
Abstract
Abstract
Background:
The three-dimensional (3D) vision system was released to the medical market to improve laparoscopic outcomes. We analyzed the muscular pain and fatigue, and the performance outcomes after several laparoscopic urologic tasks were completed with the 3D vision system.
Methods:
A total of 49 participants with different surgical expertise levels were enrolled in the study. All the participants performed some laparoscopic urologic tasks using two-dimensional (2D) and 3D vision systems separately. A mini questionnaire survey was also completed by the participants. The duration and quality of the tasks and the muscular fatigue and pain were objectively determined. All the parameters were compared between the 2D and 3D systems.
Results:
Although all the tasks were completed in significantly shorter times with the 3D vision system in each expertise level, maximal shortening was seen in the residents. The overall quality scores were significantly higher with the 3D vision system. However, a maximal increase was seen in the residents. The muscular pain of the participants was lower with 3D vision system. The overall handgrip strength significantly increased from 41.2 to 42.4 kg after the tasks with the 3D vision system, but the difference was significant in only the residents. Twenty-seven participants (56.2%) declared that the 3D system contributed to their performance, and most of the participants (83.3%) preferred the 3D system in the questionnaire survey.
Conclusion:
3D technology may be effective for use in urologic laparoscopic training programs of novice surgeons. It may also contribute to the skills of specialists and experts, shortening the surgical time, which may decrease the surgical morbidity.
Introduction
L
The use of 3D vision system and studies on this topic have increased over time, but there is still a limited amount of data about the effects of the 3D vision system on surgical performance and comfort. 5 Furthermore, to our knowledge, there is no study that has objectively investigated the musculoskeletal effects of the 3D vision system during urologic laparoscopic procedures. The aim of the present study was to analyze the muscular pain and fatigue after the completion of several laparoscopic urologic tasks with the 2D and 3D vision systems and to analyze the performance outcomes of the 2D and 3D vision systems using the completion time of the tasks, the quality of the work, and the results from the questionnaire survey.
Materials and Methods
A total of 49 participants were enrolled in the study. The participants were classified as novices (first-year residents, n = 18), specialists (general surgeons, gynecologists, and urologists, n = 16), and experts (expert gynecologists, general surgeons, and urologists, n = 15) according to their surgical expertise levels. Surgeons who completed the laparoscopic training program during their residency were described as specialists. The expert group consisted of surgeons who completed further laparoscopic training or laparoscopic fellowship programs. All the participants approved participating in the study. The study was conducted in our institute with a laparoscopic surgical training box. All the participants performed several tasks requiring bimanual surgical ability, hand–eye coordination, spatial adaptation, suture and clipping techniques, and cutting skills. Polyglactin 3-0 suture material (Pegelak® 3-0; Dogsan, Trabzon, Turkey), a nonabsorbable polymer vascular clip (Hem-o-lok®; Teleflex Medical, NC), Hem-o-lok appliers (Teleflex Medical, NC), and conventional laparoscopic instruments (Karl Storz, Tuttlingen, Germany) were used during the practices. We preferred to use the European Basic Laparoscopic Urologic Skills (E-BLUS) examination tasks 9 for the study. The descriptions of the tasks are presented in Table 1. All the participants performed each task in a random order using a conventional 2D full-HD vision system (Karl Storz, Tuttlingen, Germany) and using a 3D HD vision system (Viking Systems, La Jolla, CA) with 30° optics, separately. A 60 minute resting time was allotted between the 2D and 3D vision system procedures. In addition, vesicourethral anastomosis (VUA) was also performed by the participants with a training box VUA Kit (3-Dmed® Learning Through Simulation; Medical Training Simulators, OH) at the end of the 2D and 3D vision system procedures as the last task.
The completion time and quality of the tasks were measured using a four-item checklist (Table 1), which is similar to that previously described by Brinkman et al. 9 Scores of 0 and 1 were applied for each error and each successful procedure, respectively. The quality of VUA was assessed considering the intervals between the sutures and the tightness of the knot by assigning scores of 0 and 1 for each error and successful procedure, respectively. We objectively examined the pain and muscular fatigue of the participants in their dominant upper extremities using the visual analog scale (VAS) and a measurement of their handgrip strength, respectively. Basal handgrip strengths and handgrip strengths after the completion of all the tasks with 2D and 3D vision systems were separately determined using a hydraulic hand dynamometer (Jamar® hydraulic hand dynamometer; JA Preston Corporation, Clifton, NJ). Three different measurements with 60-second intervals between repetitions were performed for 5 seconds during each examination to provide the optimal handgrip test, and the mean handgrip strength level was determined. Finally, a nine-item mini questionnaire survey about the experiences with the 2D and 3D vision systems was filled out by the participants. The questionnaire form is shown in Table 2.
2D, two-dimensional; 3D, three-dimensional.
The completion times of each task, overall quality scores of the tasks, VAS scores of pain in the dominant upper extremity and measurements of the dominant upper extremity's handgrip strength, which served as indicators for muscular fatigue, were compared between the 2D and 3D vision systems. The results of the questionnaire survey were also evaluated. The statistical analyses were performed using SPSS 22 software (IBM Corp., Armonk, NY). Test of normality was performed with the Kolmogorov–Smirnov method. The data are expressed as the median and interquartile range. A presentation of the questionnaire survey data was also provided, which expressed the number and ratio. Comparisons of the completion times of each task between the 2D and 3D vision systems were performed with the Wilcoxon test in each expertise level separately. Differences in the total completion times of the tasks between the 2D and 3D systems were also compared between the expertise levels using the Kruskal-Wallis test. Total quality scores of the participants for the tasks were compared between the 2D and 3D systems with the Wilcoxon test. For the comparison of the VAS scores between the two systems, the Mann-Whitney U test was used. The basal handgrip strengths and handgrip strength levels of the participants after they completed all the tasks were compared between the 2D and 3D systems separately using the Wilcoxon test. A comparison of the differences in the basal and after-tasks handgrip strengths between the two systems was also performed with the Mann-Whitney U test in each expertise level. The results of the questionnaire survey were evaluated with Microsoft Excel software (Microsoft Corporation, Redmond, WA). Confidence intervals were set at 95% for all the statistical analyses, and a P value of less than .05 was accepted as significant.
Results
All the participants completed the tasks. The questionnaire survey was also completed by all the participants, except for one expert surgeon. Eighteen of the 49 participants (36.8%) were novices, whereas 16 (32.6%) and 15 (30.6%) of them were specialists and experts, respectively. All the tasks were completed in significantly shorter times with the 3D vision system in each expertise level (Table 3). Although maximal shortening in the total procedure time was seen in residents (522 seconds), substantial decreases were also detected in the specialists and experts (Table 4). The experts had the highest overall quality scores, which were 4 and 5 points, respectively, with the 2D and 3D systems. The overall quality scores were significantly higher with the 3D vision system than with the 2D system in each expertise level (Table 5). However, a maximal increase in the median overall quality score was seen in the residents (2 additional scores). The overall median VAS score of the pain in the dominant upper extremity was lower with the 3D vision system for the participants (1 versus 3, P = .001). The overall median baseline handgrip strength of the participants decreased from 43.4 to 43.3 kg after the completion of all the tasks with the 2D vision system (P = .01). In contrast, it increased from 41.2 to 42.4 kg after completion of all the tasks with the 3D vision system (P = .03). However, the difference in the baseline and after-task handgrip strength levels with the 3D system was significant in only the residents (Table 6). According to the questionnaire survey, 32 participants (66.7%) had difficulty with the 2D system's depth perception. However, of these participants who had difficulty, only 3 were experts. Twenty-seven participants (56.2%) declared that the 3D system contributed to their task performance. Most of the residents (77.8%) thought that the 3D system contributed to the task performance, but the great majority of the experts (78.6%) disagreed. Nevertheless, most of the experts (85.7%) preferred the 3D system to the 2D system in the questionnaire survey. The results of the questionnaire survey are shown in Table 7 and Figure 1.
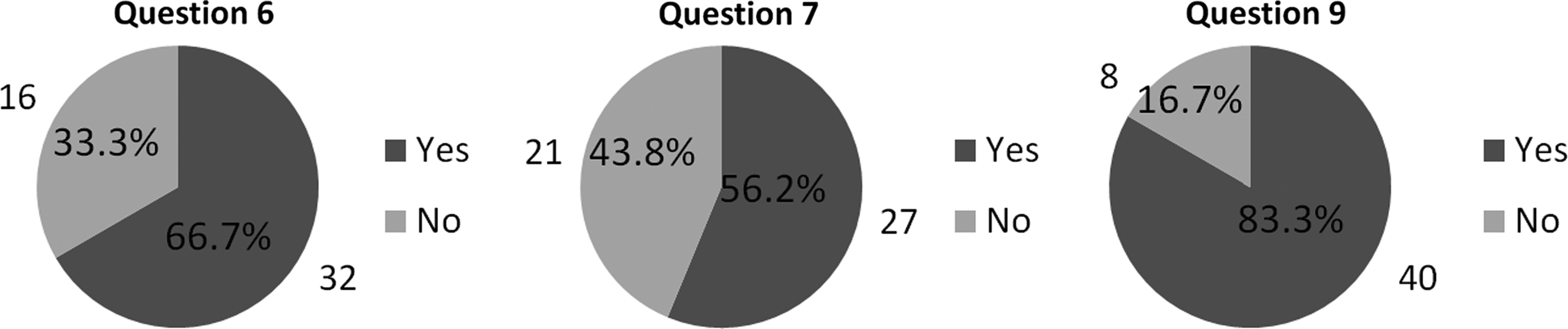
Numeric distributions of the reply to the questions 6, 7, and 9 in overall participants.
Wilcoxon test.
2D, two-dimensional; 3D, three-dimensional; VUA, vesicourethral anastomosis.
Kruskal-Wallis test.
Wilcoxon test.
2D, two-dimensional; 3D, three-dimensional.
Mann-Whitney U test.
Kruskal-Wallis test.
2D, two-dimensional; 3D, three-dimensional.
Discussion
The use and advancement of laparoscopic procedures have improved the surgical outcomes and patient satisfaction, resulting in minimal invasiveness, a shorter hospital stay and a reduction in pain. However, laparoscopic surgery can include some difficulties compared with conventional open procedures. The well-known difficulties are the limited freedom of the surgeons with restricted movements and tactile feedback during the laparoscopy. 10 During the laparoscopic surgery, surgeons commonly stand with a fixed head and neck position and with increased upper body muscle effort, which may result in pain and fatigue during and/or after the procedure. 6 Visual misperceptions from reduced depth perception and spatial orientation due to the lack of the natural binocular vision with a 2D display also contribute to the emergence of pain and muscular fatigue. 11 3D vision systems have been generated to improve the surgical visualization and to overcome the disadvantages of 2D vision systems.7,8 Although literature has contradictory results, the majority of the previous reports showed that the 3D vision system improved the operative performance and had a reduced procedure time with higher efficiency. It also has been reported that the 3D vision system provide more comfort to the surgeons.5,7,8,12 It seems that the major disadvantage of laparoscopic surgery is the 2D vision system, which may worsen the surgical performance and outcomes, and thus, advanced laparoscopic skills, such as suturing, tying, and comprehensive dissection, require adequate surgical maneuvers with tactile feedback and depth perception. Indeed, laparoscopic surgery with 2D vision system increases visual, mental, and physical strain in surgeons. 13 Most of the surgeons experienced better visualization and reported subjectively less physical strain with 3D vision systems in contrast with 2D systems.14,15
Initially, the use of 3D vision during laparoscopy was blamed for the development of several side effects, including dizziness, headaches, eyestrain, and physical discomfort. However, later on, with further reports about the new generation 3D vision systems, these results were considered contradictory. 7 There were contradictory results about the effects of 3D vision systems on surgical outcomes as well. Some early reports did not find any difference between the 2D and 3D vision systems, while others reported that there were more adverse effects, such as dizziness, visual discomfort, and headache, with the 3D vision systems. However, in time, technical advancements in the stereoscopy provided advanced 3D vision systems with better outcomes. Only a small number of new studies showed side effects with the 3D vision system, and further studies showed no difference in the adverse effects between the 2D and 3D vision systems. Moreover, some studies reported better surgeon tolerance with the 3D vision systems. 16 Currently, the common opinion about the 3D vision system is that it increases the accuracy of the laparoscopic performance and reduces the surgeon's fatigue. 17
The current study indicated that only 2 participants (4.34%) had side effects associated with the 3D vision system. Moreover, both of these participants had reported the side effects as being of a minimal severity (one point for the question 8 in the questionnaire survey). Our finding is consistent with the findings of the most recent study by Sørensen et al. in March 2017. The authors found that only one side effect, eyestrain, was associated with the 3D vision system, but that the incidence of it was of borderline significance. Therefore, it was not considered to be practical importance by the authors. 7 We detected a significant advantage of the 3D system in terms of the operative performance of the tasks. All the participants completed the tasks with significantly lower times with the 3D system than with the 2D system. The VUA was also completed with significantly lower times by the residents and experts. However, the specialists performed it with similar times using the 2D and 3D systems. Both the residents who did not perform any VUA attempts, as well as the experts who were experienced in performing the VUA, had a stable experience. Therefore, we believe that any enhancement in the visual or technical aspects during the laparoscopy may have improved their performance and speed during the VUA. We also believe that the specialists know that VUA is a difficult surgical procedure, and they always pay attention differently compared to the novice residents and expert during compelling procedures such as the VUA. Therefore, the 3D system may not have any influence on the performance of specialists in all the conditions because they usually take more care during the VUA than the others. However, the specialists performed all the tasks and VUA with a significantly higher total quality score with the 3D vision system, as expected. The total quality scores for the procedures were also significantly higher in the residents and experts with the 3D system. In the literature, Ga large number of studies have been carried out about the effects of the 3D vision system on surgical outcomes, and most of them reported better surgical outcomes, including a reduced operative time with an increased quality and better outcomes.5,10
A recent systemic research investigating studies on general surgery, gynecology, and urology clinical settings and several associated simulated setting reports in regard to the effects of the 3D vision system during laparoscopy have shown the advantages of 3D vision for both the patients and the surgeons. 10 The study also confirmed that the 3D vision system is safe and efficacious. Most of the investigated clinical studies reported several advantages of 3D vision in terms of blood loss and operative time, especially in studies in general surgery and urology field. However, the hospital stay was found to be similar between the 2D and 3D systems. The systematic research also demonstrated a significant advantage with enhanced depth perception and eye–hand coordination in terms of less visual fatigue and neck pain for surgeons performing the 3D laparoscopy. The experimental settings investigated by the same systematic research also reported better surgical performances with the 3D vision. Significantly shorter procedure times were obtained in various tasks, such as peg transfer, shape and paper cutting, suturing, rope, and needle maneuvers. Decreased error rates were also reported in favor of 3D vision. Side effects, including nausea, eye fatigue, and visual disturbances, did not show any significant difference between the 2D and 3D vision systems. 10
Discomfort, pain, and muscle fatigue are common among surgeons who routinely perform laparoscopic surgery because laparoscopic surgical maneuvers require significantly higher electromyographic (EMG) amplitudes in the upper extremity muscles compared with open instruments.18,19 These side effects of laparoscopy have been described as minimal access surgeon morbidity syndrome. 20 Indeed, it has been proved that laparoscopic grasping is associated with more forearm and thumb muscle effort than hemostatic grasping with the open technique. 21 Johnston et al. 22 revealed that surgeons reported usual or frequent hand/wrist pain during 8% of conventional laparoscopic surgeries. They also showed that surgeons reported less frequent problems with neck and back discomfort than with upper extremity pain. The Society of American Gastrointestinal Endoscopic Surgeons carried out a questionnaire survey with the participation of the 149 responding surgeons, and the study showed that 12% of the participants reported pain in the upper extremity and 8% reported neck pain. 21 In another questionnaire survey study for urologic laparoscopic surgery published by Wolf et al., 23 it was revealed that 67%, 11%, 17%, 28%, and 33% of the surgeons reported procedure associated pain in the hand or wrist, elbow, shoulder, neck, and back, respectively. According to these results, musculoskeletal pain linked to laparoscopy commonly occurs in the upper extremities, especially in the hand or wrist. Therefore, we evaluated muscular fatigue and pain primarily in dominant upper extremity of the participants using handgrip strength measurements and VAS scores, respectively.
Our findings indicated that the 3D vision system reduces muscular fatigue of the forearm and hand in the residents. However, it had no significant impact on muscular strength in the specialists and experts. Differences between the median basal and after-task handgrip strengths in the residents were determined as 1.35 and 0.75 kg for the 2D and 3D vision systems, respectively. We believe that handgrip strength was affected in only the residents because the unusual depth perception and spatial orientation with the 2D vision systems make it difficult to perform tasks in them. The binocular vision with the 3D system might have rendered usual surgical visualization for novice residents, which helps them perform the tasks. Moreover, relatively experienced specialists and more experienced experts are used to performing surgical tasks with the 2D vision system, so they have better coordination and spatial awareness. Therefore, we believe that they maintained their muscular strength as a consequence of them not being overstrained by the 2D vision. Although the 3D vision had no positive effects on muscular strength in the specialists and experts, it provided shorter times for each task and enhanced the quality of the surgical works, as stated above. Previously, Uhrich et al. 24 also investigated muscle fatigue in expert and novice surgeons during laparoscopy with the 2D vision. Both the groups were subjected to similar tasks, and EMG signals from the neck and back muscles were collected. They reported a lower degree of muscle fatigue in the expert group than in the novice group. 24 This result of the study supports our hypothesis that the unusual depth perception and spatial orientation with the 2D vision system make it hard for novice surgeons to perform tasks. Indeed, previous relevant studies reported that the 3D system is more helpful for novice surgeons than for surgeons with advanced laparoscopic education and skills. The main opinion of those studies was that laparoscopy with the 3D vision system could reduce the time needed to obtain basic laparoscopic skills, and it hence could be useful during the training period of junior residents.25–28 One of the most recent studies on the topic, by Romero-Loera et al., 28 compared the laparoscopic surgical skills of novices using the 2D and 3D vision systems in a laparoscopic simulator. The results showed that students with no previous experience with laparoscopic surgery or simulators completed the tasks with higher accuracy, in less time, and with a shorter learning curve using the 3D vision system. Our results are consistent with those of Romero-Loera et al. 28 in terms of the effects of 3D vision on residents' laparoscopy performance.
In brief, as specialists and experts have more experience with 2D vision, they are more comfortable using the 2D vision than residents, and they complete the tasks easily. It can be clearly stated that 2D vision becomes a usual and more frequently used method for surgeons as their experience increases. Consequently, a new 3D vision system provides no breakthrough gains in terms of muscular efforts for experienced surgeons, but it has some expected advantages, such as those described above. In novices such as residents who previously did not work with 2D vision enough, a more natural vision with the 3D system provided a higher comfort level and reduced the muscular fatigue with additional advantages than in specialist and experts. According to our findings, the 3D vision system is not an irreplaceable piece of equipment for routine laparoscopic surgery in advanced centers. However, it can be useful in educational terms of urologic laparoscopy, especially during the achievement of the first knowledge about basic laparoscopic tricks and tips.
As in all studies, our study has some limitations to mention. First, the number of participants should be larger to obtain more robust results. Another limitation is that we did not examine the forearm and wrist muscles by EMG. Finally, the lack of the separate evaluation of the VAS scores in residents, specialists, and experts can be considered a limitation.
Footnotes
Disclosure Statement
No competing financial interests exist.