
Abstract
Abstract
Purpose:
To report the long-term results of endoluminal sharp recanalization of occluded inferior vena cava (IVC) in patients with the Budd-Chiari syndrome (BCS).
Patients and Methods:
Seventy-two consecutive patients with BCS and IVC occlusion underwent endoluminal recanalization of the IVC occlusion during a 6-year period. BCS with occlusive IVC was detected by reviewing patient history and color Doppler ultrasonography. Data on technical success, morbidity, mortality, complications, and color Doppler sonographic outcome were collected and analyzed.
Results:
Seventy-seven recanalizations were performed in 72 patients. Technical success (patent IVC with good blood flow) was achieved in 70 (97.4%) patients. No perioperative death was observed. Six complications were found during recanalization, and 10 complications were found for total interventional procedures. The complication rates were 7.8% and 7.3% for recanalization and total procedure, respectively. Bleeding of access veins was the most common complication, and 2 patients showed slight rupture of IVC. The postoperative IVC diameter and blood speed of IVC increased significantly. Fifty-seven patients (79.2%) were clinical cured, and 2 patients (2.8%) showed no improvement. The 1-year, 3-year, and 5-year primary patency rates were 92.5%, 86.8%, and 77.3%, respectively. The second patency rates were 100.0%, 97.8%, and 91.8% for 1, 3, and 5 years, respectively. There were 2 deaths during follow-up.
Conclusion:
Endoluminal sharp recanalization of occluded IVC in patients with BCS is safe and effective with good long-term outcomes.
Introduction
B
Patients and Methods
Clinic data
This retrospective study was approved by the university committee; informed consents were obtained from all enrolled patients. Between April 2010 and August 2016, 72 consecutive BCS patients were referred to our department for endoluminal recanalization of IVC. BCS with occlusive IVC were detected by reviewing patient's history, 64-slice CT scanning (Philips Brilliance, Fig. 1), and color Doppler ultrasonography (GE Vivid 7, 3.5–5.0 MHz). Patients with severe liver function failure, severe coagulation dysfunction, or terminal hepatic carcinoma with expectancy less than 3 months were excluded from this study. The patient's characteristics and data of procedure were recorded and analyzed.
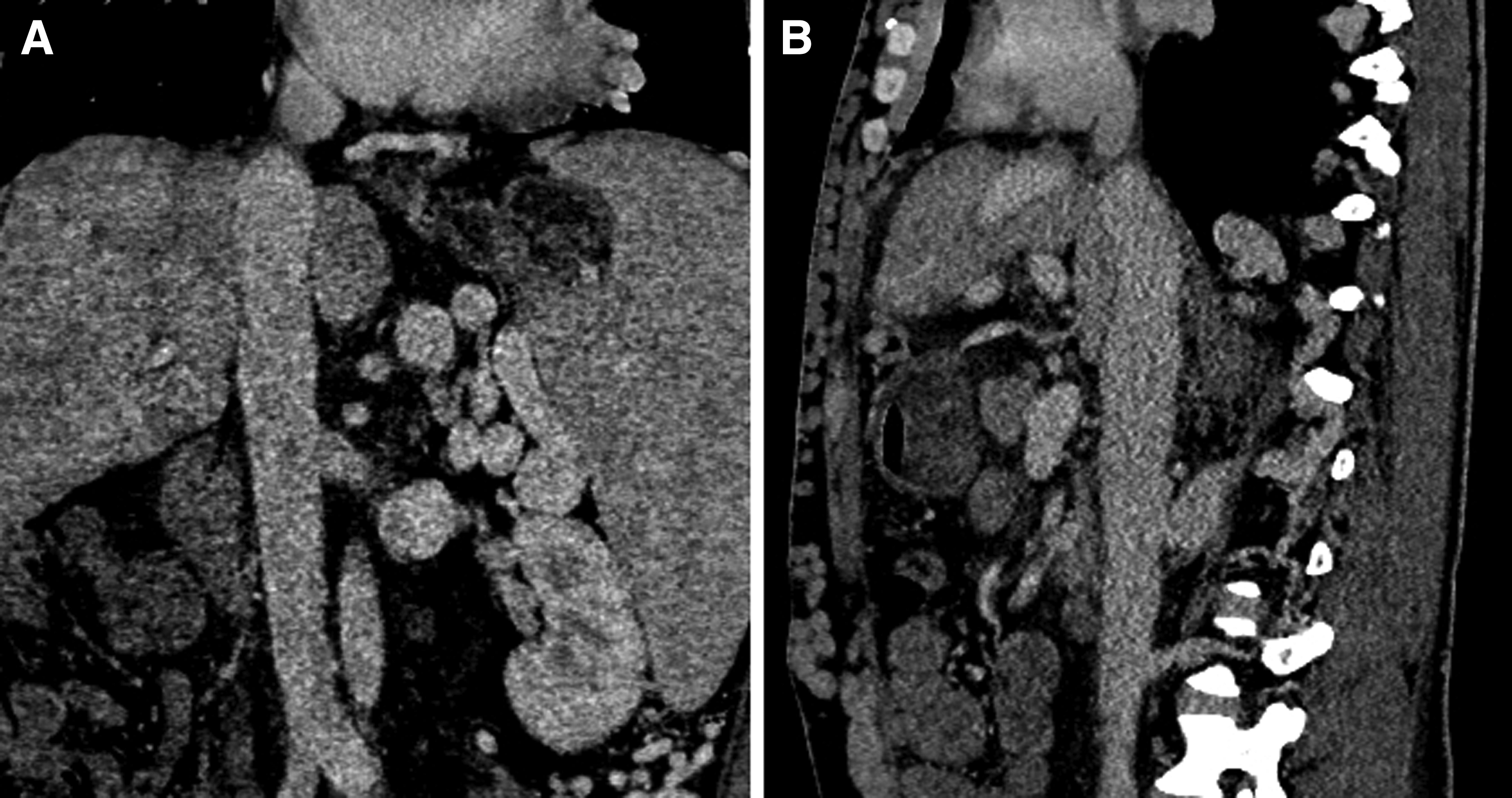
Preoperative examination by abdominal CT. Membranous occlusion of proximal IVC, collateral veins, and heterogenous contrast enhancement of hepatic parenchyma and splenomegaly were clearly shown in coronal
Endoluminal recanalization for occlusive IVC
IVC was accessed via right femoral vein (FV) puncture, otherwise, the left FV or right jugular vein was accessed. A 5F straight catheter with multiple side holes was introduced into IVC for angiography. A J-type blunt needle and rigid end of a 0.035" Terumo guide wire were used for IVC recanalization under fluorescence guidance. The blunt needle and a 5F Headhunter catheter (Cook) were introduced into the distal part of the occlusion. The needle angle was adjusted toward the right atrium at the proximal part of the occlusion (Fig. 2). A balloon catheter (Cook) was inserted via 0.035 inch stiff guide wire (Amplatz Super Stiff; Boston Scientific, MA). Predilation was performed via 8–14 mm balloon catheter.10,19 All balloon angioplasties were performed 3 times of expansion, each expansion lasted about 30 seconds. Second IVC angiography was performed to show the effect of dilation (Fig. 3).
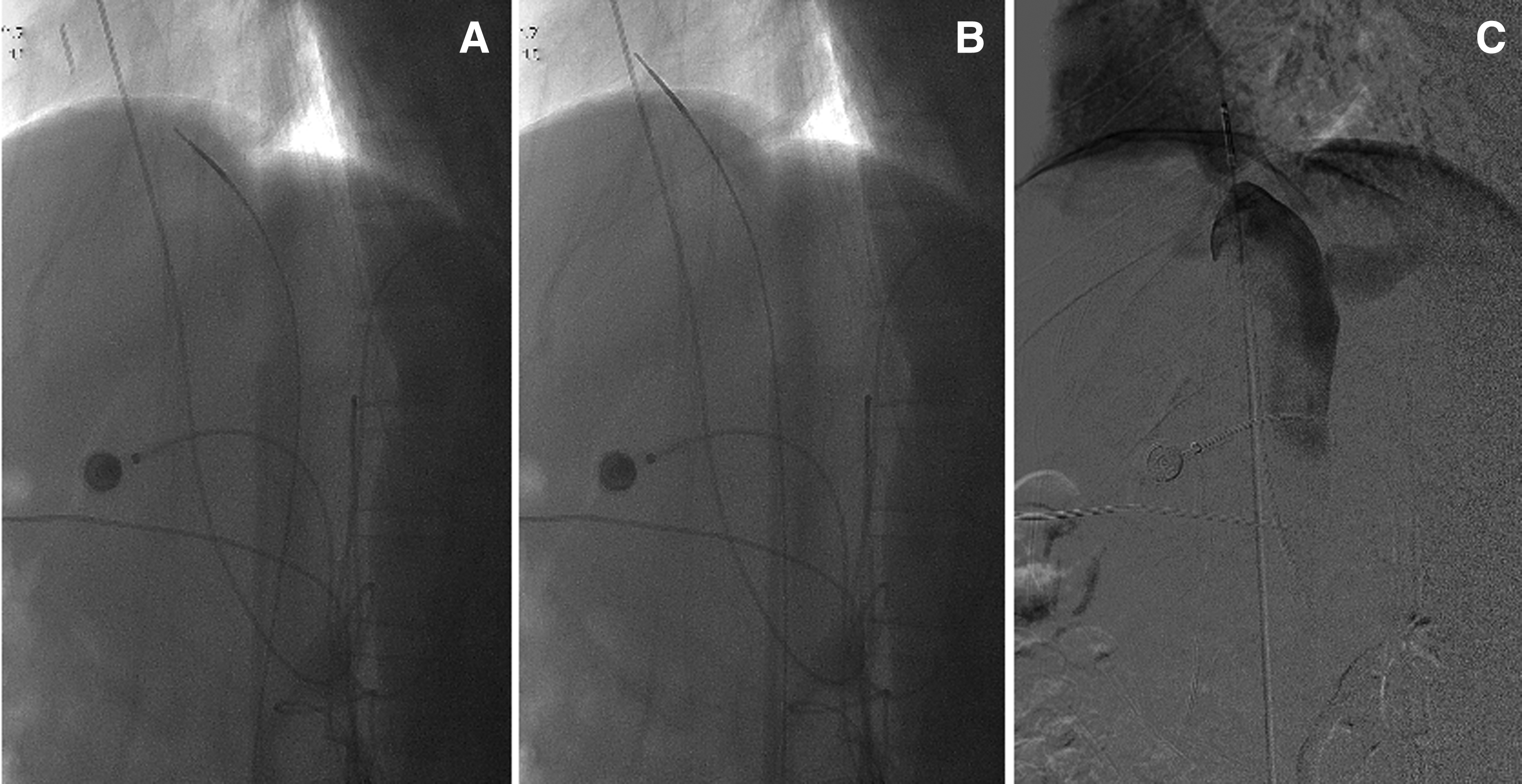
Endoluminal recanalization.
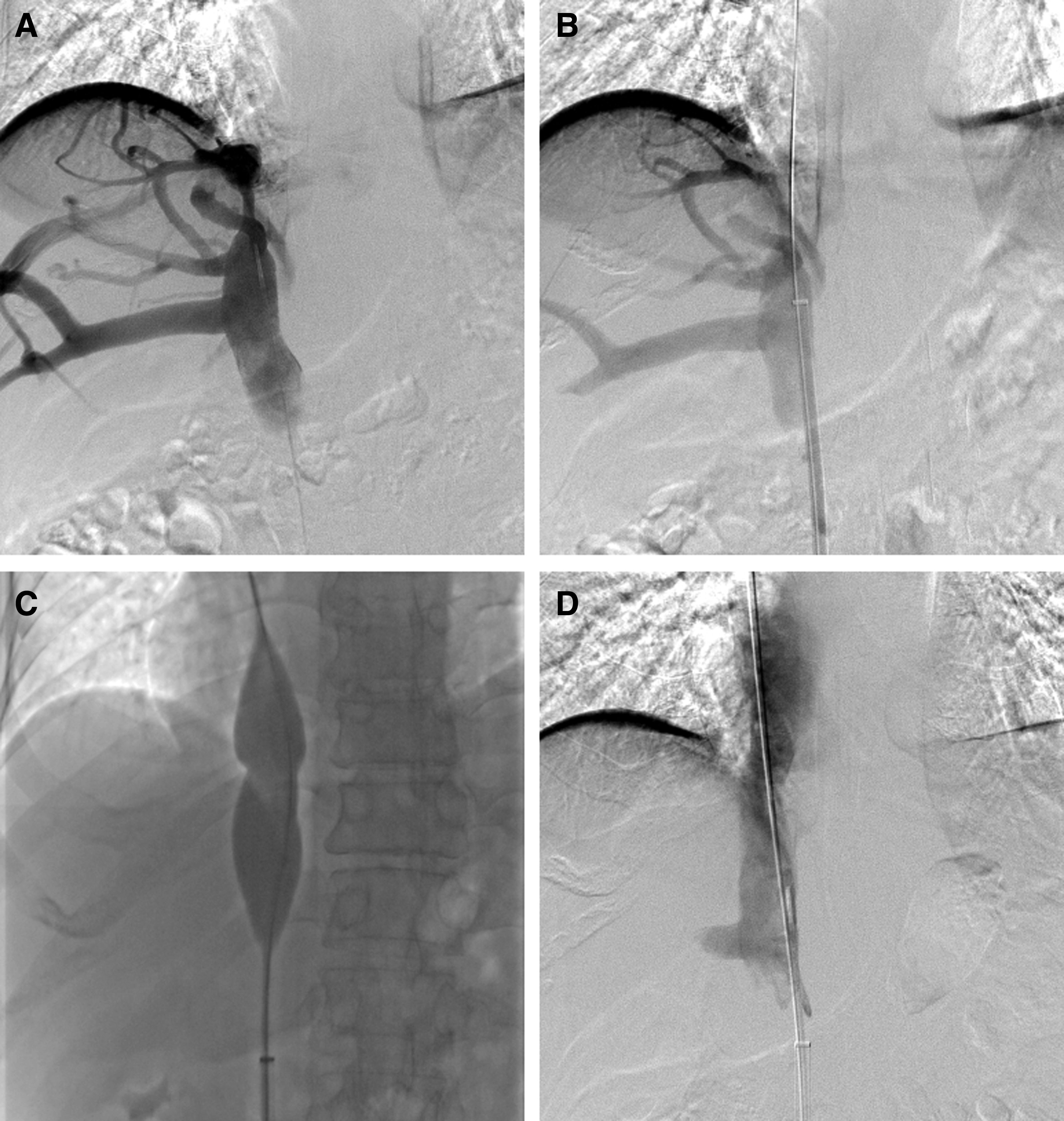
Balloon angioplasty.
Related interventional procedures
For patients with fresh thrombosis in IVC, 5F pig tail catheter was used for agitation thrombolysis or catheter directed thrombolysis according to previous reports.9,20 A retrieval stent were used for patients with IVC thrombolysis. 21 Permanent stent was implanted for patients with remained occlusion or stenosis in IVC after thrombolysis or repeated PTA.21–23 Percutaneous transhepatic variceal embolization was performed for patients with gastrointestinal bleeding.
Postoperative medicine
After procedure, 5000 U of low-molecular weight heparin was subcutaneously injected every 12 hours for 3 to 5 days. Patients underwent anticoagulation therapy by oral take of warfarin from the second day for 0.5–1 year, to maintain an international normalized ratio between 2 and 3. Aspirin (100 mg/day) and dipyridamole (225 mg/day) were used for patients with warfarin resistance.
Follow-up evaluation and definition
All patients were followed up after 1 and 3 months, and every 6 months thereafter (Fig. 4). Color Doppler ultrasonography as well as clinical/laboratory examinations were performed during follow-up. Data on technical success, morbidity, mortality, complications, and color Doppler sonographic outcome were collected and analyzed. Primary patency was defined as the interval between initial PTA and first appearance of stenosis or obstruction that necessitated PTA. Secondary patency was defined as the total time from the first PTA with the contribution of all subsequent nonsurgical procedure until the final follow-up, open surgery, or death. Patients were clinically cured if the IVC was patent with no symptom or signs.
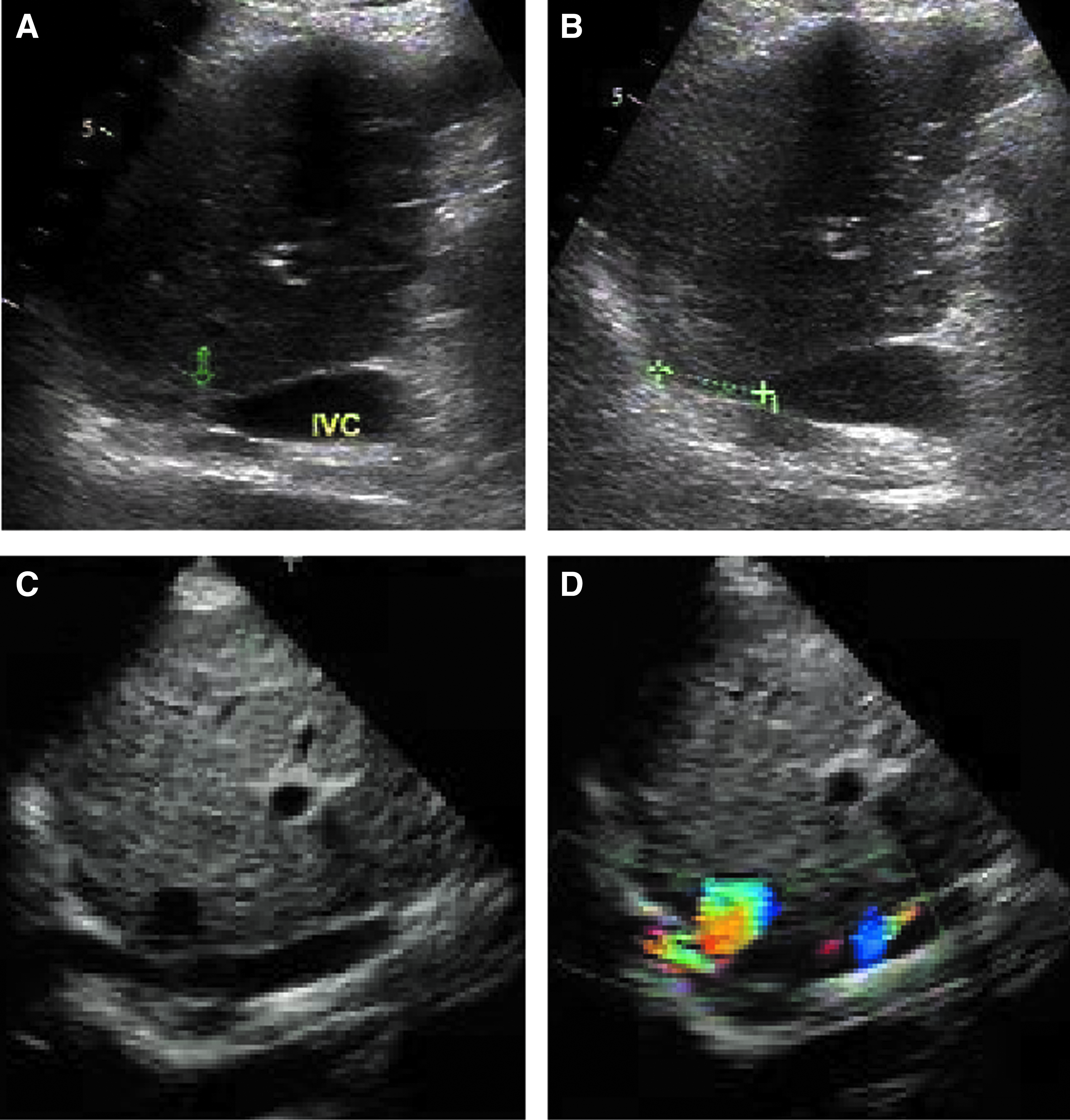
Color Doppler ultrasonography. Segmental occlusion of proximal IVC was clearly shown
Statistical analyses
Data are the mean ± SE. Student t-test and ANOVA were used for analysis of quantitative data. Qualitative data were reported as numbers and percentages, and analyzed by chi-square test. Survival and patency rates were compared by using Kaplan–Meier curves. Statistical analyses were carried out using Prism 5.0 (GraphPad Software, Inc., SanDiego, CA).
Results
Patient characteristics
A total of 72 BCS patients with occlusive IVC (43 men; mean age 47.6 ± 1.3 years, range 22–76 years) were included in this study. There were 21 patients (29.2%) with duration of less than 1 year, and 26 patients (36.1%) had a chronic duration of more than 10 years. Sixty-nine cases (95.8%) had combined HV and IVC involvement, and membranous obstruction in 31 (43.1%) and segmental obstruction in 41 cases (56.9%). Eighteen patients (25.0%) showed IVC thrombosis associated with IVC occlusion. Thirty-eight patients (52.8%) showed the liver function of Child Pugh A (Table 1). Lower extremity edema/pain and abdominal distension/abdominal pain are the most common symptoms and signs before recanalization.
HV, hepatic vein; IVC, inferior vena cava.
Recanalization
IVC recanalization procedure was performed 77 times in 72 patients with a 97.4% technical success rate. Right FV was the routine access vein for recanalization, right internal jugular vein (IJV) was accessed if recanalization failed via FV or occlusive FV. In this study, 42 times (54.5%) of recanalization were performed via isolated right FV access. The J-type blunt needle was the most common used instrument for recanalization. Antegrade recanalization from FV was the first choice, and 29 times (37.7%) of retrograde recanalization from IJV were performed, including 8 times of initial failures of antegrade recanalization. Predilation with 12–14F of long sheath was performed 42 times, of which, 24 times underwent additional predilation by small balloon. A total of 91 times of large balloon angioplasty were performed with balloon catheter of 20–30 mm in diameter (Table 2).
FV, femoral vein; HV, hepatic vein; IJV, internal jugular vein; IVC, inferior vena cava.
Related interventional procedures
Except for IVC angioplasty, each of two times balloon angioplasty was performed for occlusion or stenosis lesion in HV and right iliac-femoral veins. Catheter directed thrombolysis was performed 12 times for patients with fresh thrombus in IVC, including 7 times combined with agitation thrombolysis. Seven retrieval stents (30 × 108 mm) were successfully implanted for BCS with IVC thrombus; all were removed after disappearance of thrombus. Eleven permanent Z stents (diameter 30 mm, length 52–80 mm) were successfully implanted for patients with stenotic IVC after repeated balloon angioplasty. Three patients underwent percutaneous transhepatic variceal embolization due to gastrointestinal hemorrhage, including 2 patients who were performed during transjugular intrahepatic portosystemic stent-shunt.
Perioperative complications
No perioperative death was observed. Six complications were found during recanalization, and 10 complications were found for total interventional procedures. The complication rates were 7.8% and 7.3% for recanalization and total procedure, respectively. Bleeding of access veins was the most common complication, and was successfully treated with pressure compression. One patient showed transient loss of consciousness during large balloon dilation following successful recanalization, but recovered to normalcy 3 minutes later, after that, all procedures were ceased without treatment. Two patients showed slight rupture of IVC; one patient showed contrast agent within the pericardium during recanalization and resulted in failure of recanalization without pericardial tamponade, and the other happened during balloon angioplasty, a small amount of contrast agent was exuded to the periphery of the gastric antrum; the dilated balloon was used to stop the hemostasis, and no contrast agent was exuded during second angiography after 10 minutes (Table 2).
Size changes of IVC
The preoperative length of occlusive IVC was 40.3 ± 5.3 mm, and decreased significantly to 8.5 ± 1.9 mm after procedure (P < .0001). The preoperative diameter of lesion IVC was 3.7 ± 0.3 mm, which increased to 7.6 ± 0.4 mm after procedure (P < .0001). Diameter of relative normal IVC and distal IVC did not change significantly (Table 3). IVC pressure decreased significantly after procedure (P = .0065), and blood speed of IVC increased significantly after dilation compared to preoperative data (P < .0001).
Others included 1 gingival bleeding, 2 nasal bleeding, 2 scrotum edema, 1 panic, chest tightness, 2 leukocyte and thrombocytopenia, and 1 cough.
IVC, inferior vena cava.
Clinical efficacy evaluation and follow-up
Lower extremity edema/pain, abdominal distension/pain, and ascites were obviously relieved after procedure (P < .0001). All 7 patients with gastrointestinal bleeding were successfully treated (P = .0134), and varicose veins in lower limbs/abdomen were also relieved after procedure (P = .0400). Lower limbs pigmentation did not improve during follow-up. Four cases were lost in follow-up, with a lost rate of 5.6%. Fifty-seven patients (79.2%) were clinically cured, and 2 patients (2.8%) showed no improvement. The 1-year, 3-year, and 5-year primary patency rates were 92.5%, 86.8%, and 77.3%, respectively. The second patency rate was significantly higher than primary patency rate, with rates of 100.0%, 97.8%, and 91.8% for 1, 3, and 5 years, respectively. There were 2 deaths during follow-up. One patient died of liver failure 59.2 months after operation; the other died of advanced liver cancer 18.3 months later. The 1-year, 3-year, and 5-year survival rates were 100.0%, 98.2%, and 91.2%, respectively (Fig. 5).

Patency rate and survival rate. The second patency rates were 100.0%, 97.8%, and 91.8% for 1, 3, and 5 years, which was significantly higher than primary patency rate. The 1-year, 3-year, and 5-year survival rates were 100.0%, 98.2%, and 91.2%, respectively.
Discussions
Among treatment options for BCS,4–7 PTA has become the first choice for BCS due to membranous IVC obstruction5,8–17 due to its high success rate and less complication. Eguchi et al. 24 first reported balloon angioplasty for BCS patient due to IVC occlusion, which opened up a new therapeutic approach. However, routine recanalization sometimes may fail for patients with long-segment obstruction of IVC, and blunt needle is needed for those patients. Few studies specifically reported the technology outcomes of IVC sharp recanalization by blunt needle.
Xu et al. 18 used J-type Brockenbrough needle (Cook, Inc., Bloomington) for recanalization obstruction of IVC and HVs, and 2 of 103 patients failed in recanalization of IVC, with a success rate of 98.1%. Ding et al. 9 used a steel needle (Cook, Inc.) for membrane recanalization of IVC. However, there was no detail description and technology outcome of bunt needle recanalization in above studies. Our study indicated a technology success rate of 97.4%, and only 2 patients (2.8%) showed no improvement. The 5-year second patency rate and survival rate were 91.8% and 91.2%. The safety and complication was another issue. The complication rates were 7.8% and 7.3% for recanalization and total procedure, respectively. No perioperative death was observed. Bleeding of access veins was the most common complication, and 2 patients showed slight rupture of IVC during sharp recanalization and balloon angioplasty.
Besides, various treatments were used to improve the clinical efficacy in this study, such as thrombolysis, retrieval stent, and permanent stent. Thrombolysis was used for IVC fresh thrombus.9,20 Retrieval stent was used to compress IVC thrombus and to prevent pulmonary embolism,21–23 and permanent stent was used for recurrent BCS. 25 In conclusion, endoluminal recanalization of occluded IVC in patients with BCS is safe and effective with good long-term outcomes.
Footnotes
Acknowledgments
This work is supported by the National Natural Science Foundation of China (Grant No. 81501569).
Disclosure Statement
No competing financial interests exist.