
Abstract
Abstract
Purpose:
We retrospectively reviewed the perioperative outcomes of mini-laparoscopic procedure in the treatment of ureteropelvic junction obstruction (UPJO) in children and adults.
Methods:
From August 2009 to March 2017, 229 patients referred to our center to repair UPJO by mini-laparoscopic operation. In 203 cases, dismembered pyeloplasty was accomplished, while in other 26 cases, crossing aberrant vein division and crossing artery upward transposition were performed. A follow-up renal ultrasound was done on the cases 3 and 6 months after surgery. During the follow up period, if the patients had persistent hydronephrosis or sustained clinical complaints, diethylenetriamine pentaacetic acid (DPTA) scan was done to rule out the stenosis.
Results:
Among 229 patients, 140 patients were younger than 18 years (Range: 2 months-18 years old, mean: 3.01 ± 1.2 year) and others were scheduled as Adult (Range: 18–57 years old, mean: 35.12 ± 7.54 year). Total clinical and radiological success rates were 99.5% (228/229) and 86.5% (198/229) respectively. Mean operative times were 127.4 ± 20.3 minutes in dismembered pyeloplasty and 110.6 ± 12.7 minutes in crossing vessel transposition surgery. Mean of hemoglobin decreasing in children and adults was 0.3 ± 0.1 mg/dL; P = .26, and 0.5 ± 1.5 mg/dL; P = .13, respectively. Length of hospital stay was 3.41 ± 0.6 days in dismembered pyeloplasty and 2.1 ± 0.6 days in patients with crossing vessel transposition surgery. We did not suture the skin incision in the entrance site of 3 mm ports and the surgical scar was hardly visible after 6 months.
Conclusions:
The results of our study suggest that mini-laparoscopic pyeloplasty in adults and particularly in children is feasible, and it seems to be safe and effective in the treatment of UPJO. Furthermore, the patients tolerated the surgery well and they appreciated its outstanding cosmetic outcomes.
Introduction
Ureteropelvic junction obstruction (UPJO) is the most common cause of hydronephrosis that accounts for approximately $12 million in inpatient expenditure per annum. 1 Undiagnosed or left untreated UPJO can lead to significant kidney damage and the gradual loss of kidney function. Therefore, looking for optimal treatment with lowest morbidities is inevitable.
Nowadays, due to reduced morbidity and shorter hospital stays, open surgery has been largely replaced by laparoscopic approach for the treatment of UPJO.2,3 The introduction of smaller (miniaturized) laparoscopic instruments (≤3 mm) continues to further the field. The 2- and 3-mm ports are virtually incisionless and do not require suturing upon closure. The end result for the patient is essentially a “scarless” incision. Moreover, many consider that 2- or 3-mm incisions rather than 5- or 10-mm incisions reduce pain and translate to shorter hospital stays, faster recovery, and diminished wound morbidity. Mini-laparoscopic pyeloplasty (MLP) has been studied in children, but only some studies had reported this procedure in adult population, 4 respectively. Therefore, this study was designed to evaluate pure mini-laparoscopic procedure in treatment of UPJO to demonstrate the feasibility and results of this technique after 6 months of follow-up in children and adult populations.
Materials and Methods
Patients and setting
This was a retrospective study with prospective data collection, from August 2009 to March 2017, at the Department of Urology at Labbafinejad Hospital (ShahidBeheshti University of Medical Sciences,Tehran, Iran). Ethics Committee approval was obtained from Urology and Nephrology Research Center (UNRC), Shahid Beheshti University of Medical Sciences.
All patients referred to our center to repair UPJO through mini-laparoscopic operation were symptomatic (pain, nausea/vomiting, urinary tract infection, and hematuria) or asymptomatic (hydronephrosis grade ≥ II) obstruction, evaluated by diethylenetriamine pentaacetic acid (DTPA) scan to confirm UPJO. In this assessment, relative renal function and half-time (time at which 50% of radionuclide material is eliminated from upper tract) were calculated. Impaired renal function or a half-time greater than 20 minutes was considered an indication to intervene.
No age limitation was considered. Exclusion criteria for mini-laparoscopic surgery were BMI >30, history of abdominal surgery, concomitant with renal stone, and contraindications for laparoscopic surgery contain uncorrectable coagulopathy, intestinal obstruction, and significant abdominal wall infection. After registering demographic data, all patients were assessed preoperatively with complete blood count, urine culture, ultrasonography, serum creatinine, intravenous pyelography, and DTPA.
Surgical procedure
The patients received intravenous injection of prophylactic antibiotic 2 hours before the surgery consisting of first- or second-generation cephalosporin, unless in patients with past medical history of allergic reaction to penicillin or cephalosporin, who received aminoglycoside plus metronidazole. The initial trocar for the lense (5 mm) was placed at the umbilicus using an open access technique in semiflank position (no Veress needle was used) and under general anesthesia (Fig. 1). Two 3.5-mm trocars were placed along the midclavicular line and just below the xiphoid, respectively, for grasping and suturing. A transmesocolic approach was used in infants with left-side UPJO so that a 4-cm window in the mesentery of the descending colon was created. In right side cases, colon was reflected medially by peritoneal incision.

Semiflank position for mini-laparoscopic pyeloplasty.
Laparoscopic dismembered pyeloplasty (LP) was performed and a 3-Fr ureteral stent in children and 4.8-Fr in adults were placed over a guidewire through a subxiphoid miniport, manually by two graspers intracorporeally without using cystoscopy. The Foley catheter was placed and clamped before starting the surgery so the refluxed urine from full bladder went out from the Double-J catheter. It announced to us the correct place of the catheter and we confirmed it by ultrasonography postoperatively. We used 5-0 vicryl suture in children and 4-0 vicryl suture in adults for doing pyeloplasty. Thereafter, the mesenteric window was closed using 5-0 vicryl suture in transmesocolic approach. No suture was used to close the port sites in MLP, and only Steri-Strips were applied. At the end of procedures, corrugated drain was inserted. Urethral catheter was removed 2 or 3 days after the operation. Miniport sites were not closed, and only the 5-mm trocar at umbilicus was closed using 4-0 monocryl suture. The Double-J stent was removed 1 month after the operation. 5
In 26 patients, crossing vessels over the ureteropelvic junction were the main reason for obstruction and after releasing and carefully mobilizing these vessels, obstruction was resolved and renal pelvic was evacuated immediately. In these patients, renal pelvic dilation was decreased significantly under vision and we did not find any notable stenosis after realizing the vascular bundle. The aberrant small veins were cauterized and divided because usually these veins are short and hamper complete releasing. Upward transposition was done for crossing arteries as we reported previously.6,7 Otherwise, we performed dismembered pyeloplasty as described before.
Perioperative outcomes, including operative time, suturing time and Double-J stent insertion, decrease of hemoglobin, elevation of creatinine level, length of hospital stay, and complications like urinary leakage or hematoma, were assessed.
The patients were followed by clinical examination, urine culture, and ultrasonography at 3 and 6 months after surgery, and annually thereafter (6 months to 7 year, Mean was 3 year). Renewed intravenous pyelography and DTPA were only performed in patients with persistent hydronephrosis or sustained clinical symptoms (Fig. 2). We did not use computerized scan (CT scan) because of the risks of tissue damages and X-ray effects on gonads, unless in patients with renal stone in ultrasound. Clinical success was defined as relief of symptoms after 6 months. Radiological success was defined as decrease of hydronephrosis severity (hydronephrosis grade ≤ II). These patients, who had hydronephrosis, underwent DTPA for confirming UPJO.
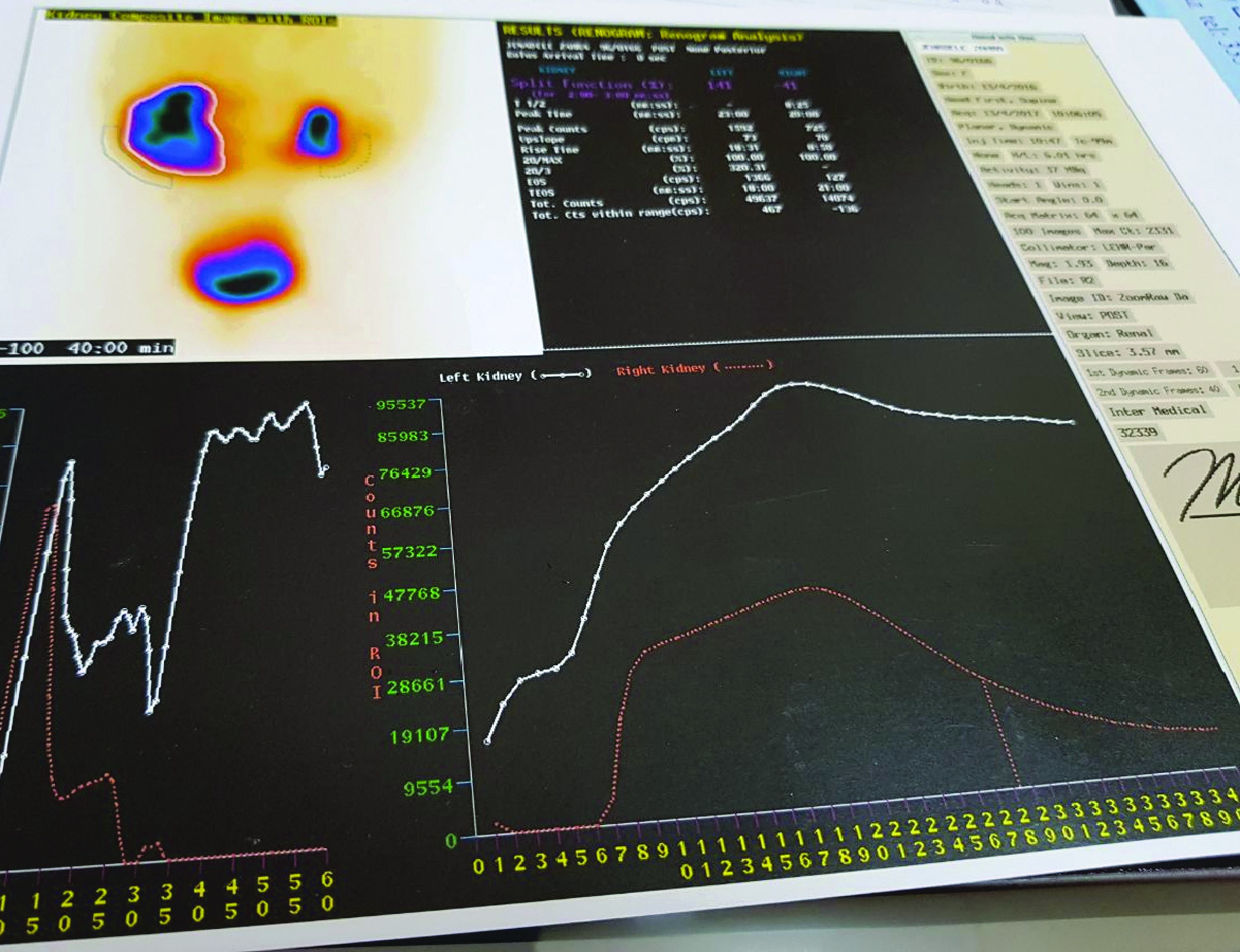
Preoperative DTPA scan showed obstruction. DTPA, diethylenetriamine pentaacetic acid.
Statistical analysis was performed with SPSS using the independent paired t-test for quantitative data and the chi-square test for qualitative variables.
Results
Baseline characteristics of patients are shown in Table 1.One hundred and forty patients were younger than 18 years and others were scheduled as Adult. Twenty six patients underwent crossing vessel transposition and pyeloplasty was done for 229 other patients. In 10 patients, crossing aberrant vessels were not the main reason of obstruction and renal pelvic did not compress after vessel transposition under vision, so dismembered pyeloplasty was done at the same session. We did not see any evidence of venous congestion after division of small aberrant vein.
Baseline Characteristics of Patients
One patient needed redo pyeloplasty, whereas the symptoms did not improve after nephrostomy insertion. Radiological success rate was estimated about 86.5% (198/229), and in these patients, obstruction was ruled out by DTPA scan. Mean operative times were 127.4 ± 20.3 minutes in patients who underwent dismembered pyeloplasty and 110.6 ± 12.7 minutes in crossing vessel transposition surgery. Suturing and Double-J insertion time were 29.32 ± 7.14 minutes. Postoperative Hb decreasing was 0.3 ± 0.1; P = .26 in children and 0.5 ± 0.15; P = .13 in adults.
Length of hospital stay was 3.41 ± 0.6 days in patients who underwent dismembered pyeloplasty and 2.1 ± 0.6 days in patients with crossing vessel transposition surgery. Febrile urinary tract infection was detected in two patients, which was treated by an antibiotic therapy. One child with active bleeding was explored 6 hours after surgery and mesenteric vessel damage was detected and repaired. A significant decrease in hemoglobin (>1 mg/dL) without clinical manifestations was detected in two patients who managed conservatively. Urinary leakage was found in eight patients. In six patients, urinary leakage were consequent of Double-J migration and were corrected endoscopically. Other two patients did not response to Double-J reinsertion, so they were treated with nephrostomy.
Discussion
This study showed that mini-laparoscopic approach as the treatment of UPJO in children and adults is feasible and safe.
Laparoscopic pyeloplasty was introduced in 1993 by Schuessler et al. 5 for the first time and developed as a successful approach to manage of UPJO very soon. During these years, all efforts were done to minimize the scar of the surgery (Fig. 4) without affecting the quality and success rate of procedure, so mini instruments and some new ways were introduced like Laparoendoscopic Single-Site Surgery Approach (LESS), Robotic-Assisted Laparoscopic Approach, and robotic laparoendoscopic single-site pyeloplasty. Laparoscopic suturing can be challenging in LESS, but this problem is not prevalent in MLP. If there is no specimen to be extracted like simultaneous renal stones, we do not need to enlarge the miniaturized entrances. Robotic surgery is so expensive and is not available in all centers.
There are some reports about MLP in children, but there are a few reports in adults. Simforoosh et al. 8 reported excellent surgical outcomes and significant better cosmetic results according to Patient Scar Assessment Questionnaire (PSAQ) in mini-laparoscopic approach in children with UPJO. Simforoosh et al. also reported a new approach to crossing vessels, crossing vein division, and upward transposition of the crossing artery to manage UPJO 6 and a long-term follow-up of these patients. 7
Hellstrom et al. had used a little different way for open surgery to manage the aberrant vessels in hydronephrosis. 9 Porpiglia et al. 4 evaluated 10 adult patients with UPJO who underwent MLP according to the Anderson-Hynes technique. They showed no patient had computed tomography evidence of hydronephrosis at 6 months after surgery and no functional obstructions were visualized with renal scintigraphy at 12 months after surgery. Our clinical success rate is in agreement with them; however, the radiological success rate was found to be lower in our study; it would be because we evaluated the patients with ultrasonography and not computed tomography. Ludwikowski et al. 10 used the BUlT Method for MLP in 40 infants with 83% complete success rate and improvement in 17%.Nevertheless, our study showed higher success rate, which might be due to surgeon experience.
The operation time in our study was in comparison of other studies, in which Double-J is inserted antegrade. However, in the studies in which Double-J is inserted endoscopically in a retrograde manner, total operating time was obviously higher (mean 214 minutes [93–360]).
Fiori et al. evaluated cosmetic results after MLP compared with standard laparoscopic pyeloplasty in an adult population and showed better cosmetic appearance in MLPs. 11 We had also acceptable cosmetic results in MLP (Fig. 3).

Surgical scars are hardly visible after 6 months.

In postoperative DTPA scan, the obstruction has been resolved.
There is some strength in our study. This is a large case series in a high-volume referral center. All of these operations were done by a single expert surgeon (N.S.) with at least 6 months of follow-up. Nevertheless, our study was done in retrospective manner, so there were no control groups for comparison (standard laparoscopic pyeloplasty or open pyeloplasty).
Conclusions
Mini-laparoscopic pyeloplasty is feasible and safe in treatment of UPJO regardless of age. It needs an experienced endourologist in fundamentals of laparoscopy, especially suturing and dissection because miniaturized instruments (lens, suction, and grasper) have some restrictions in special situations like bleeding or difficult dissection of fibrotic scar tissues.
Footnotes
Disclosure Statement
The authors disclose no commercial associations.