
Abstract
Abstract
Objective:
To contrast the clinical effects and complications for the treatment of liver carcinoma in laparoscopic partial hepatectomy (LPH) and open partial hepatectomy (OPH).
Methods:
The multiple databases were adopted to search relevant studies, and the articles eventually satisfying the inclusion criteria were included. All the meta-analyses were conducted with the Review Manager 5.3, and to estimate the quality of each article risk of bias table was performed.
Results:
In the end, 17 studies including 3897 patients were involved, which eventually satisfied the eligibility criteria. The number of samples in LPH group and OPH group were 1723 and 2174, respectively. The results of heterogeneity test suggested that recurrence rate (odds ratio [OR] = −20.11, 95% confidence interval, CI [−35.93 to −4.29], P = .01; P for heterogeneity <.00001, I2 = 100%), hospital days (mean difference (MD) = −2.21, 95% CI [−2.53 to −1.88], P < .000001; P for heterogeneity = .41, I2 = 58%), and blood loss (MD = −68.09, 95% CI [−85.07 to −51.11], P < .00001; P for heterogeneity = .13, I2 = 37%) were significantly different, whereas operating time (MD = 4.00, 95% CI [−17.50 to 25.49], P = .72; P for heterogeneity <.00001, I2 = 99%) and complication events (OR = 0.68, 95% CI [0.46 to 1.01], P = .05; P for heterogeneity = .34, I2 = 11%) between LPH and OPH were insignificantly different.
Conclusion:
This study demonstrated that clinical efficacy of OPH was better than that of LPH to some extent, but LPH was a quicker recovery and less harmful therapy.
Introduction
Liver carcinoma is a kind of malignant tumor originated from the hepatic parenchymal urinary epithelial system, accounting for 80%–90% of hepatic malignancies.1–3 The incidence of liver carcinoma is 2%–3% in adult malignant tumors, the rate of hepatic carcinoma in men and women is about 2:1, and it is frequently occurring in people between 50 and 70 years old.4–6 The etiology is not clear; the occurrence of liver carcinoma is related with genetics, smoking, obesity, and occupational contact.7–9
Owing to its minimally invasive feature, the laparoscopic technique has appeared as a widely accepted and standard surgical option for hepatic masses. 10 Compared with open surgery, laparoscopic partial hepatectomy (LPH) had some advantages, such as decreased postoperative pain, less blood loss, quicker recovery times, and lower cost. The indications of laparoscopic technique had been expanded into some complex cases, including hepatic masses with venous tumor thrombus. The second international consensus meeting of laparoscopic liver resection stated that major hepatectomy can be performed by expert centers, but more evidence is needed to support its role as a standard treatment for liver cancer.
Open partial hepatectomy (OPH) performed with the excision of a minimal tumor-free surgical margin or as simple enucleation was considered as the gold standard for the treatment of liver carcinoma.11–14 Besides, it was reported that hospital expense in OPH was less than that in LPH since supplies and ultrasonic knife are expensive medical instruments in LPH. 15 Because the complication of LPH, intraoperative knotting and suturing would take more time. This would make time of hepatic ischemia extended. Hence, OPH had better performance in hepatic ischemia time than LPH.
Since both methods had their own advantages and disadvantages, the comparison between LPH and OPH was imperative. Limited meta-analysis focused on the contrast between LPH and OPH in hepatic tumors. This study aimed to compare the safety, side effects, changes in hepatic function, and postoperative pain control between LPH and OPH in hepatic tumors.
Methods
Search strategy
To search out all of the relevant published citations, multiple electronic databases, including Pubmed, Springer, EMBASE, EMBASE, OVID, and China Journal Full-text Database, were applied without language restrictions. To maximize the search accuracy, the following MeSH terms were assembled with the Boolean operator “AND”: (1) laparoscopic partial hepatectomy OR LPH, (2) open partial hepatectomy OR OPH, and (3) liver carcinoma OR liver cancer-related articles with all publication statuses (published, unpublished, in press, and in progress) published from January 2000 to January 2016 about the pulmonary infection were systematically searched and reviewed. Two authors in our team searched the literature independently and examined the reference lists to obtain the additional relevant studies that are not identified.
Study selection
Two authors selected the citations independently and attentively in this study with the following inclusion criteria: (1) adult patients with liver carcinoma, (2) sample size >10, (3) a randomized control trial or controlled clinical trial study, (4) comparison of the LPH or OPH between patients with liver carcinoma, and (5) availability of full text. They screened the titles and abstracts of the articles identified and, subsequently, the full text of the studies that potentially met the criteria was obtained. These 2 investigators determined the included articles together, and disagreements were resolved by consultation with a third investigator if necessary.
Data extraction
After reading the full text of the articles, the characteristics from each study using a standard data extraction were extracted: the first author's name, year of publication, nation, recruitment time, age range of patients, gender distribution (men/women), sample size (LPH/OPH), follow-up period, and other parameters.
Statistical analysis
The meta-analyses were conducted with the software Review Manager 5.3 (The Cochrane Collaboration, 2011) to estimate the clinical efficacy of LPH and OPH in patients with liver carcinoma among selected articles. As continuous outcomes, standard mean difference (MD) with 95% confidence intervals (CIs) was performed. In discontinuous outcomes, odds ratio (OR) with 95% CIs was conducted. A P value <.05 was considered to be statistically significant. The heterogeneities in this study were assessed using the I2 index. We chose the random-effect model when the heterogeneity I2 statistic >50%; otherwise, the fixed-effect model was applied.
In addition, the quality of the studies was assessed with sensitivity analysis and bias analysis. Risk of bias table of the included studies was independently assessed according to the Cochrane Handbook for Systematic Reviews of Interventions by 2 members of our team. Also if any occurrence of poor agreement and no consensus could be achieved, a third investigator was the adjudicator.
Results
Search results
As shown in the flow diagram of Figure 1, 1327 relevant studies had been initially searched out, and with 1310 articles excluded for duplication, irrelevant studies, incomplete data, incomplete comparison, other diseases, and not a full text. Finally, 17 articles16–32 satisfied the inclusion criteria. Among these 17 articles, all 17 articles were published in English. The study selection process is detailed in Figure 1.
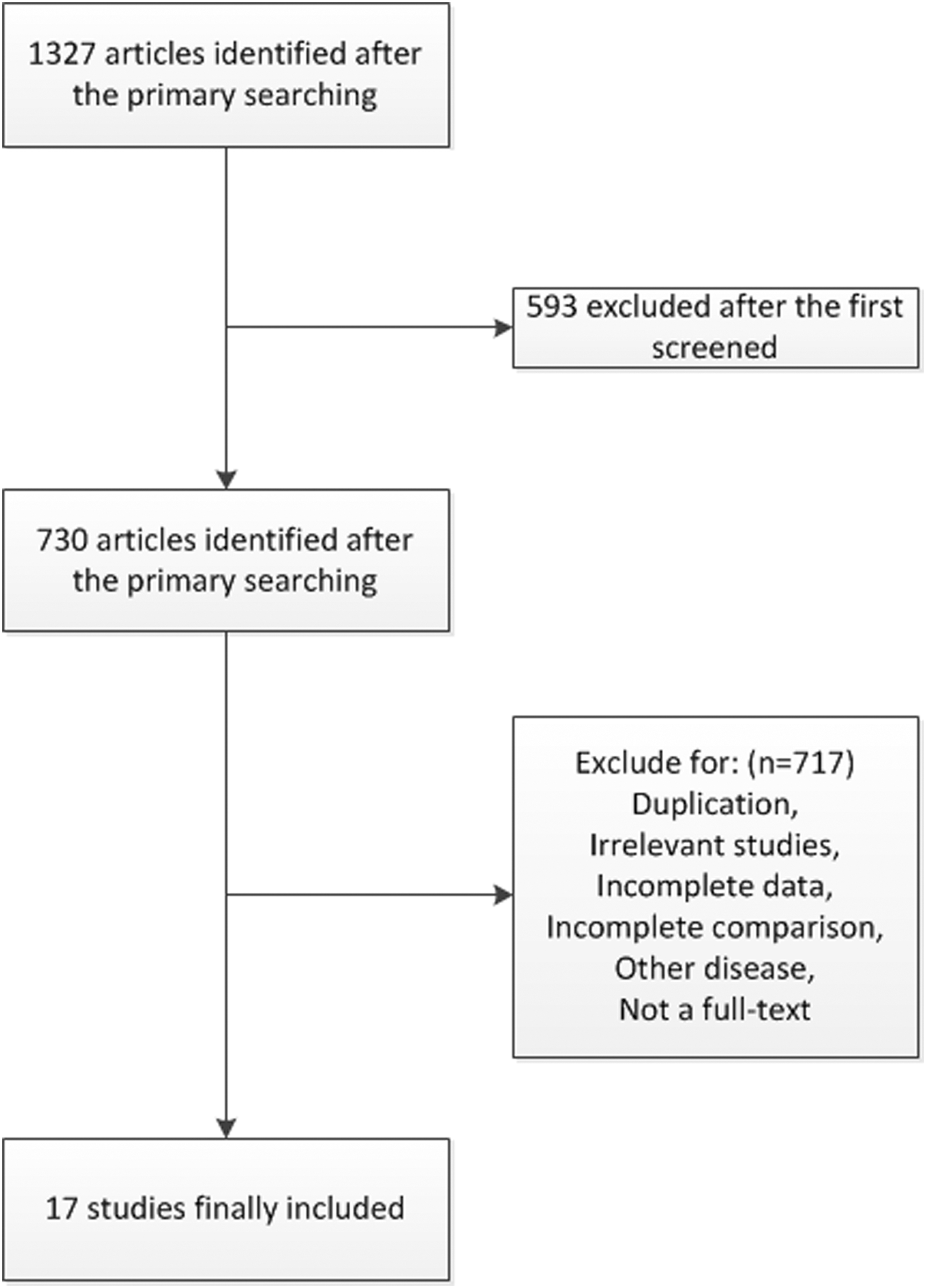
Flow diagram of the study selection.
Characteristics of included studies
Detailed characteristics of the included studies, including the first author's name, year of publication, nation, recruitment time, age range of patients, gender distribution (men/women), sample size (LPH/OPH), follow-up period, and other parameters, are presented in Table 1. All these studies were published from 2002 to 2017. The sample size ranged from 23 to 1800. Totally 1723 patients receiving LPH were included in these studies, and 2174 were patients receiving OPH.
Characteristics of Studies Included in the Meta-Analysis of Comparison of Laparoscopic Partial Hepatectomy and Open Partial Hepatectomy for the Treatment of Liver Cancer
LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Quality assessment
The bias table in the Review Manager 5.3 Tutorial was used to evaluate the risk of each study by applying the criteria of evaluating design-related bias. The quality of included studies was evaluated by the risk of bias table, and the evaluation of this study is shown in Figures 2 and 3. In the 17 articles, 1 trial showed problem in patient selection, 1 showed problem in detection bias, 1 showed problem in attrition bias, and 1 trial showed problem in the other bias. Overall, all the trials were out of risk.

Assessment of the quality of the included studies: low risk of bias (green hexagons), unclear risk of bias (blank hexagons), and high risk of bias (red hexagons).
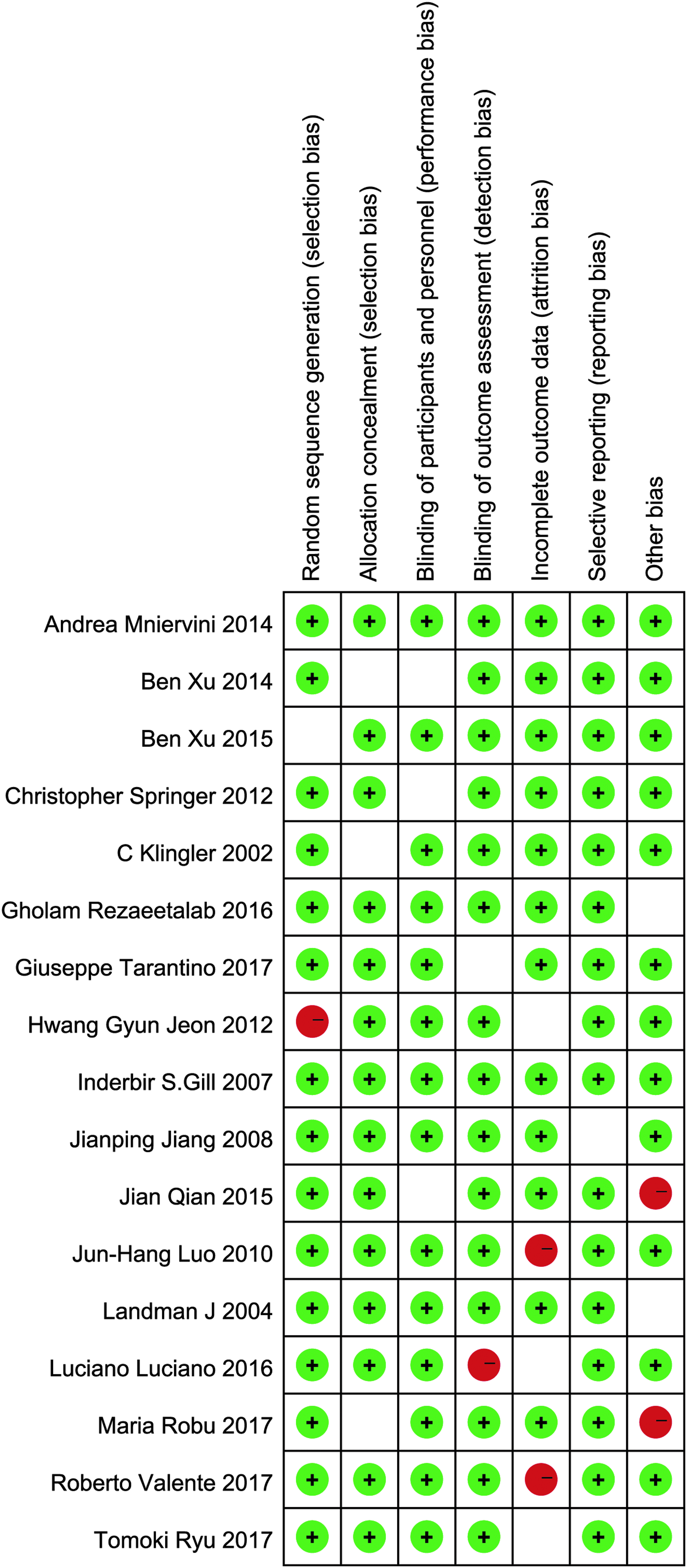
Quality assessment of included studies.
Results of meta-analysis
Meta-analysis about operating time between OPH and LPH
Twelve studies included involve in the comparison of operating time between LPH and OPH. The forest plot for operating time in different groups is shown in Figure 4. All these studies involved reported that the operating time between LPH and OPH groups were statistically insignificant. The overall result is shown in Figure 4 (MD = 4.00, 95% CI [−17.50 to 25.49], P = .72; P for heterogeneity <.00001, I2 = 99%).
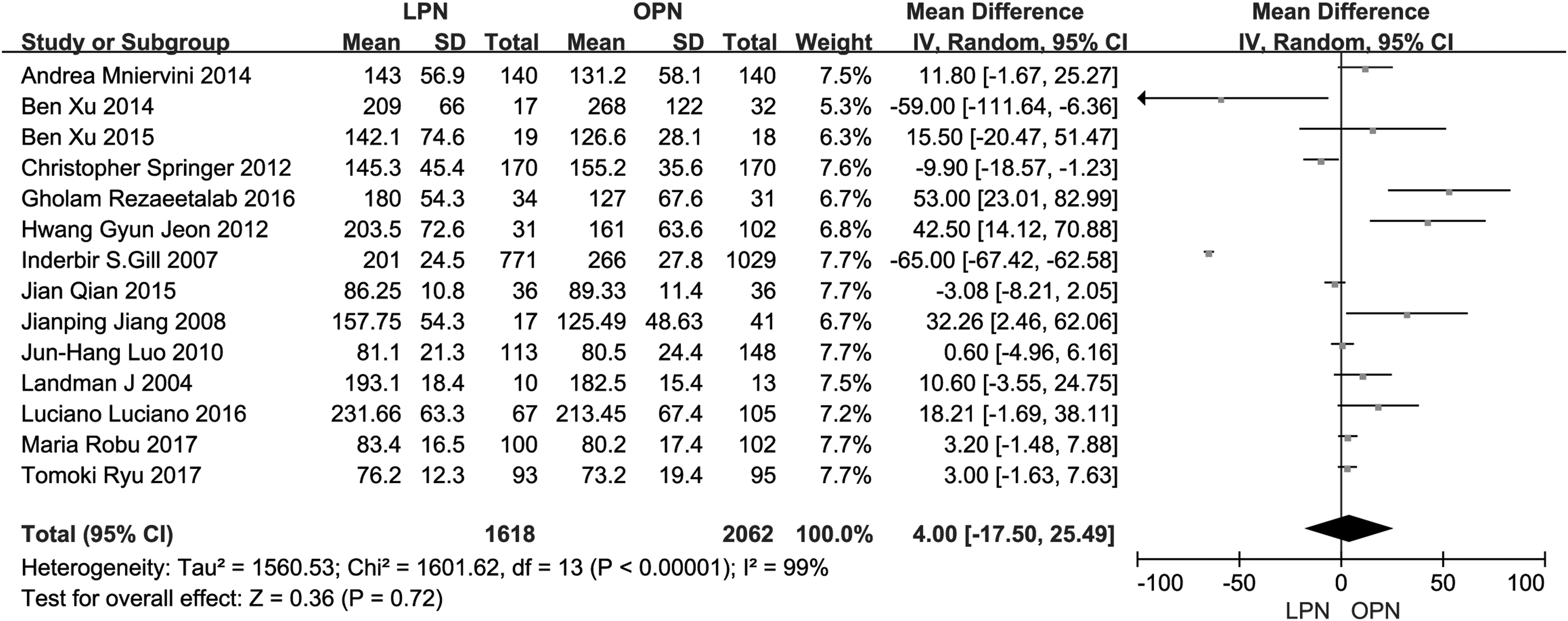
A forest plot for the comparison of operating time between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Meta-analysis about recurrence between OPH and LPH
Seven of 13 studies involved in the comparison of recurrence had showed the statistical difference (Fig. 5). The meta-analysis indicated that the recurrence in patients receiving OPH was higher than that of LPH group (OR = −20.11, 95% CI [−35.93 to −4.29], P = .01; P for heterogeneity <.00001, I2 = 100%).

A forest plot for the comparison of recurrence between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Meta-analysis about complication events between OPH and LPH
Eight of these 13 studies included involve in the comparison of satisfaction. The meta-analysis showed that the incidence of complication events occurred in patients in LPH group and that in OPH had no statistically significance (OR = 0.68, 95% CI [0.46 to 1.01], P = .05; P for heterogeneity = .34, I2 = 11%) (Fig. 6).
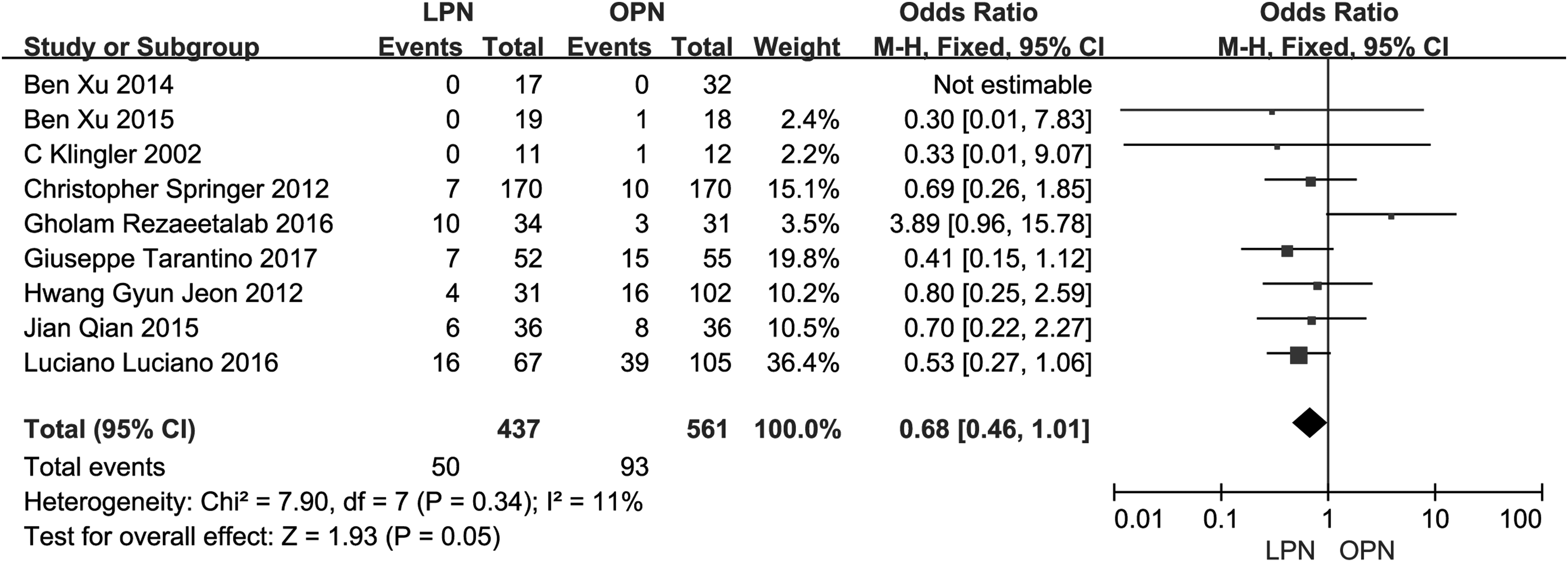
A forest plot for the comparison of complication events between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Meta-analysis about hospital days between OPH and LPH
Six of 13 included studies involve in the hospital days between LPH and OPH groups as shown in the forest plot (Fig. 7). The result of meta-analysis showed that the hospital days between LPH and OPH were significant (MD = −2.21, 95% CI [−2.53 to −1.88], P < .000001; P for heterogeneity = .03, I2 = 58%). The hospital days in OPH were much more than that in LPH.
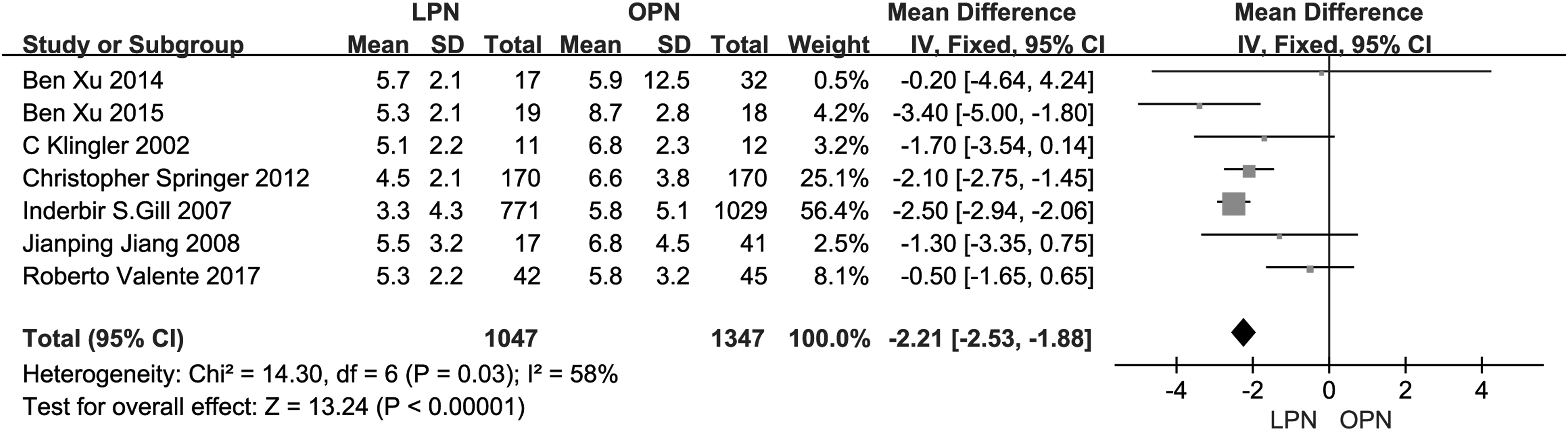
A forest plot for the comparison of hospital days between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Meta-analysis about blood loss between OPH and LPH
Among the 13 articles, there were 7 studies that reported the comparison of blood loss. The forest plot for the blood loss between LPH and OPH is shown in Figure 8. The meta-analysis indicated that the blood loss of OPH was much more than that of LPH (MD = −68.09, 95% CI [−85.07 to −51.11], P < .00001; P for heterogeneity = .13, I2 = 37%).
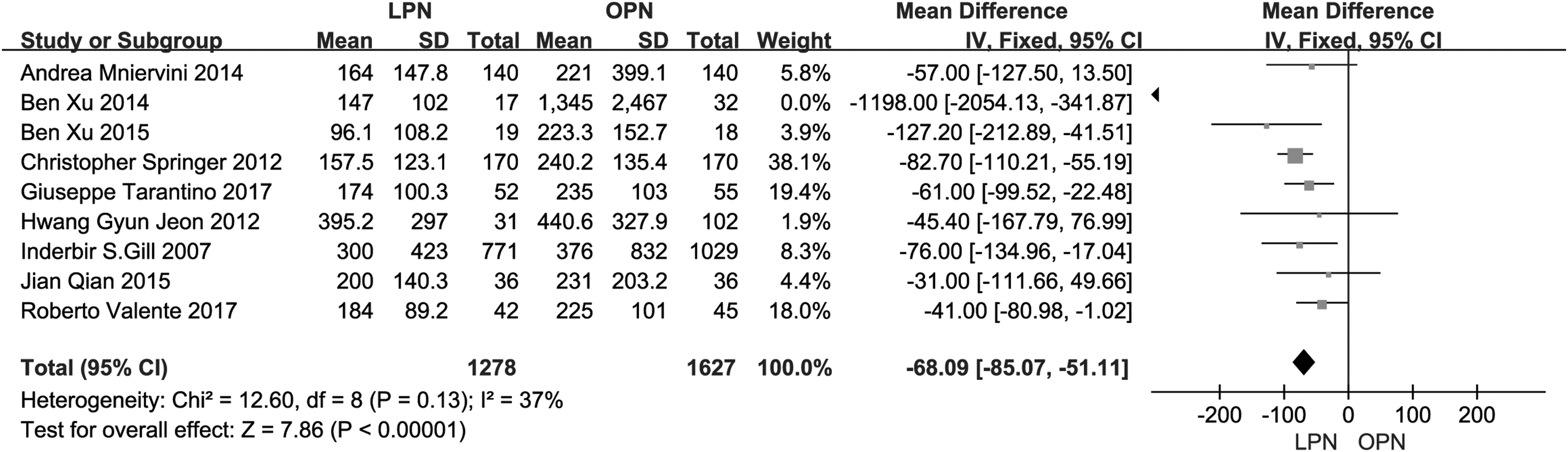
A forest plot for the comparison of blood loss between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Sensitivity analysis
According to the results of meta-analyses, the heterogeneities of operating time were very high (I2 ≥ 99%). As shown in Figure 9, the high heterogeneity of operating time was probably attributed to the different results in each study. When the article of Inderbir S.Gill was excluded, I2 changed from 99% to 74%.

A forest plot for the sensitivity analysis of operating time between LPH and OPH. LPH, laparoscopic partial hepatectomy; OPH, open partial hepatectomy.
Bias analysis
A funnel plot for operating time in LPH and OPH was performed. All the studies were included in the plot. The result showed that there existed some publication bias since the symmetrical characteristic of the funnel plot was not good (Fig. 10).

Begg's funnel plot of publication bias.
Discussion
The liver carcinoma is a kind of common malignant tumors. Radical hepatectomy is the main surgical treatment of localized liver carcinoma, which is recognized as the gold standard.32,33 Since a successful laparoscopic hepatectomy was reported for the first time, it was increasingly widely used. There was the trend of laparoscopic surgery to replace open surgery.
With the improvement of surgical methods, surgical techniques, and equipments, LPH had been widely applied for hepatic tumors.34,35 Multiple studies had demonstrated similar clinical and functional outcomes for minimally invasive and open approaches to partial hepatectomy.36–38 Laparoscopic surgery also offered the potential for enhanced cosmesis and reduced wound-related morbidity, particularly regarding incisional paresthesia, numbness, pain, flank bulge, and herniation. It was also reported that for liver cancer, traditional OPH had been replaced by LPH. However, open surgery was still required for liver tumor. Therefore, a meta-analysis for the comparison between LPH and OPH in treating liver tumor was significant.
There was no significant difference in operating time in these 2 therapies. The results of recurrence showed that this value in OPH was better than that in LPH, which indicated that the clinical efficacy of OPH was better than that of LPH to some extent. Maurette stated that LPH in patients had similar morbidity to open resections, and resection margins were not compromised because of laparoscopy. 39
The complication events between LPH and OPH had no difference according to the meta-analysis. In hospital days and blood loss, the mean value in these two aspects of LPH was less than OPH and this demonstrated that LPH was a quicker recovery and less harmful therapy. Zeng reported that LPH had many benefits, including better cosmetic effect, less pain, less blood loss, shorter hospital stay, and faster recovery, compared with OPH. 40 Overall, OPH as a gold standard for treating hepatic tumor had a better clinical efficacy than LPH, whereas LPH was a more convenient and less invasive method.
Some limitations still existed in this research. First, the details of complication events in both therapies were not analyzed, and it could be evaluated in the future. Second, the included articles could cover more researches, which could be conducted in future research.
Footnotes
Disclosure Statement
No competing financial interests exist.