
Abstract
Abstract
The vertical sleeve gastrectomy is a bariatric procedure that was originally described as the initial step in the biliopancreatic diversion. It demonstrated effectiveness in weight loss as a single procedure, and the laparoscopic vertical sleeve gastrectomy, as a stand-alone procedure, is now the most commonly performed bariatric surgery worldwide. Due to its relative technical ease and long-term data that have established its durability in treating obesity and its related comorbid conditions, the sleeve gastrectomy has grown in popularity among patients and surgeons. While there are variations in the technical aspects of performing a laparoscopic sleeve gastrectomy, key steps must be undertaken to produce safe and effective outcomes. This article reviews the indications for bariatric surgery, patient selection, surgical technique and tips, perioperative care and complications after sleeve gastrectomy.
Introduction
T
Over time, laparoscopic sleeve gastrectomy (LSG) has been adapted to be a stand-alone weight-loss procedure. It is now the most commonly performed bariatric procedure in the world. 7 Long-term data have demonstrated its similar effectiveness in weight loss and resolution of comorbidities, as well as its mortality and morbidity rates, compared with the Roux-en-Y gastric bypass, the recognized “gold standard” for bariatric surgery. 8
Patient Selection
The qualifications for bariatric surgery, as stated by the National Institute of Health (NIH) and the American Society for Metabolic and Bariatric Surgery (ASMBS), include the following:
Age 18–64 years. Body mass index (BMI) ≥40 kg/m2. BMI ≥35 kg/m2 and at least one obesity-related medical comorbidity, such as type-II diabetes mellitus, hypertension, obstructive sleep apnea (OSA), nonalcoholic fatty liver disease, osteoarthritis, lipid abnormalities, gastrointestinal disorders, or heart disease. Inability to achieve a healthy weight loss sustained for a period of time with prior weight-loss efforts.
It is also recommended that patients seek a board-certified surgeon who has completed specialized training in bariatric surgery and who works at a center with multidisciplinary expertise.
All patients considering bariatric surgery should undergo an adequate preoperative evaluation and workup. In 2013, the American Association of Clinical Endocrinologists (AACE), The Obesity Society (TOS), and the ASMBS released an update to their original 2008 guidelines for perioperative support of the bariatric surgery patient. In addition to the routine complete history and physical and surgical risk assessment, essential elements to address for bariatric patients include the following: (1) evaluation and optimization of medical comorbidities, psychosocial and behavioral assessment; (2) consultation with a dietician and/or nutritionist; and (3) thorough education and informed consent regarding the various bariatric procedures and postoperative expectations, such as need for long-term follow-up and lifelong vitamin supplementation. Other key factors to consider are smoking cessation, fertility in female patients, and preoperative weight loss to reduce liver mass. 9
An area of controversy is the need for evaluation of gastroesophageal reflux before sleeve gastrectomy. LSG may not be the best option for patients who have significant gastroesophageal reflux disease (GERD) or Barrett's esophagus. Gastric bypass has long been recognized as the preferred antireflux procedure among bariatric operations. Sleeve gastrectomy has shown conflicting results in regard to postoperative antireflux effect utilizing both objective and subjective testing. While some studies have shown GERD improvement after LSG, 10 others have shown progressive or de novo postoperative reflux in some patients. 11 Therefore, the use of sleeve gastrectomy in GERD patients remains controversial, as does the need for preoperative screening. Some experts have suggested that the lack of clinical symptoms of GERD is insufficient to recommend a sleeve to this patient population, and that endoscopy and pH studies should be performed to rule out the presence of GERD. 7 This remains a highly debated topic with no current consensus.
Another patient group that must receive careful evaluation and counseling regarding sleeve gastrectomy and Roux-en-Y gastric bypass includes patients with type-II diabetes. Aminian et al. constructed a scoring system, the Individualized Metabolic Surgery Score, to categorize the severity of a patient's type-II diabetes into three stages, which could then be used to help guide evidence-based procedure selection. The authors showed that both the sleeve gastrectomy and gastric bypass demonstrated equal efficacy in improvement of diabetes in the mild and severe groups; however, in the intermediate group, gastric bypass was more effective in improving diabetes than the sleeve, and hence is the procedure of choice for those patients. 12
Selection between bariatric procedures remains largely driven by the patient, although the surgeon must help guide the patient in making a choice that will maximally benefit him or her. Considerations such as invasiveness of the procedure, long-term complications, medical comorbidities, and expected amount of weight loss should be taken into account. One of the main advantages of the sleeve gastrectomy is its technical simplicity relative to the gastric bypass, which creates a shorter operative time. This can be beneficial for high-risk surgical patients. Factors such as prior abdominal surgeries, visceral fat burden, and abdominal wall compliance may also play a role in the ability to safely perform a gastric bypass, thereby making the sleeve gastrectomy a safer alternative.
Outcomes
Bariatric surgery outcomes are characterized by amount of excess weight loss (EWL) and improvement or resolution of obesity-related comorbidities. Excess weight is defined as ideal body weight subtracted from actual body weight. After sleeve gastrectomy, the average expected EWL ranges from 50% to 60%. This is slightly lower relative to the gastric bypass and the duodenal switch, which produce, respectively, around 70% and 80% EWL. 13
Through weight loss and changes in metabolic and hormonal activity, bariatric surgery leads to improvement or resolution of obesity-related comorbidities such as type-II diabetes, hypertension, and OSA. Sleeve gastrectomy has produced comparable comorbidity improvements with gastric bypass. Although it was originally thought to be a purely restrictive procedure, multiple studies have demonstrated that sleeve gastrectomy also affects weight loss through other mechanisms, such as changes in gastrointestinal motility, hormonal mechanisms, and metabolic activity. 14
Technique and Key Steps
While there are variations in the technical aspects of the LSG, there are key steps that should be undertaken. The first step is a complete mobilization of the greater curvature of the stomach extending proximally to the angle of His. Following exposure of the left diaphragmatic crus and adequate clearance of the posterior stomach, a vertical gastrectomy is started at 4–6 cm proximal to the pylorus with creation of a tubularized stomach measuring 34–40 French in diameter with care to not narrow the incisura, cause spiralization of the neostomach, or leave excessive fundus. The following describes the technique utilized at the authors' institution.
Routine preoperative measures are taken, including administration of prophylactic antibiotics and subcutaneous heparin or lovenox, and placement of sequential compression devices. Patients are positioned supine on the operating room table with both arms abducted and pressure points well padded. Footboards are optional. A urinary catheter is used selectively based on the expected length of the procedure. An orogastric tube should be placed to decompress the stomach before starting the surgery. The operating surgeon stands on the patient's right, whereas the first assistant stands on the patient's left (Fig. 1).

The patient is positioned supine on the operating room table with both arms abducted. The surgeon stands to the patient's right. The first assistant stands at the patient's left.
In most cases, pneumoperitoneum is achieved using the Veress technique in the left upper quadrant. The abdomen is insufflated to 15 mmHg. Five ports are placed (Fig. 2). The first is a 15-mm port 20 cm below the xiphoid in the supraumbilical midline. We use a 15-mm port to permit passage of the Medtronic EndoGIA™ black staple load; the remainder of the staple cartridges fit through a 12-mm port. An operative laparoscope is introduced, and the abdomen is inspected to rule out injury from the Veress and any other anatomic abnormalities. The second is a 5- or 12-mm port 15 cm down the left rectus for the surgeon's right hand. These two ports alternate between working and camera ports. A 5-mm port, to be used by the first assistant for retraction, is placed in the left lateral subcostal location. A 5-mm port is placed laterally along the right costal margin for the liver retractor, and a final 5-mm working port is placed in the right epigastrium for the surgeon's left hand. We use an articulating liver retractor positioned underneath the left lobe of the liver to expose the entire stomach and diaphragmatic hiatus. It can be secured to the drapes or to a retractor post attached to the operating table. Alternatively, a Nathanson liver retractor can be used from a subxiphoid position.
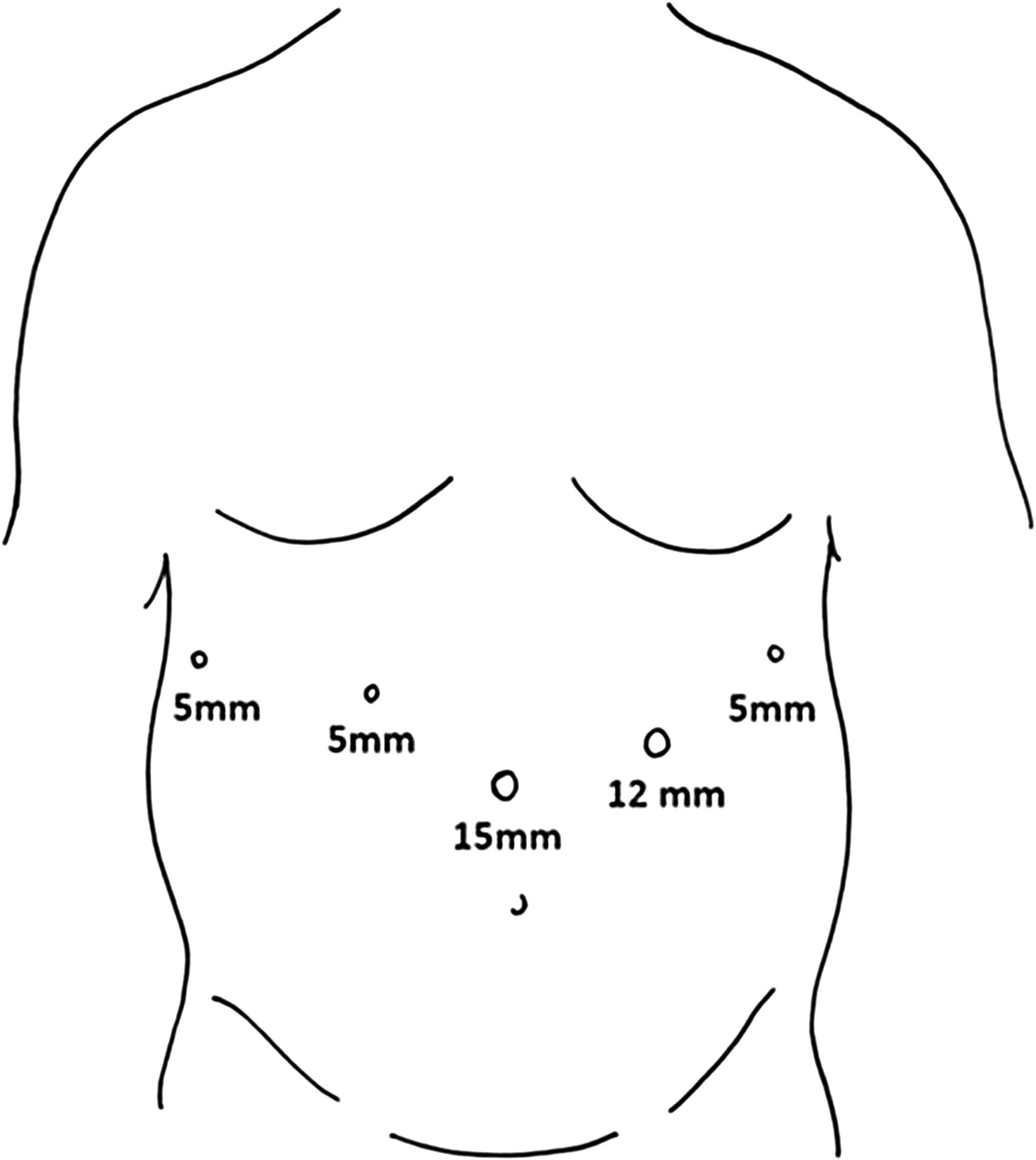
Positions and sizes of ports. The midline 15-mm port is placed 20 cm down from the xiphoid process. We use this as both a camera port and a stapling port. We use an EndoGIA™ black staple load for our first staple, and this must be inserted through a 15-mm sized port. The most lateral right port is used for an articulating liver retractor. The right mid-abdomen and left mid-abdomen ports are working ports. The left mid-abdomen port is also used for the camera during stapling. The left lateral port is used by the first assistant.
The operating table is placed in steep reverse Trendelenburg position to allow the transverse colon and small intestine to fall toward the pelvis. The pylorus is identified, and the proposed site of transection is marked 4–6 cm proximal to the pylorus. Dissection is initiated along the greater curvature at the mid-body of the stomach. The lesser sac is entered using an energy device and the omental attachments, gastroepiploics, and short gastric vessels to the greater curvature of the stomach are divided. The entire greater curve of the stomach is mobilized up to the angle of His including all posterior peripancreatic attachments, and the left crus of the diaphragm is exposed. Care should be taken during this portion of the procedure to identify and preserve the splenic vessels as well as to avoid excessive traction on the spleen. If a hiatal hernia is identified, it should be repaired. In these cases, we perform circumferential dissection of the esophagus until 3 cm of tension-free intraabdominal esophagus is mobilized. Hiatal closure is performed with posterior interrupted pledgeted sutures, using zero polyester sutures. The direction of the omental dissection is then reversed, and the greater curvature is mobilized distally to the previously identified point 4–6 cm proximal to the pylorus.
The orogastric tube and any other foreign devices within the stomach and esophagus are removed. A nonbolstered linear stapler is introduced through the 15-mm supraumbilical port and positioned obliquely across the greater curvature at the previously identified point 4–5 cm proximal to the pylorus. The first staple firing utilizes a taller staple height range (4.0–5.0 mm), then the remainder return to our typical gastric height (3.0–4.0 mm). The stapler stays parallel to the lesser curvature, and we ensure that the gastric outlet is not narrowed (Fig. 3). A 34–40 French blunt-tipped bougie dilator is then passed through the mouth, esophagus, and proximal stomach, and positioned along the lesser curvature inside the first staple line. Successive firings of the linear stapler are then taken along the dilator vertically up the stomach to 2 cm lateral to the angle of His and away from the gastroesophageal junction. It is crucial to avoid narrowing the incisura as well as to ensure that the anterior and posterior surfaces of the stomach are properly apposed during stapling to prevent causing a corkscrew effect on the sleeve and to ensure adequate resection of the fundus. Approximately 70%–80% of the stomach is resected. The dilator is then removed, and hemostasis is ensured. No additional staple line reinforcement is performed (Fig. 4).

Placement of the first staple load 4–6 cm from proximal to the pylorus. Care must be taken to avoid narrowing the gastric outlet.

Completed vertical sleeve gastrectomy. A 34–40 French blunt-tipped bougie dilator is used to size the sleeve.
If there is any concern for the potential for torsion or volvulus, we affix the mobilized gastrocolic omentum to the lateral side of the sleeve with two to four interrupted absorbable sutures. The resected stomach is then removed under direct visualization through the 15-mm port site. This is done without the use of any additional protective measures, but it must be done carefully to prevent specimen rupture and to ensure no spillage of gastric contents. No specific studies have been performed to evaluate methods of specimen extraction in sleeve gastrectomy. Some centers do utilize wound protectors or specimen retrieval bags. The 15- and 12-mm port sites are then closed laparoscopically using a suture passing device.
In 2014, an international expert panel was surveyed to develop best practice guidelines for the sleeve gastrectomy, which were then published in 2016. Their results were compared with the 2011 International Sleeve Gastrectomy Expert Panel Consensus and with data collected from a survey of general surgeons. The optimal bougie size proposed by the 2011 group was 32–36 French. Current recommendations lean toward a larger bougie to avoid strictures and leaks, which may be associated with smaller bougie sizes. The average bougie size used by experts today is a 36–37 French. Transection of the stomach should begin no less than 3 cm proximal to the pylorus. 15
The use of the appropriate staple height for different parts of the sleeve is more prominent in the 2014 consensus. 15 It is recommended that a higher staple height is used for the antrum or thicker stomach in revisions. We use the Medtronic EndoGIA stapler black load for the first staple firing at the antrum. This uses Tri-Staple technology with successively longer staple heights (4.0, 4.5, and 5.0 mm) that is designed to be used for thick tissue. Of note, the black cartridge requires a 15-mm port for introduction. An alternative option is to remove the port for the first firing and pass the staple cartridge directly through the abdominal wall. For the remainder of the sleeve, we use medium height purple staple loads.
Staple line reinforcement is a controversial step of the procedure. We do not perform any additional reinforcement. The 2014 panel reported that 43.2% of expert surgeons used buttressing material for staple line reinforcement, 28.8% oversew, and 28.0% do not perform any staple line reinforcement. 15 Multiple studies have looked at leak rates with and without staple line reinforcement with differing conclusions. Knapps et al. performed a retrospective systematic review that demonstrated no difference in leak rates, mortality or morbidity in sleeve gastrectomy with or without staple line reinforcement. 16 Gagner et al. found that the leak rate in sleeve gastrectomy using absorbable polymer membrane was significantly lower compared with oversewing, nonabsorbable bovine pericardial strip reinforcement, and no reinforcement. 17 Imbrication of the staple line seems to be a more historical technique, with caution by the 2011 panel that this should occur with the dilator in place to avoid reducing the lumen size 18 but no discussion of the practice by the panel in 2014. 15
Neither panel addressed fixation of the sleeve to surrounding omental or retroperitoneal tissues. There have been few studies looking at this technique. Elbalshy et al. performed a prospective randomized study, and concluded that fixation should be performed as they found less postoperative vomiting, better gastric emptying, and decreased staple line bleeding. 19 Abdallah et al. published a retrospective analysis and found no significant differences in postoperative vomiting or leak, but lower rates of staple line bleeding or gastric axial rotation with fixation. 20 With no consensus and variable results, fixation remains a choice based on surgeon preference, and when performed can be done in an interrupted or running fashion.
Routine intraoperative leak tests have fallen out of favor for the sleeve gastrectomy. Leak tests can be performed through various methods such as endoscopy, insufflation with air or methylene blue. Multiple studies have demonstrated that intraoperative leak tests are neither predictive of leaks nor do they prevent leaks. 21 In fact, Sethi et al. even argued that intraoperative leak tests were associated with a higher rate of postoperative leaks, potentially related to putting additional stress on the staple line. 22 The ASMBS has stated that the intraoperative leak tests should be performed at the discretion of the surgeon, and has not recommended it as a routine practice. 23
The creation of a sleeve gastrectomy allows some degree of variation in surgical technique, but it is important to execute key elements of the procedure to produce safe and effective outcomes. In summary, the critical aspects of the procedure include the following: (1) complete mobilization of the greater curvature and posterior stomach, (2) appropriate sizing of the sleeve, (3) avoidance of narrowing at the incisura and gastroesophageal junction, (4) equal apposition of the anterior and posterior aspects of the sleeve while stapling to avoid spiraling, and (5) sufficient resection of the fundus to avoid leaving behind a large retained fundic pouch.
Postoperative Care for Sleeve Gastrectomy
As LSG has become more prevalent over the past decade, management in the immediate postoperative phase has evolved. Most patients are appropriate for transfer to the floor without continuous monitoring. Aggressive nausea prevention is provided to prevent vomiting and stress on the stomach. Utilization of scheduled antiemetics, multimodal analgesia with minimization of narcotics, as well as scopolamine and metoclopramide is effective in this regard. 24
Diet advance is varied and practice specific. Many groups start patients on a volume-restricted liquid diet immediately. In general, practices are based on gradual progression in food consistency and texture over 1–2 months. Patients begin with clear liquids, increasing the volume gradually. Intake should be in small portions, with no more than a half cup per serving. The daily intake goal is 2 L. If the patient tolerates this, liquid foods such as milk, soy drinks, and plain yogurt can be safely started without delay. After 1–2 weeks, patients progress to a mashed or puréed diet. It is recommended to separate liquids from solids by avoiding drinking beverages 15 minutes before or 30 minutes after eating. After 2 weeks, patients can start a soft diet, including food such as meatballs, eggs and soft, peeled fruits and vegetables. Some solid foods are incorporated at 1 month, including legumes, fresh vegetables, fresh fruit, and bread. By 2 months, patients may consume a regular balanced solid diet. It is recommended that patients progress to solid foods, as this encourages greater satiety and improved nutritional intake. 25
Our practice discharges the patient from the hospital after tolerance of 3 ounces per hour of full liquids. Timing regarding progression to solid diet also varies. We recommend a liquid diet only for the first week, then a pureed diet for the following week. Slow diet advance with solid foods is encouraged over a 4–6 week period. We recommend a goal protein intake of 60–80 g/day or 1–1.5 g/kg for ideal body weight.
Many obese patients suffer from OSA. Those with diagnosed OSA should be monitored after sleeve gastrectomy with continuous pulse oximetry and capnography. Patients who require continuous positive airway pressure during sleep are safe to continue use in the postoperative period; however, their personal device is preferred. 24
Obesity, marked by a chronic inflammatory state and associated with immobility, is a risk factor for deep venous thrombosis (DVT) and pulmonary embolus (PE). In the immediate postoperative period, early ambulation, lower extremity pneumatic compression devices, and either unfractionated or low-molecular-weight heparin have been shown to reduce this risk. Those patients who are at higher risk, such as those with history of DVT/PE, BMI >55 kg/m2, male gender, prolonged operative time, or patients who are nonambulatory, should be considered for an additional 2–4 weeks of prophylactic anticoagulation after discharge. 24
Most patients are ready for discharge to home on postoperative day 1 or 2. Some programs have begun to allow same-day discharge for selected patients after sleeve gastrectomy, but The Quality Improvement and Patient Safety (QIPS) Committee, on behalf of the ASMBS, has stated that the existing data do not currently support this practice. 24
Although LSG is viewed as a restrictive procedure, some degree of malabsorption is also to be expected. After recovering from surgery, patients are at risk of macronutrient deficiencies in the long term due to reduced dietary intake, decreased gastric secretion of hydrochloric acid and intrinsic factor, and poor food choices. Daily micronutrient supplements are necessary, including multivitamin concentrate (with iron, copper, and zinc), calcium citrate with vitamin D, vitamin B-12, and elemental iron, although multivitamins or nutritional supplements are typically not initiated in the immediate postoperative period. 24
Postoperative Complications and Management
The rate of major complications after LSG is between 0% and 6%.26–28 Early complications include leak, bleeding, symptomatic stenosis, DVT/PE, including a specific risk of portomesenteric venous thrombosis, and dehydration. Late complications include stricture, weight regain, and malnutrition.
Leak rates range from 0.5% to 7.0%, though most recent series are closer to 1%, reflecting improvement with time and experience.23,26,28 The etiology of leaks is attributed to either mechanical forces that stress the staple line or ischemia. An estimated 75%–85% of sleeve leaks occur at the proximal third of the greater curvature staple line, as opposed to the distal or antral staple line, and most series have reported leaks typically occurring at postoperative day 5 or later. 23
Risks for leak include bougie size >40 French, narrowing or stricture of the sleeve conduit, and inadvertent stapling of the esophageal wall. In patients with clinical signs or symptoms of a suspected leak after LSG, such as left upper quadrant pain, tachycardia, fever, or leukocytosis, upper gastrointestinal contrast studies have a low sensitivity (0%–25%), though higher specificity (90%–95%). Due to greater sensitivity, computed tomography (CT) with oral and IV contrast is now recommended as the method of choice for diagnosis of a leak in patients with suggestive signs or symptoms who are clinically stable. Routine immediate postoperative imaging studies are no longer recommended unless there are concerning clinical signs. Patients who are not stable enough to undergo CT should return to the operating room for diagnostic laparoscopy. For an acute postoperative leak, the objective is to prompt adequate drainage to prevent or mitigate abdominal sepsis. In addition, the surgeon should consider insertion of a feeding jejunostomy. The goal of early surgical management is not definitive repair of the leak; however, in the setting of very early reoperation, within 72 hours, primary suture repair is feasible. Essential treatment includes adequate drainage, nutritional support, and antibiotics. In most cases, resolution of the leak is a matter of time, sometimes taking several months. 29
Multiple surgical procedures have been described for chronic nonhealing fistulas, including gastrojejunal anastomosis, conversion to Roux-en-Y gastric bypass, completion of gastrectomy with esophagojejunostomy, and T-tube placement. 29 Advanced endoscopic treatments to address leaks are emerging and becoming more commonplace in an effort to avoid surgical interventions. Endoscopic stent placement is a solution with variable success rates. 30 Oftentimes, multiple endoscopies are required for stent replacement or for the addition of other endoscopic adjuncts. Migration, kinking, erosion, and patient intolerance may complicate the use of endoluminal stents. Endoscopic clip placement is another method that may help manage a leak. 31 Endoscopic placement of a double pigtail stent through the perforation site has been used in cases of limited intraperitoneal contamination and provides the advantage of early drain removal without residual chronic fistula. 30 Other options that are still in the experimental phase at the time of this writing include endoscopic suturing devices 30 and endoluminal vacuum-assisted closure. 32 Endoscopic injection of sealants such as fibrin glue or cyanocrilate has been used, although with mixed rates of success. 33
Stenosis can result from surgical technique or ischemia with subsequent stricture development. Clinically significant stenosis occurs in 0.5%–3.5% of cases, most often a short segment located at mid-body, near the incisura. 34 Initial management consists of endoscopic balloon dilatation. Many patients require two to four dilation sessions, with long-term success rates reported at 95%–100%. 35 The risk of perforation associated with dilation is 2%–5%. For those patients in whom endoscopic dilation fails, treatment options include endoscopic stenting, longitudinal seromyotomy, median gastrectomy with gastrogastric anastomosis, 36 and conversion to Roux-en-Y gastric bypass.
Postoperative hemorrhage is rare after sleeve gastrectomy and less common than with gastric bypass. Bleeding usually occurs at the staple line and is extraluminal in about half of the cases. CT scan confirms the diagnosis, and emergent surgical intervention is required for clinically significant active hemorrhage. For intraluminal bleeding, endoscopic interventional methods, including epinephrine injection, heater probe, and clipping, are effective. 37
Significant GERD has been considered a contraindication for sleeve gastrectomy. Some studies show an increased prevalence of GERD in patients after LSG, with potential causes including hypotensive lower esophageal sphincter, disruption of the angle of His, resection of sling fibers, reduced gastric compliance with higher intragastric pressure, decreased gastric emptying, late dilatation of the sleeve, and occurrence of hiatal hernia. 38 However, a 2014 prospective study from Italy evaluating for GERD in 65 patients after LSG, including 24-hour pH probe data, suggests that pre-existing reflux improved in patients after surgery, and that the rate of de novo reflux was only 5.4%. 10 The ASMBS currently does not recommend empirically starting antacid medication after sleeve gastrectomy. 24
For those patients who do develop reflux after LSG, treatment usually consists of proton-pump inhibitor medication or conversion to Roux-en-Y bypass.35,39 A recent pilot study including 6 selected patients 40 demonstrated feasibility of a laparoscopic anterior fundoplication of the proximal sleeve with posterior crura approximation for treatment of post-LSG reflux, given that preoperative evaluation demonstrated enough tissue volume of the proximal gastric pouch to allow fundoplication.
Portomesenteric venous thrombosis is a rare complication of LSG thought to be secondary to locoregional postsurgical inflammation, change in venous outflow, and dehydration predisposing to clot formation. Patients may present 1–2 weeks after surgery with vague abdominal pain, severe nausea and vomiting, fever and diffuse abdominal tenderness. Diagnosis is confirmed with CT scan, and treatment consists of anticoagulation, fluid resuscitation, and bowel rest. Thrombolytics may be indicated depending on severity of symptoms. There are no established guidelines for duration of anticoagulation therapy, but patients are usually treated for 3–6 months. Surgical treatment is reserved for patients with evidence of infarcted bowel. 41
In recent data, LSG has shown to be a durable, successful weight-loss treatment. EWL percentages at the 5-year mark fall between 50% and 70%. The long-term EWL after LSG appears to be inversely proportional to preoperative BMI. For those patients who fail to meet their goal EWL or who experience weight regain, surgical options include re-sleeve gastrectomy, conversion to Roux-en-Y gastric bypass, or duodenal switch. There is insufficient evidence to determine which operation is best for weight regain, but a systematic review of the existing literature suggests that both re-sleeve and conversion to gastric bypass are equally effective operations after failed LSG, with similar EWL and BMI in patients 2 years after reoperation. 42
Conclusions
Since its evolution from the initial step of a staged procedure to a stand-alone procedure, the LSG has emerged as the most commonly performed bariatric operation worldwide. It has proven to be safe and effective in addressing weight loss and metabolic derangements. In addition, long-term outcomes have demonstrated the durability of LSG comparable with that of other bariatric procedures. The technical ease of the procedure, coupled with decreased surgical complications in comparison with other more complex surgical options, has bolstered its popularity among patients and surgeons. This article describes the key principles of the operation that are essential for safe and effective outcomes. Although there remains some controversy, such as the optimal workup and procedure choice for morbidly obese patients with GERD, the sleeve gastrectomy has established itself as a successful option in the surgical treatment of obesity and related diseases.
Footnotes
Disclosure Statement
No competing financial interests exist.