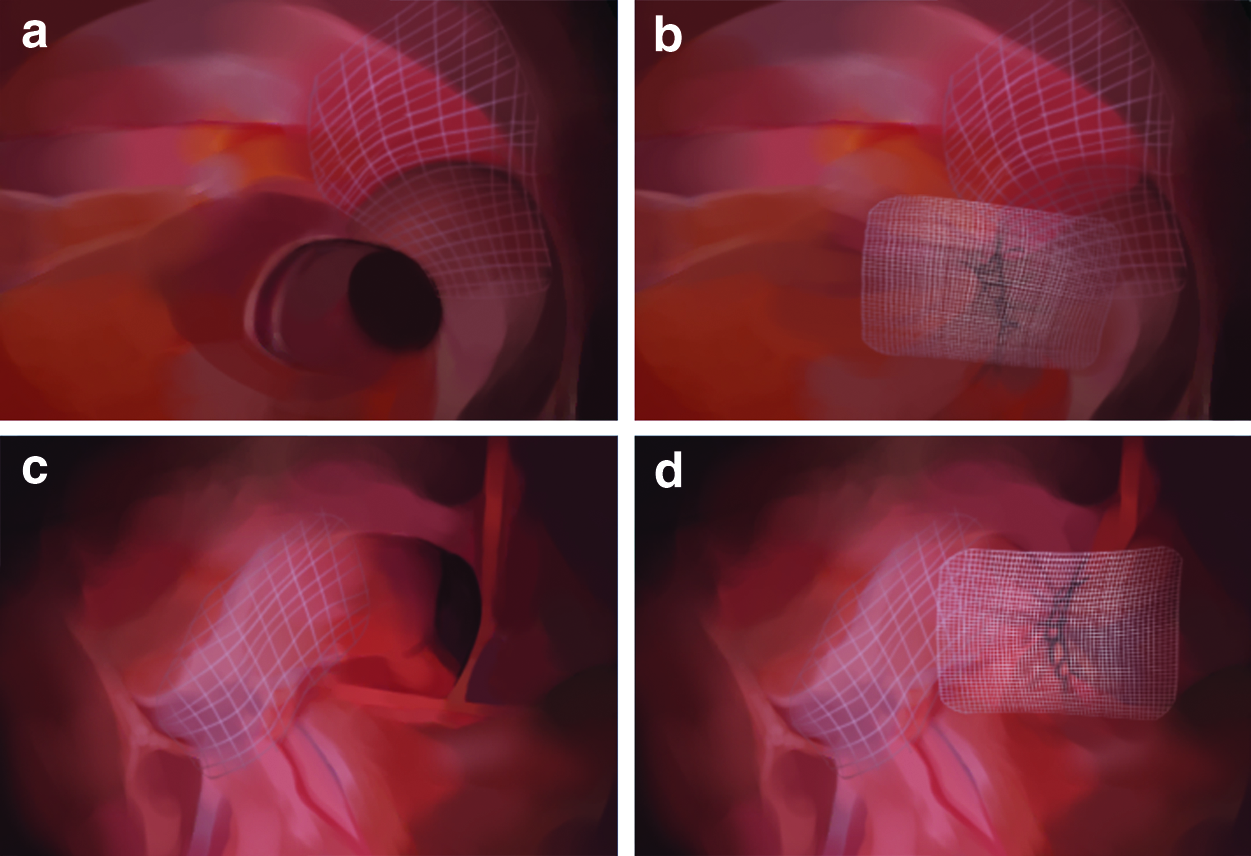
Drawing of mesh and coverage of whole posterior wall:
Materials and Methods
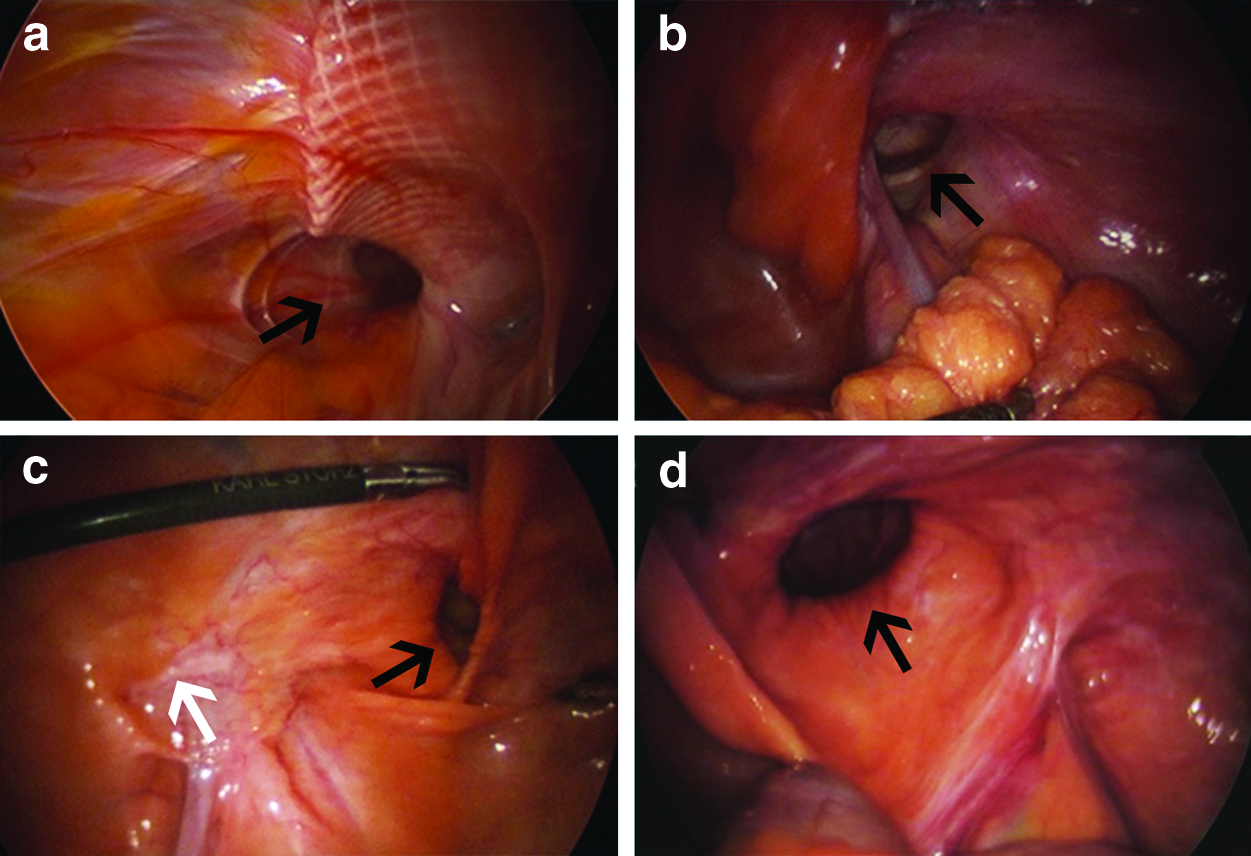
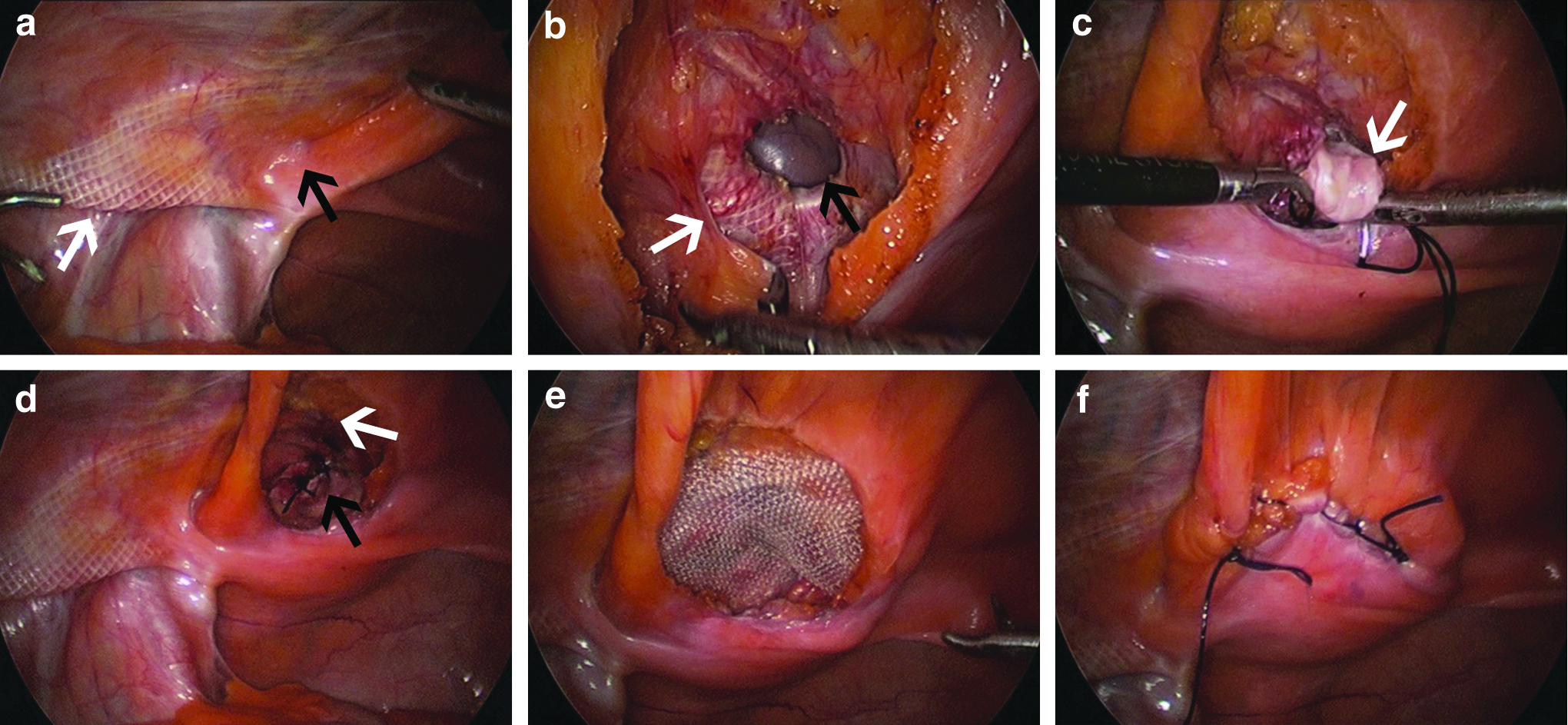
A retrospective analysis of the case records of 24 patients who presented with recurrent inguinal hernias at Damsoyu Hospital from September 2012 to December 2017 was performed. The patients' history, including the initial hernia type and the surgical method used, was confirmed by checking the medical records obtained from facilities at which the initial procedure had been performed. The inguinal hernias were categorized as indirect (lateral, Fig. 2a, b) or direct (medial, Fig. 2c, d) based on their location. A modified TAPP (mTAPP) procedure was performed, which involved closing of the hernia defect and implantation of an ∼8 × 6-cm2 polyester mesh (Figs. 3 and 4). This study was approved by the Institutional Review Board of Damsoyu Hospital.
Recurrent inguinal hernia in adults:

Reoperation of a recurred right indirect inguinal hernia by mTAPP hernioplasty:
Reoperation of a recurrent direct inguinal hernia by modified mTAPP hernioplasty:
Inclusion and exclusion criteria
All patients included in this study presented with a recurrent inguinal hernia that had initially been repaired by previous laparoscopic hernioplasty. All patients aged ≥20 years and requiring elective hernioplasty for treatment of a recurrent inguinal hernia were included in this study. All data were retrospectively collected by a data manager working at the Damsoyu Hospital research center. One patient who removed pre-existing mesh was excluded. One patient who was lost to routine follow-up after the procedure was also excluded from the study. The effective number of patients who were analyzed in this study after following all inclusion and exclusion criteria was 24. All patients underwent surgery after the procedure had been described to them, and their informed consent had been obtained.
Laparoscopic herniorrhaphy technique
All 24 patients underwent TAPP herniorrhaphy with a three-port laparoscopic system. The procedures were performed with the patients under general anesthesia and in the supine position. The laparoscopic system used a 5.0-mm camera and 5.0-mm instruments. A 5.0-mm transumbilical incision was made to create pneumoperitoneum using a 5.0-mm trocar, and carbon dioxide pressure was maintained at 8–12 mmHg. Two other 5.0-mm instruments were inserted through separate 5.0-mm stab incisions in the lateral abdomen. A mesh fixation device was not used.
In the mTAPP procedure for indirect inguinal hernias (Fig. 3), the deep inguinal ring was closed using a nonabsorbable multifilament suture (silk 1–0) as follows: Initially, the bottom portion of the deep inguinal ring was tied and sutured in an upward direction to close the myopectineal orifice. The first stitch was used to tie the lateral and medial walls of the deep inguinal ring with sufficient space for the vas deferens and the spermatic cord vessels to pass through without compression (Fig. 3c). In the mTAPP procedure for direct inguinal hernias (Fig. 4), the defect was closed using a nonabsorbable multifilament suture (silk 1–0). Initially, the bottom portion of the wall defect was tied and sutured in a longitudinal direction to the top of the defect, and then sutured continuously in the opposite direction until the suture came back down and could be tied to the initial knot. The lax transversalis fascia was sutured together during defect repair to decrease the risk of seroma development (Fig. 4c). 15
Protocols and follow-up
The patients were permitted to ingest liquid after 2 hours of observation. The protocol at our institution stipulates that patients shall be discharged if their condition remains stable and if they are comfortable while performing daily activities (such as walking and eating). Postherniorrhaphy pain was evaluated using a 0- to 10-point visual analog scale (VAS). Routine outpatient follow-up included a physical examination at 1 week and 1 month, and an annual telephone follow-up in December every year until December 2017. The follow-up period ranged from 2 to 56 months (mean 21.0 ± 17.0 months). Telephone interviews were performed to obtain information on the patients' postoperative status, such as pain and recurrence.
Results
The patients' characteristics are shown in Table 1. No patient required conversion to open surgery. The mean operation time was 46.5 ± 23.7 minutes for patients with direct hernias and 35.9 ± 13.6 minutes for those with indirect hernias. The duration of postoperative hospital stay was 21.9 ± 15.3 hours for patients with direct hernias and 9.2 ± 5.1 hours for those with indirect hernias. In the direct hernia group, 1 patient developed a surgical site hematoma and 1 developed a surgical site seroma. In the indirect hernia group, 1 patient developed a surgical site seroma and 1 developed an umbilical port site wound infection. The hematoma, seroma, and wound infection subsided with conservative treatment. No chronic inguinodynia was observed in either group, and the mean postherniorrhaphy VAS pain score was 2.5 ± 2.3 in the direct hernia group and 2.0 ± 2.7 in the indirect hernia group 1 week after the procedure. The mean period until return to normal activities was similar in the two groups (8.5 and 7.5 days in the direct and indirect hernia groups, respectively). No chronic complications or rerecurrence occurred in either group.
Characteristics of Adult Patients who Underwent Reoperations for Inguinal Hernias
Categorical variables are represented as n (%), and continuous variables as mean ± standard deviation (range).
VAS, visual analog scale; F/U, follow-up; TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal.
Discussion
The general guidelines for treating recurrent inguinal hernias recommend open anterior repair if the primary procedure was laparoscopic repair. 1 Although many studies have reported that laparoscopic reoperation reduces the rerecurrence rate after primary open anterior repair, no randomized controlled trials have shown an increase in the rerecurrence rate after primary laparoscopic repair. 2 Furthermore, laparoscopic reoperation is recommended for recurrence after a primary Lichtenstein repair of a direct inguinal hernia. 10
The general guidelines for recurrent hernia repair recommend using a large synthetic mesh for treatment, 16 and many reports have suggested that there is no difference between laparoscopic TAPP and totally extraperitoneal hernioplasty when used to surgically manage recurrence.17,18 Compared with the anterior open approach, the TAPP procedure has a better outcome profile in terms of pain and return to regular activity. 16 A subsequent TAPP procedure has recently been more frequently performed in the management of recurrence after primary laparoscopic inguinal hernia repair, provided adequate surgical expertise is available. 5 Reflecting this, the International Endohernia Society (IEHS) has provided a level III recommendation regarding re-TAPP procedures, and a grade B recommendation that re-TAPP procedures should only be attempted by experts. 16 If no intra-abdominal adhesion is present, the laparoscopic camera can accurately identify the recurrence site and the state of the pre-existing mesh.
No reports have described a combination of suture closure for a hernia defect with implantation of a newly added mesh for hernia recurrence, but this suture closure for a hernia defect has been reported as the primary procedure to manage direct inguinal hernias, adolescent indirect inguinal hernias, and ventral hernias.12–14 When TAPP hernioplasty is performed for recurrent hernias, removing the previous mesh is sometimes difficult, and there is a risk of damage to organs such as the gonadal vessels, vas deferens, and bladder. 16 In this study, the surgeon did not remove the pre-existing mesh if it did not interfere with placement of the new mesh. One report described laparoscopic mesh removal in patients with intractable pain. 19 Consistent with this, the IEHS guidelines include a level IV recommendation that the presence of two or more meshes in the inguinal region does not seem to enhance the frequency of chronic pain, and a grade D recommendation that the previous mesh should be left in place. 16 Therefore, in this study, the pre-existing mesh was not removed if no intractable pain was present except in 1 patient with inguinal pain.
In this study, the numbers of recurrent direct hernias and recurrent indirect hernias were the same. The lateral area in patients with medial recurrence overlapped well with the pre-existing mesh, as did the medial area in patients with lateral recurrence. When the preperitoneal space of the recurrence site was dissected, the defect site was identified and the myopectineal wall was completely visualized. As mentioned in the Materials and Methods section, the myopectineal wall of the defect site was sutured with a suture line of ∼2 cm, which was sufficient for a 3-cm overlap with a newly added mesh of 8 × 6 cm2. The suture procedure used for recurrent indirect hernias was similar to that used for Marcy repair in the open anterior approach. Some studies have reported low recurrence and complication rates associated with Marcy repair for indirect inguinal hernias in adults.20–22 Some reports have described laparoscopic suture repair of inguinal hernia defects.23,24 The new mesh and pre-existing mesh were placed in a pants-and-vest pattern that covered the entire posterior wall over 20 cm. Such closure of the defect using sutures can prevent migration of the mesh, and it is possible to achieve a >3-cm overlap. In general, suture closure is considered to cause tension. However, no strain or tension was noted when the myopectineal wall of the defect site was sutured using a continuous linear suture instead of a purse-string suture. There was no difference in the 1-week postoperative VAS score between the patients who did and did not undergo suturing among adolescent indirect inguinal hernia repairs. 14 Tension-free hernia repair using suture closure has an important effect on recurrence and postoperative pain because tension in the suture site increases the hospital stay due to postoperative pain. In this study, the mean length of the postoperative hospital stay was within 2 days, the mean 1-week VAS score was 2.3, and the mean time taken to return to daily life was 8 days.
Recurrent hernias account for ∼10%–15% of all inguinal hernias.25,26 Furthermore, the risk of rerecurrence is higher after the first reoperation than after the primary operation.2,27 The rerecurrence rate reportedly varies from 1% to 20% depending on the surgical procedure.28–30 Although there is a need for additional follow-up, we observed no rerecurrence. No patients in this study developed chronic inguinodynia, and all cases of seromas and hematomas, which are acute complications, were managed with conservative treatment.
This study has several limitations, including its retrospective design. Some patients had undergone herniorrhaphy in other hospitals for previous treatment of their hernias. In addition, only 24 patients were included in this study, which is a relatively low number for accurate comparison of outcomes. Because the follow-up period was not long, a longer term follow-up would be required to ascertain the actual recurrence rate. This was not a comparative study of mTAPP and standard TAPP.
In conclusion, we evaluated a new technique for treating recurrent inguinal hernias, wherein the defect was treated by implanting a newly added mesh without removing the previous mesh. The mTAPP reoperation could be effectively performed. Reducing the dissection site was possible because the posterior wall, other than the site of recurrence, was covered with the pre-existing mesh placed during the previous operation. Defect sutures prevented mesh migration, and overlap of the entire posterior wall was possible using a combination of the pre-existing mesh and the newly added mesh. This study shows that a re-TAPP operation is easily applied to recurrent inguinal hernias after a TAPP operation. This procedure is potentially applicable because it can reduce the rerecurrence rate and is associated with low postoperative pain.
Footnotes
Acknowledgments
Disclosure Statement
No competing financial interests exist.