
Abstract
Abstract
Background:
This study presents the initial feasibility of three-port right-side approach-duet totally laparoscopic distal gastrectomy (R-duet TLDG) with uncut Roux-en-Y (R-Y) reconstruction for the treatment of lower- or middle-third gastric cancer.
Methods:
A total of 30 patients who underwent R-duet TLDG with uncut R-Y reconstruction for gastric cancer were enrolled. All patients were treated at the Catholic Medical Center. Reconstructions were performed intracorporeally without special instruments. The clinicopathological characteristics, operative details, postoperative short-term outcomes, and postoperative follow-up endoscopy results were analyzed retrospectively.
Results:
All operations were performed by three-port R-duet TLDG. There were no conversions to an open approach, and no additional ports were placed. The mean operating time was 170 minutes, and the mean number of retrieved lymph nodes was 44. Three patients experienced mild postoperative complications, including small bowel ileus and pneumonia. Follow-up endoscopy was carried out at 3 months. No patients had experienced moderate-or-severe food stasis, alkaline gastritis, or bile reflux during the follow-up period. Recanalization of the biliopancreatic limb was not observed.
Conclusions:
R-duet TLDG with uncut R-Y reconstruction could be safely performed as a reduced port surgery without special instruments.
Introduction
A
After distal gastrectomy in gastric cancer, there are various reconstruction methods available, including Billroth-I (B-I), Billroth-II (B-II), and Roux-en-Y (R-Y). Each of these reconstruction methods has relative advantages and disadvantages; the superior approach among them remains controversial. Indeed, the reconstruction method used is often determined by the location of the tumor and/or the preference of the surgeon.9–11 In 2005, Uyama et al. 12 first outlined a laparoscopic-assisted uncut R-Y reconstruction method following distal gastrectomy. This method reduces both the Roux stasis of conventional R-Y reconstruction and the incidence of bile reflux, and is now widely used due to its satisfactory postoperative outcomes.13–15 However, an analysis of an uncut R-Y reconstruction method in RPS has not been carried out, and only a small number of case series report on the use of this method in early gastric cancer.2,16
In this study, we report the feasibility of R-duet TLDG with uncut R-Y reconstruction along with short-term postoperative outcomes and endoscopic findings.
Materials and Methods
Patients and data collection
Thirty patients who had undergone R-duet TLDG with uncut R-Y anastomosis reconstruction to treat gastric cancer were enrolled to this study. All operations were carried out at the Catholic Medical Center between September 2015 and June 2017. All operations were performed by a single gastric cancer specialist (H.H.L.). The perioperative details, operative details, and pathological data of all enrolled patients were retrospectively collected from the Catholic Medical Center gastric cancer registry. The pathological stage of each specimen was classified according to the American Joint Cancer Committee (AJCC)–Seventh Edition's tumor, node, metastasis (TNM) classification. 17 The histological type was categorized as differentiated or undifferentiated. Cases of poorly differentiated tubular adenocarcinoma, signet ring cell adenocarcinoma, and mucinous adenocarcinoma were assigned to the undifferentiated group.
The remnant stomach was evaluated by endoscopy at 3 months postoperatively using the residual food, gastritis, and bile reflux classification. These findings were reviewed by 2 expert endoscopists. 18 If there was a disagreement between the 2 reviewers, the individual case was discussed until a consensus was reached.
The study was approved by the Institutional Review Board of the Ethics Committee of the College of Medicine, Catholic University of Korea (approval no. KC17RESI0110). Patient records were anonymized and deidentified before analysis.
Surgical procedures
As reported previously, the patients were placed in supine position, and the operator and endoscopist were positioned on the right side of the patient until the duration of the operation. Three ports were used: the first was a 12-mm-diameter camera port located in the umbilical area, the second was a 12-mm-diameter port located in the right lower quadrant (RLQ), and the third was a 5-mm-diameter port located in the right upper quadrant (Fig. 1). 19
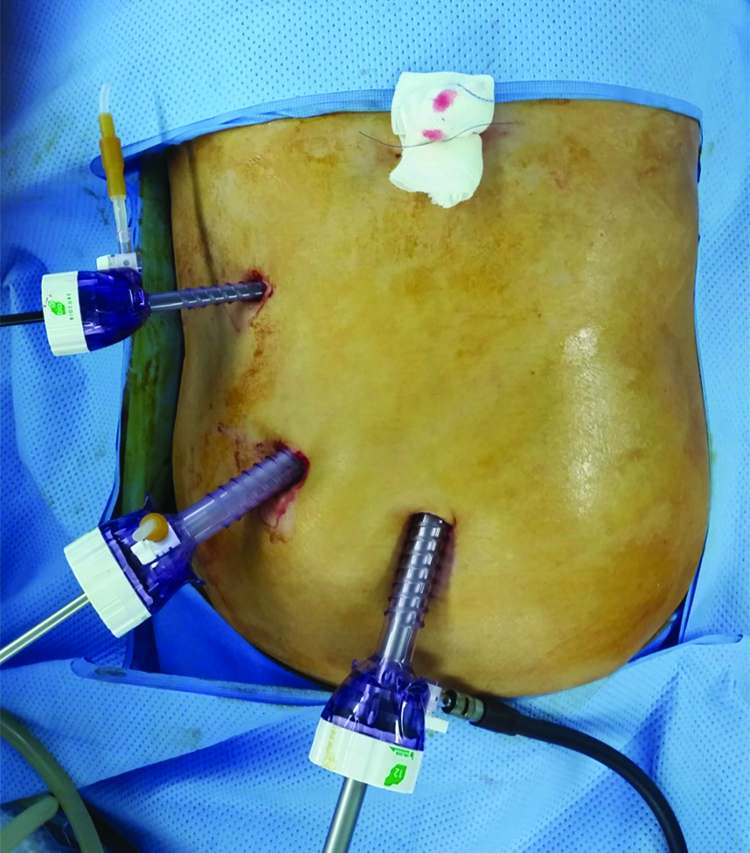
Location of the ports.
The liver was lifted in a V-shape using polypropylene monofilament on a straight-taper needle and two plastic surgical clips. For all cases, a standard radical gastrectomy with lymph node (LN) dissection was performed using conventional laparoscopic instruments, including a rigid laparoscope. Operations were performed according to the Japanese gastric cancer treatment guideline 2014 (ver. 4). 20 Specimens were extracted from the umbilical port following a 2.5-cm vertical extension of the initial incision.
The uncut R-Y reconstruction was performed intracorporeally. First, the proximal part of jejunojejunal (JJ) anastomosis site was marked on the jejunum, 5 cm distal to the ligament of Treitz. Next, the gastrojejunal (GJ) anastomosis site was marked 8 cm distal to the JJ anastomosis site. Then, the distal part of JJ anastomosis site was marked 40 cm distal to the GJ anastomosis site. The lengths of the anastomoses were ∼5 cm. Measurements were done using the open jaws of long-jaw forceps. The distance between the open jaws was ∼4 cm (Fig. 2A). Each anastomosis site was marked with Gentian Violet (Codman & Shurtleff, Inc., Raynham, MA; Fig. 2B). 21 After marking, a side-to-side JJ anastomosis was made through the 12 mm RLQ port, using a 45 mm endoscopic linear stapler (Fig. 2C). Next, an antecolic-antiperistaltic GJ anastomosis was made on the posterior wall of the remnant stomach, using a 60-mm linear stapler (Fig. 2D). The entry hole made by the linear stapler at each anastomosis was closed using intracorporeal hand-sewn sutures (Fig. 2E). After making two anastomoses, the biliopancreatic limb was closed 3 cm proximal to the GJ anastomosis using a nonknife stapler (Fig. 2F, G). After finishing all anastomoses, the mesenteric space under the JJ anastomosis was closed using nonabsorbable multifilament suture to prevent internal herniation (Fig. 2H). The completed uncut R-Y reconstruction is shown in Figure 3A, B.
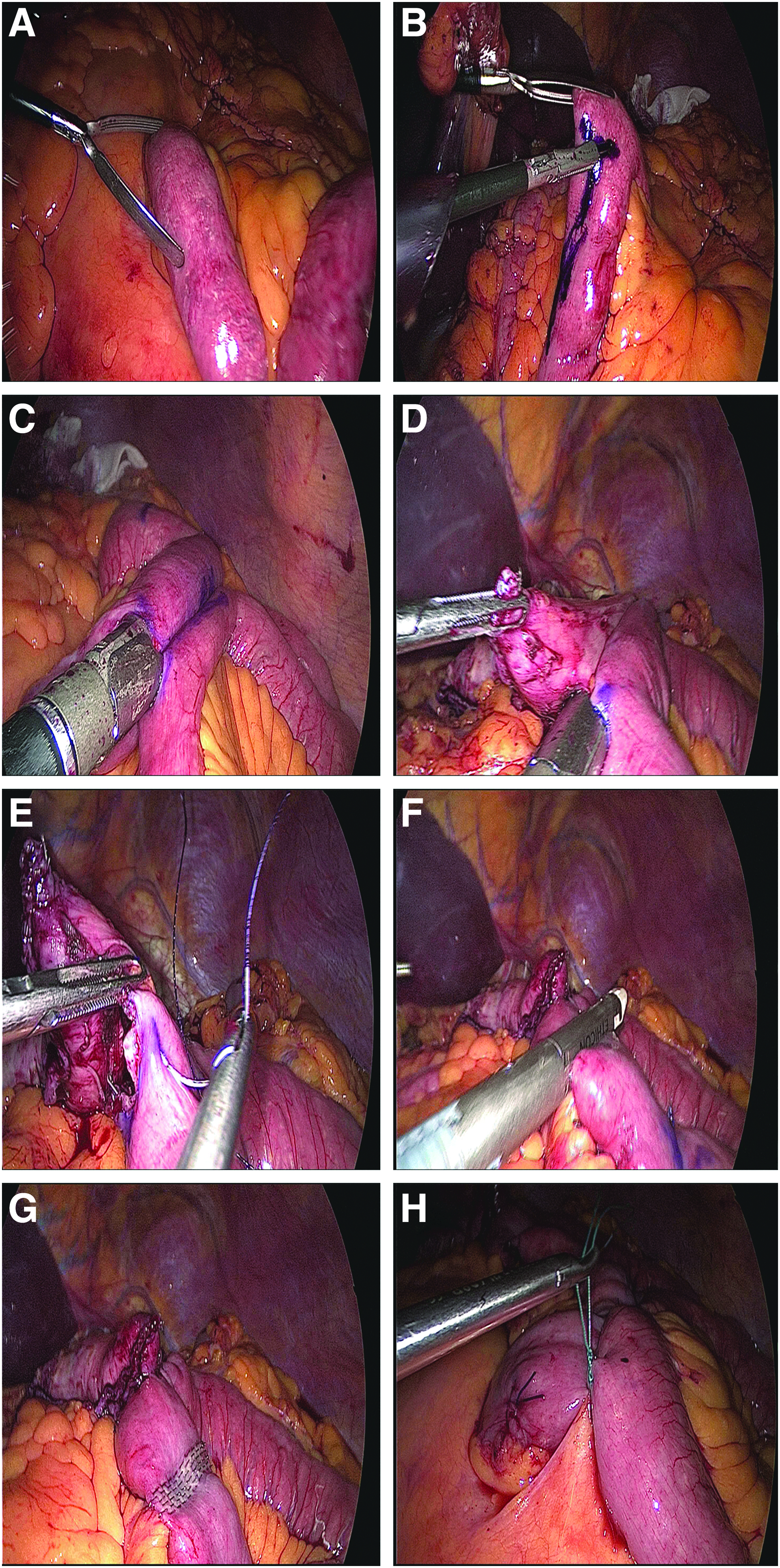
Uncut R-Y reconstruction.

Completed uncut Roux-en-Y reconstruction.
Statistical analysis
Data exploration was used as appropriate. All statistical analyses were performed using SPSS for Windows (ver. 21.0; SPSS, Inc., Chicago, IL).
Results
The patient population included 20 men and 10 women with a mean age of 54.2 years and median body mass index of 23.9 kg/m2. The mean length of the proximal and distal margins was 4.7 and 6.2 cm, respectively. The mean number of retrieved LNs was 44. Twenty-six patients were in stage I and 4 patients were in stage II. All patients underwent R0 resection. The clinicopathological characteristics are given in Table 1.
SD, standard deviation; BMI, body mass index; ECOG, Easter Cooperative Oncology Group; LN, lymph node; R-Y, Roux-en-Y.
All patients underwent R-duet TLDG with uncut R-Y reconstruction. There were no intraoperative complications, and there were no conversions to laparotomy in any case. D2 LN dissection was performed in 21 (70%) patients. The mean operating time was 170.0 minutes, and the estimated mean blood loss was 122.8 mL. The mean duration to flatus and discharge was 2.6 and 7.3 days, respectively. One patient (3.3%) experienced mild postoperative ileus and was managed without medication or surgical intervention. Two patients (6.7%) experienced postoperative pneumonia and were medically managed. The other complications such as surgical site infection, bleeding, anastomotic complications, or pancreatic fistula did not occur in this study. There was no postoperative mortality (Table 2).
Within 30 postoperative days.
LN, lymph node; SD, standard deviation; EBL, estimated blood loss; CD, Clavien–Dindo; R-Y, Roux-en-Y.
The mean follow-up period was 13.5 ± 6.3 months (range, 3–23 months), and there was no morbidity within 30 postoperative days. At the 3-month postoperative follow-up, endoscopic examination showed that minimal or mild food stasis was present in 9 (30.0%) and 4 (13.3%) patients, respectively. No patient had moderate or severe food stasis. Three patients had minimal or mild alkaline gastritis. Of these, 1 had alkaline gastritis around the anastomosis and 2 had alkaline gastritis up to the body of the remnant stomach. There was no moderate or severe alkaline gastritis, and no patient had bile reflux (Table 3; Fig. 4A). No jejunal recanalization of the uncut staple line was observed (Fig. 4B).

Endoscopic findings at the 3-month follow-up:
Three months after the operation.
Discussion
Minimally invasive surgery, such as RPS, has been widely performed for the treatment of gastric cancer. In addition, there is a growing interest in improving postoperative QOL after gastric cancer surgery. 22 Although there are many factors that affect QOL after gastric cancer surgery, one of the most important is the reconstruction procedure. For middle- or lower-third gastric cancer, the recommended treatment is distal gastrectomy with radical LN dissection; however, there is no consensus on the preferred anastomotic method. In most cases, B-I, B-II, or R-Y is used. The unique advantages and disadvantages of each method are determined by the location of the tumor, the progression of the cancer, the condition of the patient, and preference of the operator. 23
A B-I reconstruction procedure creates an anastomosis between the remnant stomach and duodenum and is most similar to the original anatomical structure. However, it requires enough remnant stomach to relieve anastomotic tension, and so is mainly performed in cases of early and distal-third gastric cancer. The B-I method also has several disadvantages, including an increased incidence of food stasis, bile reflux, alkaline gastritis, dumping syndrome, and reflux esophagitis.24–26
A B-II reconstruction procedure creates an anastomosis between the remnant stomach and jejunum and can be performed without regard to the size of the remnant stomach. However, bile reflux and alkaline gastritis occur in most patients. 27 Although Braun anastomosis can be performed to compensate for the bile reflux and alkaline gastritis, they often occur regardless. B-II reconstruction is also associated with afferent loop syndrome, which can occasionally lead to serious complications. 28
A R-Y reconstruction procedure creates an anastomosis between the remnant stomach and the jejunum with an additional JJ anastomosis. Compared with other methods, the R-Y procedure reduces the incidence of bile reflux and alkaline gastritis.28–30 However, the additional anastomosis, the complexity of the procedure, and the longer anastomosis time remain disadvantages. In addition, Roux stasis can occur in up to 30% of patients who undergo the R-Y procedure. 31 Complications in patients with Roux stasis include nausea, postprandial pain, and vomiting food but not bile. 32 Roux stasis is known to be an electrical and motor coordination problem that occurs after jejunal transection. 33 Of note, an uncut R-Y procedure may theoretically address bowel motility issues by eliminating jejunal transection. 34 In this study, food stasis was minimal or mild (43.3% of patients), and there was no moderate or severe food stasis. Moreover, this stasis could have developed due to difficulty controlling the diet after gastrectomy and may be unrelated to intestinal motility. Finally, no patients complained of nausea, vomiting, or postprandial pain during the follow-up period. This result suggests that an uncut R-Y procedure may prevent the Roux stasis seen in conventional R-Y reconstruction. Minimal to mild and limited gastritis was seen in 10.0% of the patients, and no patients had bile reflux. This indicates that an uncut R-Y reconstruction procedure, in addition to preventing Roux stasis, also maintains the advantages of conventional R-Y in reducing the incidence of gastritis and bile acid reflux.
Kitano et al. first described laparoscopic gastrectomy in 1994. Since this initial description, continuous refinements in minimally invasive surgery have reduced both the incisional lengths and the number of ports.3–5,35 We have compared the feasibility of three-port TLDG with four-port and five-port TLDG in previous studies.7,8 One advantage of three-port TLDG is that no special instruments are required during the surgery compared with conventional reduced port or single-incision laparoscopic surgery. In this study, we were able to perform the uncut R-Y procedure with only a rigid laparoscope, long- or short-jawed forceps, and an energy device. A second advantage of the three-port TLDG is that it reduces manpower, requiring only an operator and an endoscopist. The absence of additional assistants may reduce unnecessary trauma and aid in patient recovery postoperatively. 8 In this study, the operator and the endoscopist were located on the right side of the patient. This positioning is similar to conventional five-port TLDG, ensuring a familiar field of view for most operators, as compared with conventional three-port TLDG positioning. 19
The extent of LN dissection is important when performing radical surgery to treat gastric cancer. Although several previous studies have reported the feasibility of using single-incision laparoscopic gastrectomy in the treatment of gastric cancer, the patients enrolled in those studies underwent less than D2 LN dissection. This suggests that D2 LN dissection may be impossible to perform using a single-incision approach.2,16 However, this study included patients with both early and advanced gastric cancer, and 21 (70.0%) patients underwent D2 LN dissection. Our group has previously reported the feasibility of using R-duet TLDG for D2 LN dissection. 19 This study continues these results and demonstrates that, in contrast to single-incision laparoscopic gastrectomy, R-duet TLDG can be used in patients with gastric cancer requiring extended LN dissection.
This study had several limitations including being a retrospective single-arm study with a small number of cases. However, to our knowledge, this is the first study to show the feasibility of uncut R-Y reconstruction in RPS. This study highlights the need for further large-scale comparative retrospective studies or well-designed prospective randomized controlled studies.
In this study, we retrospectively analyzed 30 patients who underwent R-duet TLDG with uncut R-Y reconstruction for the treatment of gastric cancer. R-duet TLDG with uncut R-Y reconstruction had excellent short-term postoperative outcomes compared with conventional TLDG with uncut R-Y.13–15 In addition, the incidence of bile reflux, alkaline gastritis, and Roux stasis was low. In conclusion, R-duet TLDG is a feasible method of performing uncut R-Y reconstruction for the treatment of lower- or middle-third gastric cancer and does not require special instruments. Moreover, it is a reliable method that maintains the advantages of conventional RPS and uncut R-Y reconstruction.
Footnotes
Acknowledgments
This research was supported by grants from the National Research Foundation of Korea (grant nos. 2012R1A1A1043576, 2015R1A1A1A05028000, and 2018R1D1A1B07045486) and the Research Fund of Seoul St. Mary's Hospital, The Catholic University of Korea.