
Abstract
Abstract
Introduction:
Endoscopic submucosal dissection (ESD) is an acknowledged endoscopic technique for the management of early gastrointestinal neoplasia. The clinical experience and the research from the Eastern ESD centers show that experienced endoscopists can successfully treat even the most demanding recurrent colorectal lesions.
Aim:
The aim of this study was to analyze the clinical outcomes of the management of recurrent colorectal lesions in comparison with those of primary lesions in the setting of high-volume European center.
Methods:
A retrospective analysis of 298 cases (228 primary lesions and 70 recurrent lesions) performed by a single endoscopist was carried out. Evaluating learning curves for both primary and recurrent lesions, cumulative sum analysis was performed.
Results:
Primary lesions had ∼9% higher R0 resection rate (86.84% versus 78.51%). Yet, this difference did not reach statistical significance (P = .091). The presence of recurrent lesion and lengthy procedure (≥150 min) are risks factors of R1 resection, whereas rectal localization of the lesion was associated with lower risk of R1 resection. The cumulative R0 of 80% was achieved at 36th procedure in the primary lesions group, whereas for the recurrent lesions it was reached at 50th procedure (overall 229 procedures).
Conclusions:
Our study underlines the importance of proper experience in ESD before the management of recurrent lesions. Even after the completion of high volume of primary lesions, first recurrent lesions can pose a challenge. Nevertheless, the final outcomes are promising, as the complications do not pose a serious risk to the patients and high R0 resection rate can be achieved in a reasonable timeframe.
Introduction
E
Materials and Methods
Retrospective analysis of clinical outcomes of consecutive ESD procedures was performed. We enrolled patients who have undergone ESD since April 2014 until October 2017. During this period 298 colorectal lesions were removed. A total of 228 patients had primary colorectal lesion, whereas 70 patients were referred to our center for recurrent colorectal lesion. All cases were performed by a single operator (M.S.). The patients were selected based on the following criteria—lesions not qualifying for the en bloc resection by standard polypectomy or endoscopic mucosal resection (EMR) technique (≥2 cm, lesions with fibrosis from previous resection attempts). The patients were disqualified from ESD on the following basis: (1) suspicion of deep submucosal invasion; (2) coagulopathy; and (3) serious medical state with a predicted overall survival time <6 months.
Endoscopist's experience before the study period
All the procedures were performed by a single endoscopist (M.S.). Before ESD training he had performed >400 EMRs and polypectomies in the colon. 12 Before starting the ESD procedure, he was trained at several international ESD hands-on seminars and received hands-on training directly from Japanese experts. During the duration of the study, he participated in two animal model ESD courses and underwent additional training in the Japanese center of excellence.
ESD procedure
Patients were admitted to the hospital the day before the procedure. On this day, patients underwent bowel preparation with 4 L polyethylene glycol (PEG). On the day of the procedure, patients received single-dose prophylactic antibiotic therapy. The first 30 ESD procedures were performed under conscious sedation with intravenous (i.v.) midazolam hydrochloride (10 mg). Fentanyl (1 mg) was given in the event of severe pain during the procedure. After 30 cases, all colonic and rectal ESD ≥5 cm were performed under general anesthesia in the operation theater. Procedures were carried out using a single-channel endoscope (Olympus EVIS Exera II CF-Q180AL/I; Pentax 90i; Olympus Company) with a disposable distal attachment (D-201–11804 or D-201–15004; Olympus Company). After 30 procedures all ESDs were performed with CO2 insufflation. Two different electrosurgical units were used: ERBE VIO 300D (ERBE Elektromedizin, Tübingen, Germany) and Bowa Arc 250 (BOWA-electronic GmbH & Co. KG). During the analysis period different knives were used: in 13 cases—Pentax Splash Needle, in 21 cases—Erbe Water Jet Knife, in 62 cases—Olympus DualKnife, and in 202 cases—Fujinon Flush 1.5 Knife. After detailed endoscopic evaluation of the lesion, the submucosa was injected with 0.9% saline or 6% mannitol solution and indigo carmine 0.01% and epinephrine 1:10,000 using a 25 G injector needle (Net 25-22 G5; Endoflex GmbH). To manage bleeding electrosurgical hemostatic forceps (FD411-QR; Olympus Company) were used. Mucosal defect on right-sided ESD cases was routinely closed with endoclips (HR 110 QR; Olympus Company). The same equipment was also used for closing intraoperative perforations.
Definition of a complication
Postprocedural bleeding was defined as significant bleeding with loss of ≥2 hemoglobin units after completion of procedure. Intraprocedural perforation was defined as visible cut through the muscle layer of the colonic wall during the dissection.
Histopathological assessment
Resected specimens were immersed in 10% formalin and sectioned serially at 2 mm intervals. They then underwent histological evaluation in accordance with the Vienna classification. 13 The histopathological assessment of the obtained specimens included lateral and vertical margins, budding and lymphovascular invasion.
Postprocedural hospitalization and follow-up
On the day of the procedure, the patient remained in fasting state and received 2000 mL crystalloids i.v. In the absence of significant bleeding during the procedure, the patient received low-molecular-weight heparin at a prophylactic dose in the evening. Antibiotic therapy was not given on a routine basis. In the absence of intraprocedural complications and an uncomplicated course on the first day after the procedure (postoperative day [POD] 1), on POD 2 a clear liquid diet was introduced instead of i.v. fluids and the patient was discharged from hospital with the recommendation of remaining on a liquid diet for another 2–3 days.
The first follow-up visit with the doctor was usually carried out 3 weeks after dissection and then again after 1 year. During the visit, the pathological report of the dissected specimen and any complications that occurred after discharge were discussed. When the pathological report excluded the presence of invasive cancer, the patient was scheduled for a first follow-up colonoscopy 6 months after ESD.
Statistical analysis
Basic patient-related data (gender, age), diameter of the lesions, histopathological type, laterally spreading tumor (LST) classification, and its localization were assessed. As for procedure-related and postprocedural data, duration of the procedure, grade of resection, and presence of complication were analyzed. We also calculated speed of the procedures (cm2/min) on assumption that every lesion had a shape congenial to the circle (thus A = πr2 formula was used).
As all the continuous variables had a distribution other than normal, they are reported with their mean and median values and interquartile range.
Variables were tested with Mann–Whitney test (when comparing 2 groups) or Kruskal–Wallis test (when >2 groups were compared). The chi-square test was used to assess the differences in a distribution of the categorical variables between the groups. Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY).
Analysis of R1 risk factors
When assessing the risk factors of R1 resection of the lesion, logistic regression model was applied. Having performed the fundamental analysis of factors associated with the clinical outcomes of colorectal ESD, we aimed to assess which of them influenced the procedure most. To this end, we evaluated the impact of factors on resection status of the procedures (R0 versus R1) as confirmed by the histopathological examination.
We applied logistic regression model. First, univariate analysis was performed, then multivariate analysis during which all the factors were fitted was performed. Continuous variables—diameter and time—were entered as categorical variables. Namely, patients were divided into subgroups using the following cut-off points: diameter ≥5 cm and time ≥150 min. Moreover, the procedure number was entered as a continuous variable into the analysis to assess whether there was a significant progress in the outcome of the procedures regarding the resection rate.
Comparison of learning curves
To evaluate learning curves for both primary and recurrent lesions, cumulative sum (CUSUM) analysis was performed. 14 As recurrent lesions are generally viewed as more challenging to resect, we aimed to build the learning curves for both types of lesions. CUSUM analysis was applied, as this method enables to accurately assess at which procedure the assumed cumulative resection rate was achieved.
Carrying out CUSUM, one has to assume acceptable and unacceptable failure rates (p0 and p1, respectively). Analyzing our data p0 and p1 were set at 0.2 and 0.25, respectively. The α error type and β error type were set at 0.1 as in standard CUSUM analysis. Having these values other coefficients were calculated (Table 1).
The CUSUM plot consists of two decision boundaries with the lower one (h0) reflecting achieving the acceptable failure rate and the upper one (h1) indicating that unacceptable failure rate is reached. The curve itself is built by adding the calculated values in the following manner:
For every success value “s” is subtracted from the CUSUM For every failure value “1 − s” is added to the CUSUM
The equation used for the calculation of the required coefficient and their values are given in Table 1.
In both cases the acceptable failure rate was set at 0.2 and the unacceptable failure rate of 0.25 was assumed (indicating R0 rate of 80% and 75%, respectively).
Results
In the analyzed period 298 colorectal ESD cases were performed in total. In this group 228 cases were primary lesions and 70 were recurrent.
The analysis of basic factors is given in Table 2. Statistically significant differences were found for mean time and speed of the procedures including the resected specimen size. Interestingly, primary lesions had ∼9% higher R0 resection rate (86.84% versus 78.51%). Yet, this difference did not reach statistical significance (P = .091).
IQR, interquartile range.
As given in Table 3, we observed significant differences in complication rate between the two types of lesions (15.32% versus 21.43% for primary and recurrent lesions, respectively, P = .011). The detailed analysis showed that although the observed perforation rate was higher in the recurrent lesions group, it did not reach statistical significance level (11.43% versus 7.54% P = .294). However, when analyzing rectal/proximal groups, we found that recurrent rectal lesions had significantly higher perforation rate (14.29% versus 4.31% P = .024), whereas no differences were found between proximal subgroups. In fact only one perforation occurred in the proximal recurrent lesions subgroup. Higher perforation rate did not have any serious clinical ramifications, as the perforated sites in low rectum did not have to be closed. The requirement of additional surgical treatment was similar in both groups. When it comes to the bleeding rate, it also did not differ significantly between groups (1.43% versus 3.95% P = .091). Thus, the disparity between recurrence rates (7.14% versus 0.88% P = .002) had the greatest impact on the overall difference in the distributions of complications.
Table 4 sums up the logistic regression model used for the analysis of R1 resection risk factors. It has revealed that factors such as the presence of recurrent lesion, the presence of big lesion (≥5 cm), and lengthy procedure (≥150 min) are all risks factors of R1 resection. The rectal localization of lesion was associated with lower risk of R1 resection. The volume of procedures that the operator performed also affected the results, as the more procedures were performed the lesser was the risk of R1 resection.
Rectum vs. proximal localization.
Intramucosal carcinoma vs. other types.
The bolded factors' values are statistically significant with p < 0.05.
CI, confidence interval; OR, odds ratio.
On multivariate analysis only diameter ≥5 cm from the listed factors did not reach the level of statistical significance. Seemingly, the lengthy procedure reflecting the intraprocedural difficulties is more accurate risk factor of complete resection failure.
Figures 1 and 2 show CUSUM plots for primary and recurrent lesions, respectively. In case of primary lesions the acceptable failure rate (h0) was achieved at 36th procedure and then the curve of CUSUM decreases only in correlation with the constant progression of operator's prowess.
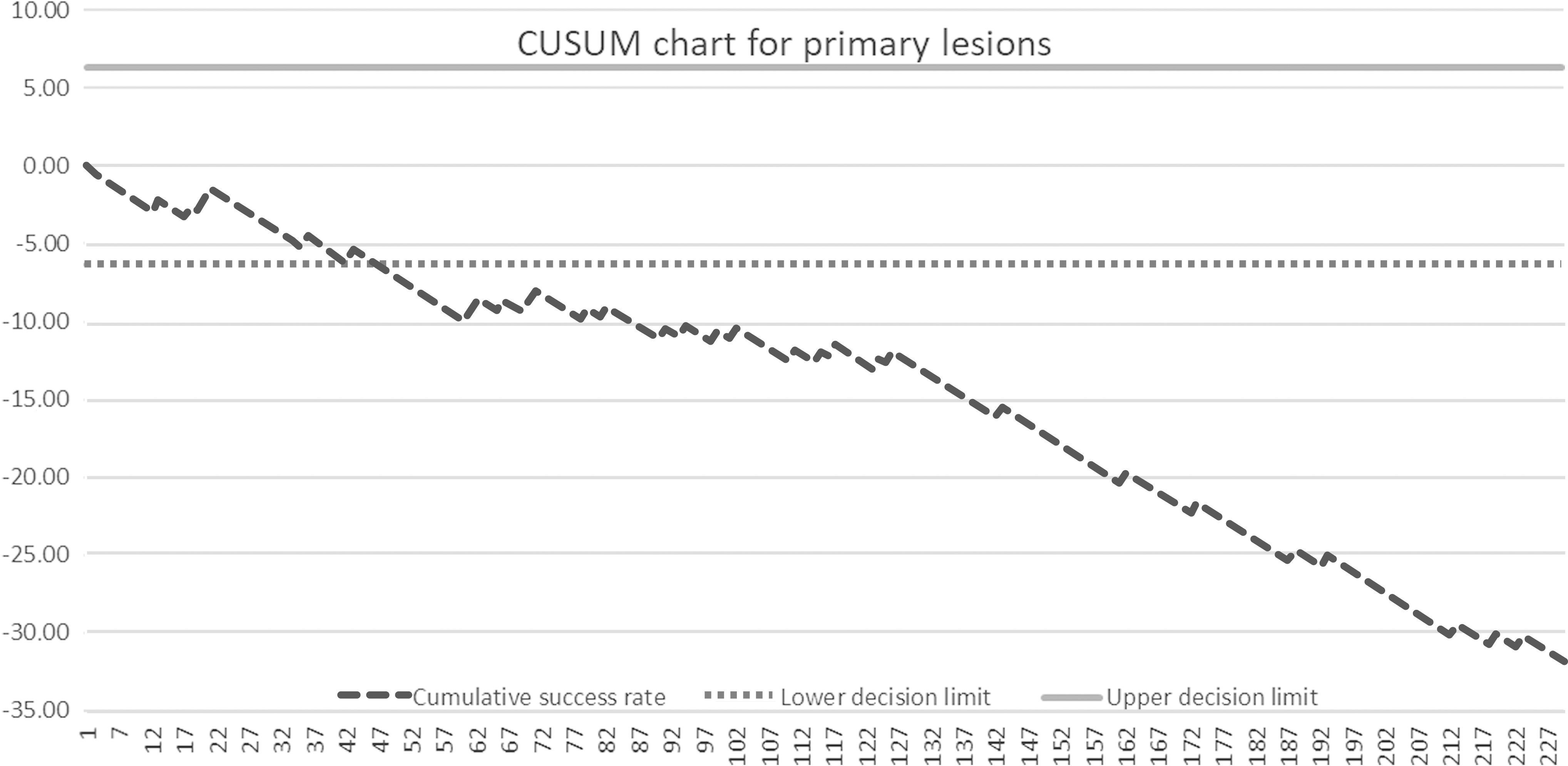
CUSUM analysis chart for primary lesions indicates reaching acceptable failure rate at 36th procedure. CUSUM, cumulative sum.
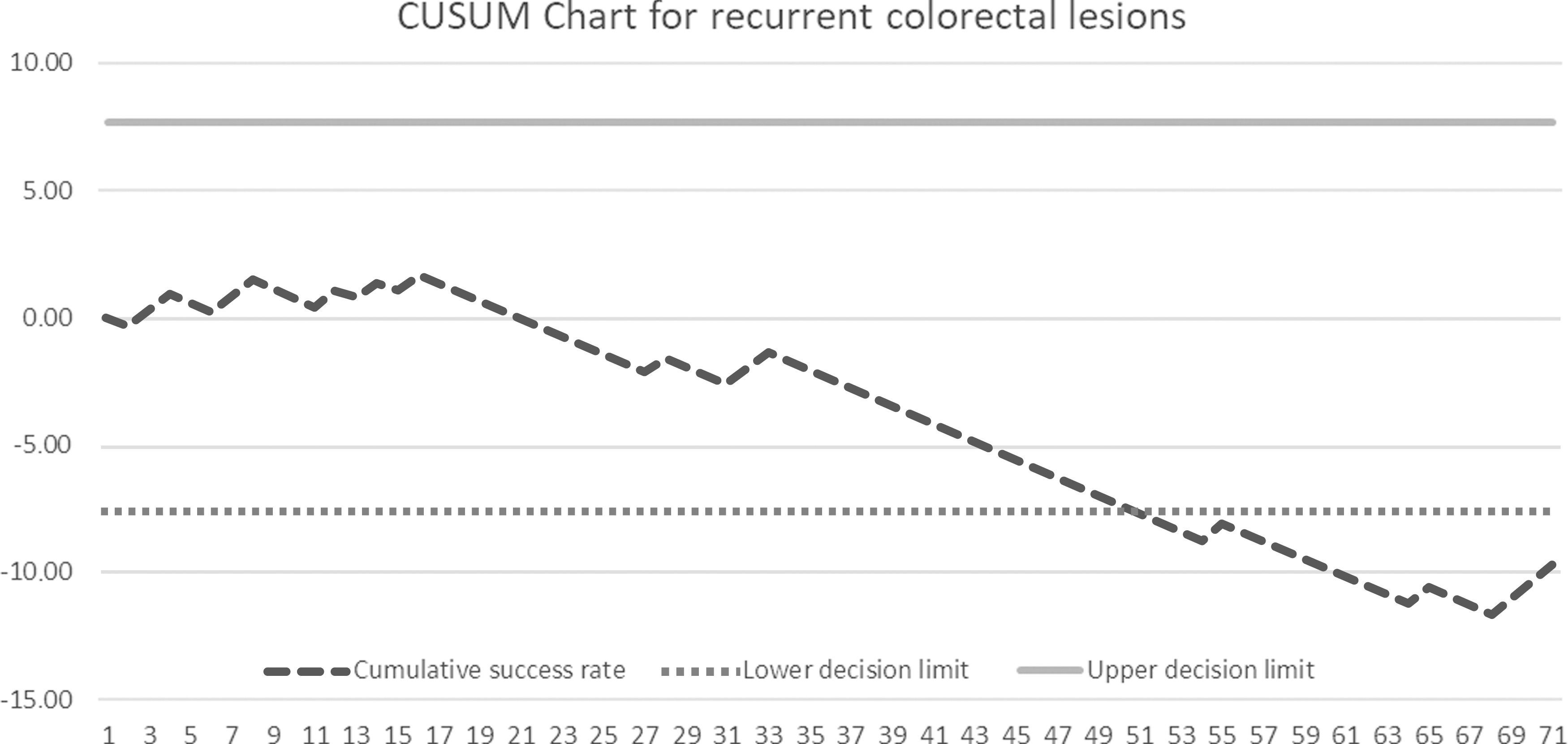
CUSUM analysis chart for recurrent lesions indicates reaching acceptable failure rate at 50th procedure. CUSUM, cumulative sum.
On the contrary, recurrent lesions are characterized by a lower rate of progression. The acceptable failure rate of 0.2 was reached at 50th procedure and the curve of CUSUM was not constantly decreasing, as a few cases with a resulting R1 resection status were performed in the later period of the study. This analysis is of particular interest in this study, as a simple chi-square test did not reveal statistically significant difference in R0 resection rate between these two groups (84.9% for primary lesions versus 78.51% for recurrent lesions, P = .091) and therefore do not reflect the presence of technical difficulties associated with the removal of recurrent lesions.
Discussion
The proper management of the recurrent colorectal lesions poses significant technical difficulties. Usually this kind of lesions do not elevate after the submucosal injection of fluid, thus mucosectomy is predominantly impossible. 8 Even if piecemeal removal is feasible, it cannot be considered as a method of choice, as such a management results in high recurrence rate.15,16 Argon plasma coagulation could also be considered, but it usually does not remove the lesion completely and does not provide a specimen for the histopathological assessment. En bloc resection of recurrent colorectal lesions is paramount especially in case of an early adenoma recurrence, as a quick progression to adenocarcinoma is highly probable.17,18
The endoscopic methods are of particular importance when treating rectal lesions. 19 As surgical treatment entails a significant decrease of patients' quality of life, it should be reserved for the cases in which endoscopic treatment cannot be carried out. It should also be highlighted that a precise histopathological assessment of the depth of invasion is also crucial as it can discriminate an early adenocarcinoma (depth of invasion—SM1) from pathologies that infiltrate deeper layers and require surgical treatment. 2
Taking into account these issues, new techniques have been proposed, for instance, endoscopic full thickness resection (EFTR). Although promising, this is still not a standard method. Usefulness of EFTR is hampered by few considerable limitations—it can only be applied for the lesions with a diameter of up to 20 mm, endoscopist can carry out only one try to resect the lesion and the resulting specimen's edges are difficult to assess.20,21
Transanal endoscopic microsurgery (TEM) is another option as it yields similar results in terms of R0 resection, complications, and recurrence rates.22–24 Although the fact that its application is limited only to the rectal localization is not a significant disadvantage per se, the certain conditions that should be fulfilled lower its efficacy. First of all, TEM can be applied only when lesions are located within the first 18–20 cm from the anal verge and ideally a 5 cm distance between lesions and the dentate line should remain. 25 Second, lesions located on the sphincters level and those located in the upper part of the rectum cannot be easily resected by the means of TEM. As for the lesions spreading above the sphincters, the proper postoperative anorectal function comes into question. However, the studies show that it is only intermittently distorted.26,27 In addition, the size of the lesion also limits the possibility of its performance namely, when full-thickness excision is required, large lesions that cover >50% circumference of rectum pose a technical challenge in terms of suturing. Therefore, lesions with a bigger diameter (≥5 cm) are suboptimal candidates for TEM management, 28 as they require full-thickness resection. Nevertheless, small recurrent rectal lesions can be safely managed with excellent results.29,30 Regarding some direct advantages of ESD over TEM, it is associated with a shorter hospital stay and lower costs.22,31 It should be also noticed that learning curve of TEM is similarly steep as that of ESD. 32 Yet, after the completion of a demanding training in TEM, one can treat only lesions confined to the rectum, whereas a trainee in ESD can potentially manage any malignancy located within the whole length of the colon.
Taking into account all the discussed aspects, ESD seems to be the most versatile technique, although not flawless. Its main advantage consists in the fact that it can be performed virtually in any localization in the GI tract and there is no limitation regarding the diameter of the lesion.33–35 However, this comprehensiveness has its price—the learning curve of ESD is long—even in case of primary colorectal lesions. This is especially true in case of lesions located in the right side of the colon. 4
According to the European Society of Gastrointestinal Endoscopy (ESGE) guidelines, 1 EMR is a first-line therapy in the treatment of early epithelial neoplasia in colorectal localization, unless there is a high risk of submucosal invasion (e.g., LST-nongranular type, lesion with a central depression).
Of note, Japanese guidelines place greater emphasis on ESD management, as local endoscopists achieved excellence in this technique. 2 As every lesion should undergo R0 resection, ESD is a regarded as a method of choice for treatment of lesions ≥20 mm and all recurrent ones. As European endoscopists still have relatively less experience in ESD management of recurrent lesions, according to ESGE, TEM is a recommended method in the management of rectal recurrent lesions. As stated previously, the aforementioned techniques do not lack significant limitations.
In our study, we aimed to assess the clinical outcomes of the management of recurrent colorectal lesions with the comparison of those of primary colorectal lesions. Having these results we focused then on comparing their respective learning curves. Such an evaluation may constitute a valuable evidence supporting ESD as a method of choice for recurrent colorectal lesions.
Our good clinical outcomes regarding the management of recurrent colorectal lesions can be partly explained by the fact that these lesions were significantly smaller than their primary counterparts and more importantly by the fact that their most common localization was rectum (65.71% versus 50.9% for primary lesions P = .019), which is generally associated with relatively easier ESD procedures.
Obviously, these observations cannot be analyzed separately, as every ESD expands operator's experience. As stated, we have reached >80% R0 resection for primary lesions after 36th procedure. As 11 procedures as a result of recurrent lesions were carried out in the meantime, it took overall 47 procedures to reach this level of excellence in this aspect. The same level of excellence was achieved after 50 procedures as a result of recurrent lesions. Yet, 179 primary lesions were removed in this period, thus it was only after 229 procedures.
Indeed, R0 resection rate is a parameter that indicates best whether a certain endoscopist achieved excellence in ESD technique. 36 Therefore, we mainly focused on its analysis, and explored the potential risk factors of R0 resection failure. As given in Table 4 on both univariate and multivariate analyses, the presence of recurrent lesions and lengthy procedure (≥150 min) highly increases the risk of R1 resection (∼7.5 times higher likelihood when both factors are present). Similarly diameter of ≥5 cm proved to be a risk factor on the univariate analysis, but failed to reach a statistical significance in the multivariate model. On the contrary, rectal localization of the lesion was associated with a lower R1 resection rate. Another factor that also reduces the risk of R1 resection is the number of the procedure. This result gives us particularly positive feedback, as it clearly shows the progress of the endoscopist's prowess in ESD and reflects the steady decrease in R0 resection failure.
As for the complications, recurrent lesions were characterized by significantly higher rate (21.43% versus 15.32%, P = .011). The observed difference is similar to the ones reported in the other studies. 37 However, contrary to the recognized paradigm we did not observe much higher perforation rate. In our experience only recurrent lesions located in the proximal colon are at the greater risk of perforation. This may be because of the difficulties in stabilizing an endoscope in this position, thinner wall, and greater fibrosis of these lesions. Similar amount of surgical intervention in both groups partly shows that a proper management of recurrent lesion by an experienced endoscopist is safe and not associated with serious complications. The most notable difference that we found is the one pertaining to the recurrence rate. As shown by previous studies, these lesions are inherently correlated with the presence of another recurrence in the follow-up period.
Although most of the patients in the recurrent lesions group were ultimately diagnosed with benign lesion, 4 cases of recurrent adenocarcinoma SM1 were present. The clinical outcomes of these patients clearly highlight the importance of a proper en bloc, ideally R0 resection of such lesions. In two cases piecemeal resection was performed. Another recurrence was found after ∼5 months in both cases and the patients were qualified for the surgical treatment. Regarding the intramucosal adenocarcinomas that were resected en bloc in the R0 manner, no complications after the procedure occurred and the patients were recurrence-free in the follow-up period. Thus, only meticulous en bloc resection decreases the local recurrence risk and the overall oncologic risk. Moreover, complete resection can usually spare the patients the need of surgical treatment.
As for the other cases of recurrence, no serious complication occurred and all of them were successfully treated during the following hospitalizations. Regarding the primary lesions group, 2 patients underwent another successful ESD procedure, as both did not have any signs of recurrence in the follow-up period. One patient had to be treated surgically—he fully recovered during the postoperative period and did not require another intervention in the follow-up period. As for the recurrent group, 3 patients were subsequently treated surgically, with no complications in the postoperative period and no signs of another recurrence in the follow-up period. Two of them were treated by ESD procedure with uneventful follow-up period.
To conclude, first cases of recurrent colorectal lesion are especially challenging for endoscopists and only after the management of relatively high volume of colorectal ESD cases can they be completely safely removed. Seemingly, the complications do not pose a serious risk, as they were successfully managed during endoscopy.
Taking into account the safety profile of ESD and its versatility, it can be hypothesized that its dissemination is going to progress in the near future in Europe. 38 With a greater number of experienced European endoscopist, ESD might be drafted to the ESGE recommendations as a method of choice for the management of recurrent colorectal lesions.
Nevertheless, when encountering colorectal lesions the whole spectrum of therapeutic options should be analyzed, “tailoring” the final choice of the management method optimal for lesion's localization, diameter, the risk of invasive adenocarcinoma, endoscopist's experience, the feasibility of endoscopic treatment, and the consequences of surgical treatment (Table 5). Therefore, the final decision should also be individualized.
ESD, endoscopic submucosal dissection.
Footnotes
Disclosure Statement
No competing financial interests exist.