
Abstract
Abstract
Objective:
To evaluate the surgical outcomes of single-site laparoscopic percutaneous extraperitoneal closure (SLPEC) and modified transumbilical two-port laparoscopic suturing (M-TTLS) of the hernia sac for the treatment of pediatric inguinal hernia (PIH) and determine whether one approach was superior to another.
Methods:
From January 2014 to June 2017, a total of 599 children had undergone SLPEC or M-TTLS in our department. SLPEC and M-TTLS were the most frequently performed single-site laparoscopic procedures for PIH in our department, which represented the extraperitoneal and intraperitoneal approaches, respectively. All patients were followed up at the out-patients' clinics and the medical records were reviewed with respect to all operative outcomes.
Results:
There were 412 patients undergoing SLPEC and 187 patients undergoing M-TTLS, of which 358 hernias were on the right side, 172 on the left and 69 bilaterally. Two hundred and thirty-one unilateral hernias with contralateral patent processus vaginalis underwent contralateral repair at the same session. Mean operation time was 10.81 minutes in unilateral repair and 17.00 minutes in bilateral repairs, respectively. The perioperative complications included minor extraperitoneal hematoma in four (0.44%) patients, recurrence in one (0.11%), hydrocele in five (0.56%), and contralateral metachronous inguinal hernia in three (1.00%). No other complication developed in either group. There was no significant difference of complications between the two approaches except for the longer operation time in M-TTLS.
Conclusions:
Both SLPEC and M-TTLS were the safe and effective methods for PIH. The complications were comparable for M-TTLS and SLPEC, but operation time was significantly longer in M-TTLS than in SLPEC.
Introduction
P
Laparoscopic PIH repair can be performed transperitoneally (i.e., intraperitoneal approach) or through a percutaneous extraperitoneal approach with transperitoneal visualization (i.e., extraperitoneal approach).1–3 Each laparoscopic approach has its own advantages and disadvantages, and so far there is no sufficient evidence favoring one approach over another. 2 To overcome the inherent limitations of initial procedures, the surgical techniques of both approaches have evolved constantly with the trends of high success rate, few complications, minimal invasiveness, and improved cosmesis.1–3 Nowadays, single-site Laparoscopic closure of the hernia sac has been increasingly used to manage PIH worldwide.
Single-site laparoscopic percutaneous extraperitoneal closure (SLPEC) 4 and modified transumbilical two-port laparoscopic suturing (M-TTLS) 5 were the two most frequently performed procedures for PIH in our department. They also represented the extraperitoneal and intraperitoneal approaches for laparoscopic PIH repair, respectively. In this study, we evaluated the surgical outcomes of SLPEC and M-TTLS for the treatment of PIH and determined whether one approach was superior to another.
Materials and Methods
Study design
This is a single-center, retrospective study, including 599 patients who underwent SLPEC or M-TTLS for PIH in our department from January 2014 to June 2017. This study was approved by our Institutional Review Board, and informed consent for the procedures was obtained from all patients' guardians before the operation. All patients were clinically diagnosed as an indirect inguinal hernia, and those who underwent other procedures at the same time were excluded. All procedures were performed by a single surgeon.
Patients were allowed to drink a little water at the third hour after surgery and eat liquid diet at the sixth hour postoperatively. Patients were discharged if they did not complain obvious discomfort for four continuous hours. All patients were followed up at the out-patients' clinic after 1 week, 1 month, and 6 months. Medical records were reviewed with respect to presence of contralateral patent processus vaginalis (CPPV), intraoperative injury, conversion to other procedure, operation time, recurrence, hydrocele, contralateral metachronous inguinal hernia (CMIH), and other postoperative complications.
Surgical procedures
After general anesthesia, the patient was placed in the Trendelenburg position. According to the body size of patient, a 3 mm or 5 mm incision was made at umbilicus, through which a corresponding trocar was inserted and a pneumoperitoneum was established at 8–12 mmHg. A single port was usually sufficient for most of the SLPECs, although sometimes a grasping forceps was needed to assist the procedure. As for M-TTLS, another umbilical port with a laparoscopic needle holder was always required. The internal inguinal ring (IIR) of the unilateral inguinal hernia was routinely observed, and prophylactic surgery was performed if a CPPV was present.
During SLPEC, a 3 mm incision was made at the corresponding skin of IIR, from which an 18-gauge epidural needle loaded with a silk suture loop was introduced (Fig. 1a). The needle was advanced extraperitoneally on the medial side of IIR (Fig. 1b) and passed into the peritoneal cavity lateral to the spermatic vessels or the round ligament of uterus (Fig. 1c). When it was difficult to separate the vessels and vas from peritoneum, the “hydrodissection” technique could be used by infusing a small amount of saline solution into the preperitoneal space through the sheath of the epidural needle. 6 The suture loop was pushed into peritoneal cavity by a modified spinal needle and the epidural needle was withdrawn to the roof of IIR (Fig. 1d). The epidural needle was kept advancing along the lateral side of IIR and passed into the suture loop in the cavity at the same puncture site (Fig. 1e). Aided by the spinal needle and laparoscope, a long suture loop was sent into the first loop in peritoneal cavity (Fig. 1f). The needles were withdrawn out of the abdominal wall by inserting the laparoscope into the long loop to fix the suture (Fig. 1 g). Finally, the long suture loop was pulled out of the abdominal wall by picking up the first loop, and IIR was closed by knotting the suture extracorporeally (Fig. 1h).
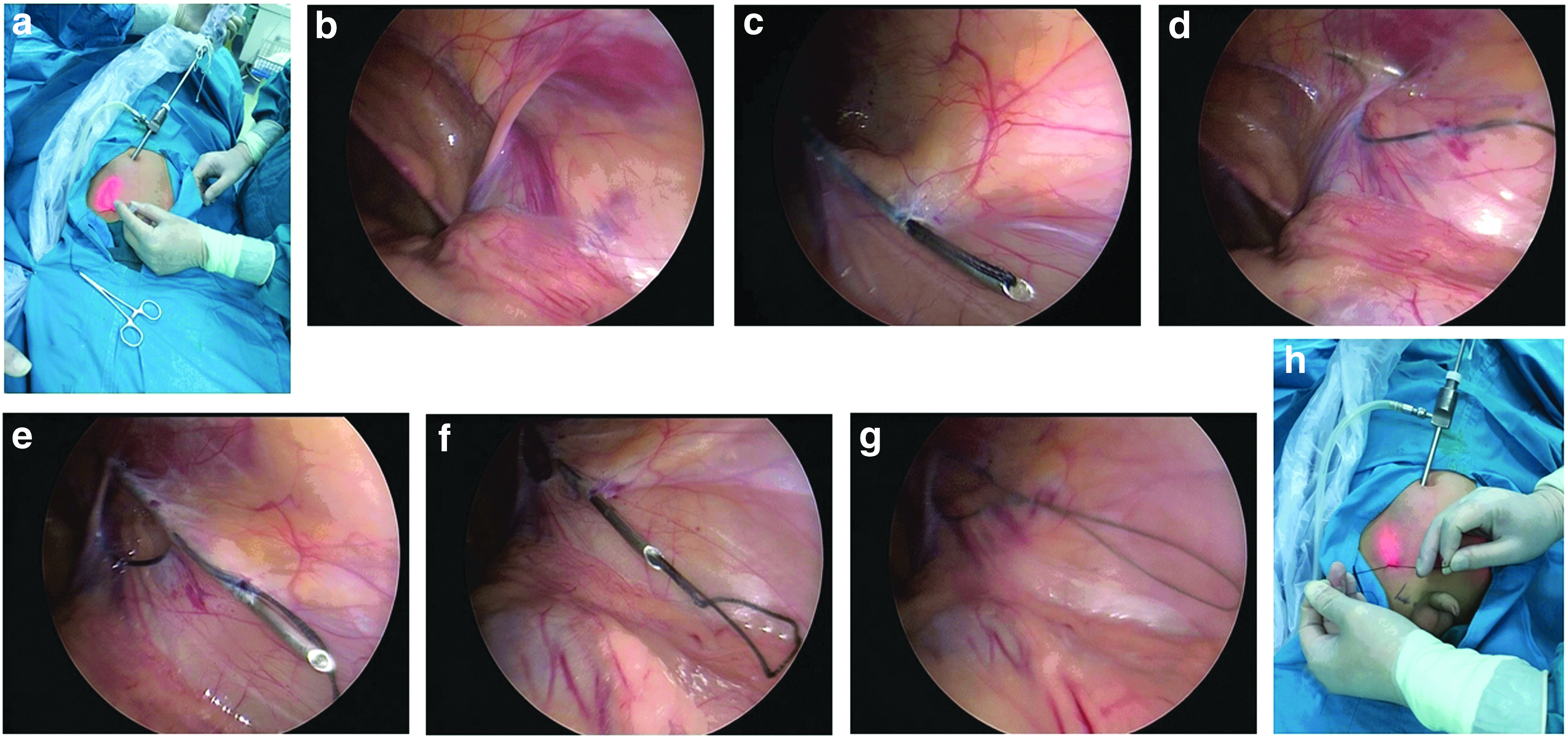
Description of the technique of SLPEC:
During M-TTLS, a long syringe needle (0.9 × 80 TWLB) was punctured into the preperitoneal space above IIR (Fig. 2a). After the peritoneum separated from the vessels and vas by hydrodissection, the syringe needle was left in peritoneal cavity (Fig. 2b). A medical suture needle (○1/2, 7 × 17) loaded with a 2–0 silk suture was introduced into peritoneal cavity transparietally, and its tip was then inserted into the hole of the syringe needle by a laparoscopic needle holder (Fig. 2c). Under the guidance of the syringe needle, the peritoneum on the surface of the vessels and vas was sutured intactly by a single stitch (Fig. 2d). Subsequently, the rest peritoneum around IIR was sutured continuously in a clockwise direction (Fig. 2e). After a complete purse-string suture with about two to four stitches, the needle was cut from the suture and retrieved through the abdominal wall. IIR was closed intracorporeally with a triple knot by using a single-instrument tie technique, which used a grasping forceps to loop the suture in peritoneal cavity (Fig. 2f), then pulled the suture end out of the loop (Fig. 2g), and finally held the external suture end tightly by hand and pulled the intraperitoneal end by forceps to the opposite direction (Fig. 2h).
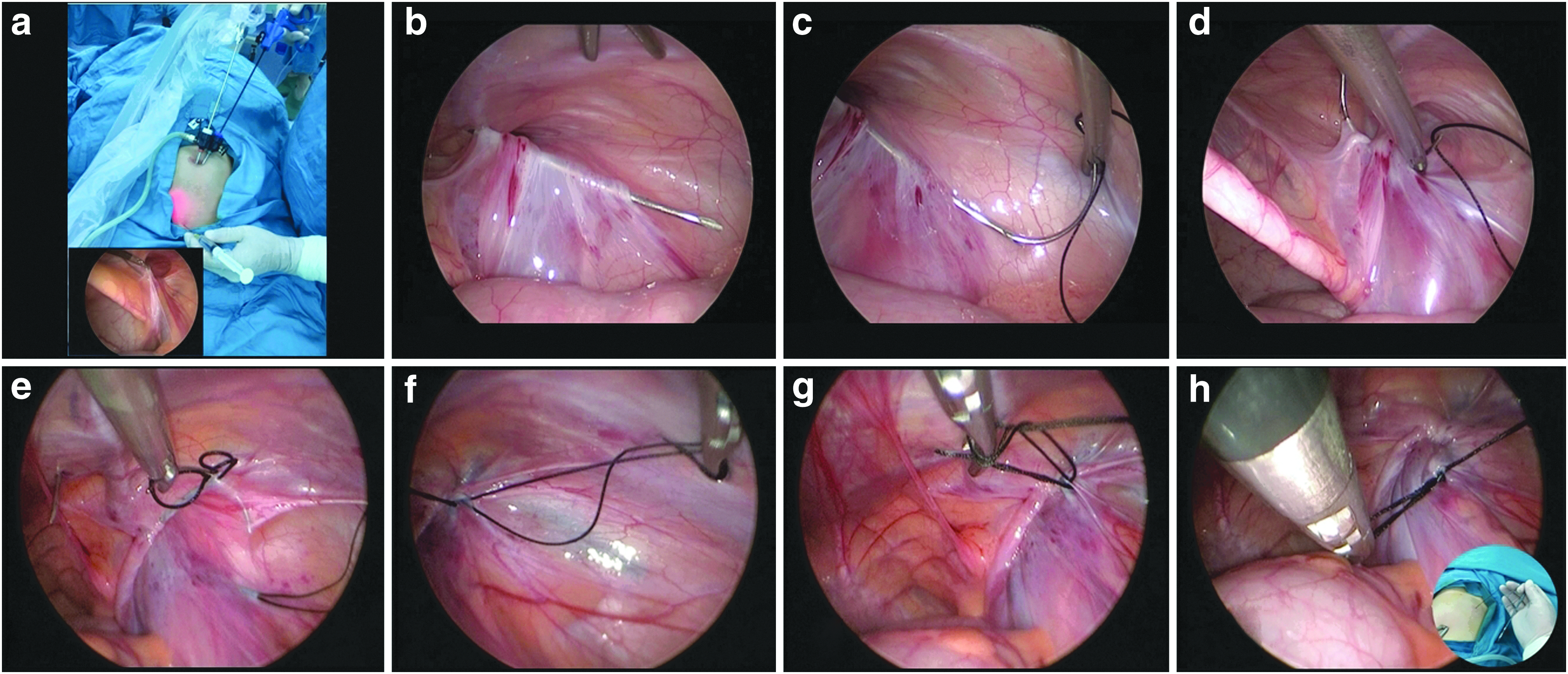
Description of the technique of M-TTLS:
Statistical analyses
For continuous variables, numeric values are expressed as mean ± SD, and normal distribution was tested by Kolmogorov–Smirnov test. The independent samples t test was used to compare the normally distributed variables and the Mann–Whitney U test for the non-normally distributed. For categorical variables, the significance of differences between the two groups was evaluated by Chi-squared or Fisher's exact test. Statistical analyses were performed using Stata 12.0 (Stata Corporation), and a two-sided P < .05 was considered statistically significant.
Results
The patient characteristics are shown in Table 1. There were 412 patients undergoing SLPEC (“SLPEC group”) and 187 patients undergoing M-TTLS (“M-TTLS group”), respectively. The mean age at operation was 3.37 years. Among them, there were 533 boys and 66 girls; 358 inguinal hernias were on the right side, 172 on the left, and 69 bilaterally. Among the 530 unilateral hernias, 231 had undergone contralateral repair because of coexisting with a CPPV. Thus, a total of 899 (299 unilateral and 300 bilateral) repairs were performed in this series. Mean follow-up period was 26.21 months.
Patient Characteristics
CPPV, contralateral patent processus vaginalis; M-TTLS, modified transumbilical two-port laparoscopic suturing; SLPEC, single-site laparoscopic percutaneous extraperitoneal closure.
Surgical outcomes are listed in Table 2. During the operation, minor extraperitoneal hematoma occurred in four (0.44%) patients, of which one (0.16%) in the SLPEC group and three (1.06%) in M-TTLS (P = .095). The hemorrhage was self-limited or stopped after the purse-string suture was tied. All operations were completed as planned without conversion. Mean operation time was 10.81 minutes (9.72 minutes in SLPEC vs. 13.31 minutes in M-TTLS, P = .000) in unilateral repair and 17.00 minutes (13.00 minutes in SLPEC vs. 25.50 minutes in M-TTLS, P = .000) in bilateral repairs, respectively.
Surgical Outcomes
CMIH, contralateral metachronous inguinal hernia; M-TTLS, modified transumbilical two-port laparoscopic suturing; SLPEC, single-site laparoscopic percutaneous extraperitoneal closure.
After the operation, there were nine cases with complications. There was only one (0.11%) case with recurrence, which occurred in a (0.16%) girl in SLPEC (P = 1.000). Hydrocele developed in five (0.56%) patients, of which three (0.19%) in SLPEC and two (0.71%) in M-TTLS (P = .653). Three of the five hydroceles were resolved with observation, while the other two needed a testicular sheath inversion surgery. CMIH was detected in three (1.00%) unilateral repairs, of which two (0.96%) in SLPEC and one (1.10%) in M-TTLS (P = 1.000). No wound infection, suture granuloma, groin pain, testicular atrophy, and ascending testis developed in either group.
Discussion
Laparoscopic repair of PIH has gained increased popularity due to its abovementioned advantages, and numerous techniques have been described in literature so far.2,3 However, traditional laparoscopic surgery, which required placement of three ports on the abdominal wall, was not cosmetically superior to open inguinal repair, wherein the single incision could be hidden within the groin crease. 7 Currently, there was a trend of increasing use of single-site laparoscopic surgery for PIH repair because of its excellent cosmetic results.4,5,8,9 Although single-site laparoscopic surgery was technically more demanding for the surgeon, it still could reproduce the outcomes of traditional laparoscopic repair and not exert additional risk to the patient if performed by an expert. 10 Furthermore, it was believed that the safety of single-site laparoscopic surgery could be improved because it obviated the need for additional trocars and hence the risk of trocar injury. 11 The current study presented a very low complication rate and relatively short operation time, which also showed that single-site laparoscopic surgery was a safe and effective method for the treatment of PIH.
Single-site laparoscopic closure of the hernia sac could be performed through either an extraperitoneal or intraperitoneal approach, and each approach had the pros and cons of their own. Accordingly, we made some modifications to conquer their limitations and established the SLPEC 4 and M-TTLS. 5 SLPEC was one of the most representative extraperitoneal techniques. It did not need skilled intracorporeal suturing and knot tying, and could be performed easily even by the beginners. In contrast, M-TTLS was an essentially intraperitoneal technique, which required mastery of the laparoscopic manipulations and hence a longer learning curve. In 2010, Shalaby et al. 12 compared laparoscopic intraperitoneal suturing with extraperitoneal knotting for repair of PIH and found shorter operation time in extraperitoneal knotting. Therefore, it was not surprising that the operation time in this study was significantly shorter with SLPEC than with M-TTLS for both unilateral and bilateral PIH repairs.
Vessel injury was the most common complication during SLPEC and M-TTLS, although small in number. 3 These vessels included the iliac vessels in the triangle of doom, the inferior epigastric vessels, and the spermatic vessels, as well as small peritoneal vessels. As they are very close to the peritoneum at the level of IIR, they were likely to be punctured unexpectedly by the sharp tip of the needle (e.g., the epidural needle for SLPEC and suture needle for M-TTLS). Generally, the hemorrhage could be stopped by conservative treatment, such as observation and manual extracorporeal compression. 8 To reduce the vessel injuries, we introduced the “hydrodissection” technique to lift the periorificial peritoneum off the vessels and vas by infusing the saline solution into preperitoneal space.6,8 Besides reducing the injuries, “hydrodissection” also could greatly simplify and facilitate the operations. With the aid of “hydrodissection,” we had gained very few vessel injuries and no conversion in both the SLPEC and M-TTLS groups.
Recurrence was one of the most common complications after laparoscopic repair of PIH, especially through an intraperitoneal approach. In the early days, some surgeons intentionally jumped over the vessels and vas when suturing the peritoneum around IIR to avoid injury to these vital structures. 13 However, incomplete closure of the periorificial peritoneum probably caused significantly higher rate of recurrence. 13 Therefore, we introduced a percutaneous assistance in M-TTLS by using a long syringe needle, which could allow a single stitch of the peritoneum and folds on the surface of the cord structures. 5 Furthermore, it was also important to note that the needle-in point of next stitch must close to the needle-out point of previous stitch so as to leave no significant peritoneal gaps. 14 By adopting these modifications in M-TTLS, we had achieved a comparable low rate of recurrence with the SLPEC group.
Another concern after the operation was groin pain and suture granuloma in the ligated region where the hernia defect was repaired, especially for the extraperitoneal approach of laparoscopic PIH repair. 15 The extraperitoneal approach had been criticized by many authors for including the unnecessary subcutaneous tissues (e.g., muscles and nerves) in the ligature. The unexpected inclusion might lead to several problems, such as severe groin pain, suture granuloma, and even recurrence from later loosening of the knot. 8 Considering that, we introduced the “one puncture” technique in SLPEC, for example, withdrawing the epidural needle just to the preperitoneal space on the roof of IIR after setting the suture on one side, and then directly reintroducing the needle along the other side to bring out the preset suture. 8 By routinely using the “one puncture” technique, we had completely rooted out the above-mentioned complications from the current series.
Hydrocele was a potential complication following SLPEC and M-TTLS because the distal portion of the hernia sac was left intact and the lymphatics might be impaired by thicker bites of the peritoneum around IIR. 3 To bear this in mind, we sutured as few unnecessary tissues other than peritoneum as possible in both intraperitoneal and extraperitoneal approach of laparoscopic PIH repair. This study showed that hydrocele formation was not frequent, and there was no significant difference between the SLPEC and M-TTLS groups. During laparoscopic surgery, contralateral IIR could be simultaneously detected and repaired if a CPPV was present. This prophylactic surgery was proved to be very effective for preventing CMIH, although there were still very few cases with false negative exploration missed.16–18 Therefore, CMIH following laparoscopic repair was a relatively rare but possible phenomenon.16–18 Wound infection, testicular atrophy, and ascending testis were the other uncommon complications in laparoscopic repair. 2 Fortunately, they were almost unseen in the SLPEC and M-TTLS groups, perhaps due to the less and more precise operations.
This study has several limitations. The first limitation is the small sample size, which may not have enough power to detect all potential differences or capture rare complications, for example, testicular atrophy and ascending testis.19,20 The second is the relatively short duration of follow-up, which probably underestimates the incidence of some postoperative complications, such as recurrence and CMIH. 19 Finally, as a retrospective design, this study inevitably has some recall bias and difference of baseline characteristics between the SLPEC and M-TTLS groups, which likely has an impact on the comparative results. Therefore, in future, more well-designed studies with large population and long-term follow-up are expected to accurately assess the results in this study.
In conclusion, both SLPEC and M-TTLS were the safe and effective methods for the treatment of PIH. The complications were comparable for M-TTLS and SLPEC, but operation time was significantly longer in M-TTLS than in SLPEC.
Footnotes
Acknowledgment
The authors acknowledge the Natural Science Foundation of Ningbo Municipal Bureau of Science and Technology (2016A610177; 2014B82003) for funding this study.
Disclosure Statement
No competing financial interests exist.