
Abstract
Abstract
Introduction:
Although the first laparoscopic gastrectomy was performed in 1991, there was a long delay until it was incorporated into the regular practice of western surgeons. In Brazil, there are only few case series reported and data on its safety and efficacy along with mid- and long-term results are desired.
Objective:
Present the mid-term results of laparoscopic gastrectomy with curative intent in the treatment of gastric adenocarcinoma and review the current evidence on the therapy of this neoplasia with the laparoscopic access.
Methods:
Patients who underwent D2 laparoscopic gastrectomy for gastric adenocarcinoma were retrospectively reviewed.
Results:
Sixty-nine patients met the inclusion criteria. The mean age was 59.2 years and the mean body mass index was 24.2 kg/m2. Subtotal gastrectomy was performed in 73.9%. The mean number of harvested lymph nodes was 36.7, increased lymph node count and shorter operative time were observed in the last 34 cases. Median hospital stay was 8 days. Postoperative complications occurred in 22 (31.9%) cases. Surgical mortality was 4.3%.
Conclusion:
Laparoscopic gastrectomy can be performed safely with excellent short- and mid-term results. As experience increases, surgical duration is reduced and lymph node count rises.
Introduction
The first laparoscopic gastrectomy was performed by Kitano et al. 1 in 1991. Although this surgical access has being employed progressively, there has been a delay in its popularization, especially in western countries.2,3 Among the reasons for this, it can be pointed out that: the access is technically demanding and the learning curve is extensive; expertise both in open gastric cancer surgery and in advanced laparoscopy are required; there is less applicability in the west due to the higher incidence of advanced cases and the prevalence of patients with high body mass index (BMI), which increases both the technical difficulty and the conversion rate; and the current scientific evidence are still inconclusive (studies are heterogeneous and biased, meta-analyzes have broad confidence intervals).4–7
In Brazil, laparoscopic gastrectomy in the treatment of gastric cancer has been performed more often only in the last decade, and there is a lack of reports about its learning curve and of mid- and long-term results. 3 The primary aim of this study is to report our experience performing D2 gastrectomy with curative purpose. Our secondary objective is to review the most current scientific evidence regarding its use.
Methods
This is a retrospective single center study. Data were collected through our prospective database. All cases operated between January 2006 and March 2018 were considered. Only patients with gastric adenocarcinoma submitted to laparoscopic resection with D2 lymphadenectomy were included. Exclusion criteria were: patients who lost follow-up; those with previous surgeries on the stomach; T4b lesions; and those who underwent palliative surgery. Cases converted to conventional access were also excluded, allowing the survival analysis of those patients effectively submitted to the laparoscopic access.
Preoperative evaluation included laboratorial test, upper digestive endoscopy with biopsy, computed tomography scan (chest, abdomen, and pelvis), and endoscopic ultrasound in selected cases.
The extension of gastric resection (total or partial) was based on the location of the tumor to obtain free margins. All patients were operated by high-volume surgeons specialized in the treatment of gastric cancer. The surgical technique, extension of the resection, and dissected lymph node stations followed the recommendations of the Japanese Gastric Cancer Association. 8
The surgical specimen was examined in the operating room and lymph node stations were freshly dissected. Fixation was performed in 10% buffered formalin solution or Carnoy's solution for 24–48 hours and then the lymph nodes were retrieved.9,10 Surgical specimens were evaluated according to the protocol of the College of American Pathologists, 11 and the 7th edition of the TNM used for staging. 12
Immunohistochemistry for cytokeratin (CK AE1/AE3) was selectively used to increase the detection of hidden lymph node metastases. 13
Patients were classified as proposed by the American Anesthesiology Association 14 (ASA) and according to their comorbidities by the Charlson's classification. 15 Perioperative complications were described according to the Clavien–Dindo classification. 16 Clavien complications ≥ III were considered as severe. Surgical mortality was considered when death occurred up to 30 days after surgery or during hospital stay.
The hospital length of stay, number of resected lymph nodes, surgical margins, overall survival, and disease-free survival were analyzed. Follow-up occurred on a quarterly basis in the first year and every 6 months in the following years. Tests and exams for recurrence were performed based on the presence of symptoms or complications. Absence in medical appointments for more than 12 months was considered as loss of follow-up.
Statistical analysis
Statistical analysis was performed using SPSS software version 20.0 (SPSS, Chicago, IL). Chi-square test was used for categorical variables and the t-test for continuous variables. The correlation between age and length of hospital stay was assessed using the Pearson correlation test. Survival was analyzed using the Kaplan–Meier method and t curve comparison determined by the log-rank test. Binary logistic regression was used to evaluate the odds ratio (OR) for the occurrence of major complications. For the OR calculation, BMI values were divided into quartiles and the upper quartile used as cutoff. Multivariate analysis was performed for those variables with significance in the univariate analysis. Survival was considered in months, from surgery until the date of death/relapse/last visit as outpatient. Results were considered significant when P < .05.
Results
Clinical features and surgical treatment
Of 622 GC patients operated with curative intent during the period studied, 69 patients met all inclusion criteria. Their characteristics are shown in Table 1. The mean age was 59.2 years, with male predominance (52.2%). The mean BMI was 24.2 kg/m2. In most patients, comorbidities were absent or mild/compensated (94.2% were classified as ASA ≤II). Three patients (4.3%) underwent neoadjuvant treatment. Subtotal gastrectomy was performed in 73.9% of the cases. All patients underwent D2 lymphadenectomy and Roux-en-Y reconstruction. Gastrojejunostomy and esophagojejunostomy were both performed in a side-by-side fashion with linear stapler. Peritoneal cytology was negative for all patients and free margins (R0) were obtained in all cases. Surgical duration decreased as case number increased (Fig. 1). Adjuvant therapy was performed in 25 patients (36.2%).
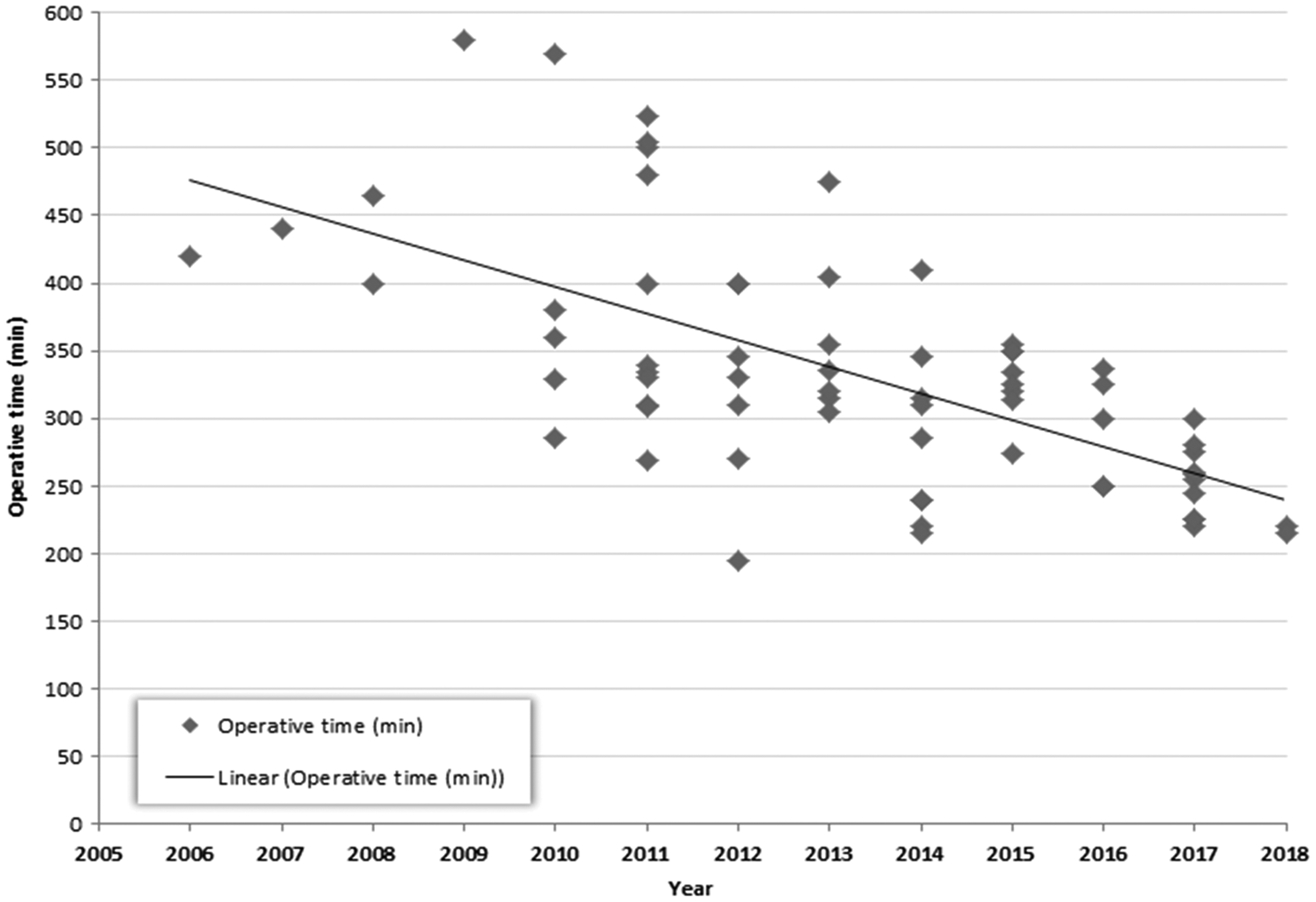
Operative time according to case number (n = 69).
Patients' Demographics and Surgical Procedures
ASA, American Anesthesiology Association; BMI, body mass index.
Pathological features
Most lesions were from the distal portion of the stomach (73.9%) and classified as Lauren's intestinal type (42.0%). The mean tumor size was 3.3 cm (ranging from 0.2 to 17.5 cm) and the majority had ulcerated macroscopic appearance (39.7%). The mean number of lymph nodes dissected per patient was 36.7. Lymph node count increased as the case number rose (Fig. 2).
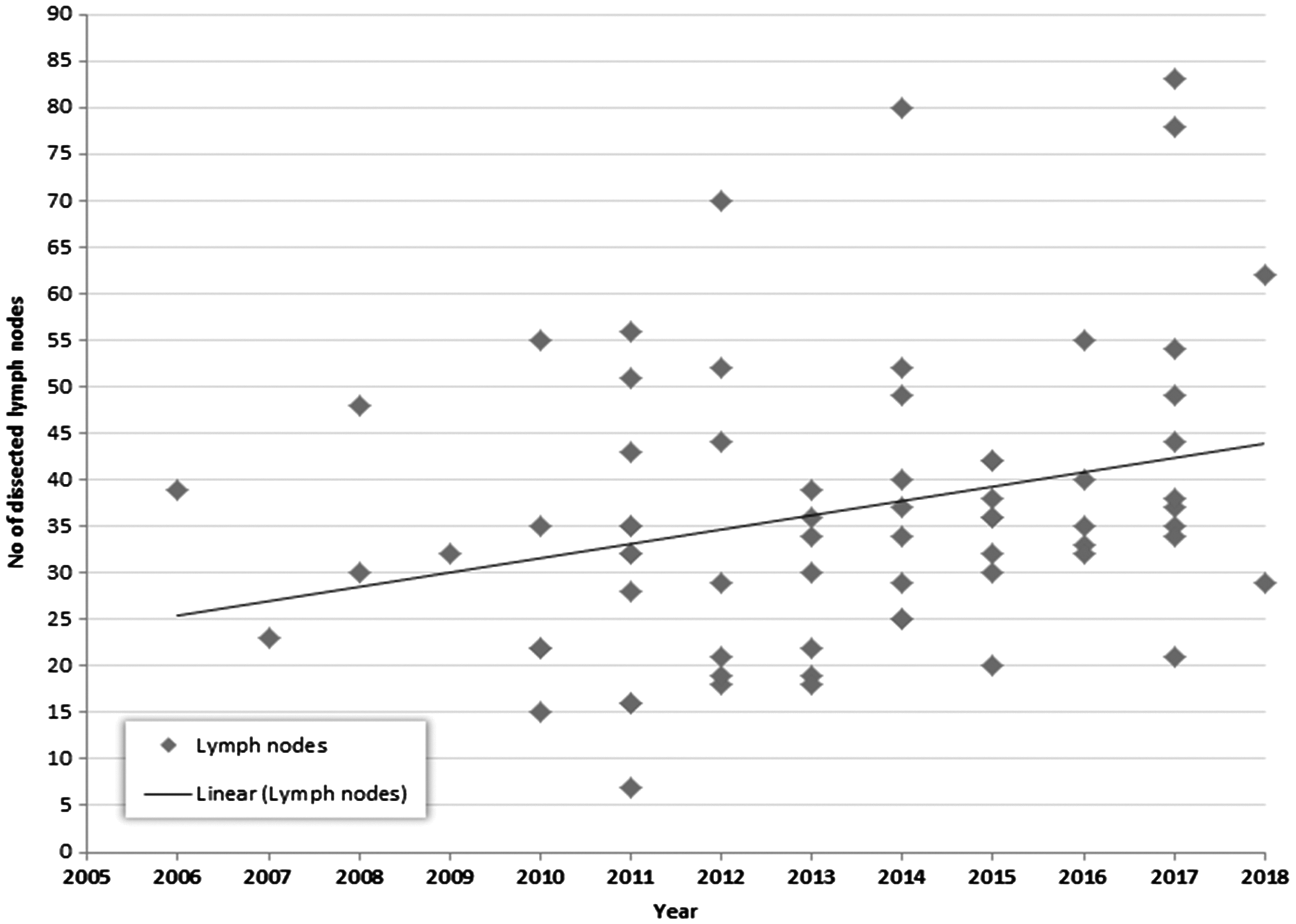
Lymph node count according to case number (n = 69).
T1 lesions were predominant (55.1%: 18 pT1a and 20 pT1b). Lymph node metastasis was detected in 30.4% of cases (6 pN1, 5 pN2, 5 pN3a, and 5 pN3b). The pathological characteristics of the studied population are described in Table 2.
Pathological Features
Postoperative data
The median hospital stay was 8 days (ranging from 4 to 37 days) and positive correlation between age and hospitalization was observed (r = 0.391, P = .001).
Postoperative complications were observed in 22 (31.9%) patients (Table 3). Seven patients had two or more complications.
Incidence and Type of Complication According to Clavien–Dindo Classification (Number of Cases as Per Complication)
Minor complications (Clavien–Dindo grades I and II) occurred in 10 patients. Twelve (17.4%) had severe complications (≥III) and surgical mortality was 4.3% (3 patients). All deaths were in males: 1 due to respiratory complications in a 65-year-old morbidly obese patient (BMI = 43.1 kg/m2), ASA III, submitted to total gastrectomy (pT2pN0); 1 due to duodenal stump fistula in 79-year-old ASA II patient submitted to subtotal gastrectomy (pT1apN0); 1 bronchoaspiration due to intestinal obstruction in a 58-year-old ASA I patient submitted to total gastrectomy (pT4apN2).
Severe complications were associated with older age (68.1 versus 57 years, P = .002) and higher anesthetic risk (ASA III/IV comprised 25% versus 1.8%, P = .015). The hospitalization time of these patients was also longer: 23.9 versus 8.9 days (P < .001).
ORs for major complications according to clinical variables are presented in Table 4. In univariate analysis, age over 65 years (P = .03) and ASA III/IV (P = .016) were related to greater chance for severe complications. In multivariate analysis, ASA was an independent risk factor for major complications (P = .03).
Univariate and Multivariate Analyses for the Risk of Major Complications (Clavien–Dindo ≥ III)
Bold numbers signify statistically significant values.
ASA, American Anesthesiology Association; BMI, body mass index.
Comparing the first 35 cases with the last 34 (Table 5), patient`s BMI was higher in the last cases, whereas complications were similar.
Comparison of the First 35 Laparoscopic D2 Gastrectomy Cases Versus the Last 34
Bold numbers signify statistically significant values.
BMI, body mass index; SD, standard deviation.
Follow-up and survival
At an average follow-up of 35 months (median of 30.1), 11 (15.9%) patients died and 6 (8.7%) had recurrence. Disease-free survival and overall survival during the follow-up was 90.3% and 84.1%, respectively. Regarding the site of recurrence, in 3 patients it was regional, 1 in the peritoneum and 2 had distant metastasis (1 pulmonary, and 1 liver and ovaries). The survival curves are presented in Figure 3.
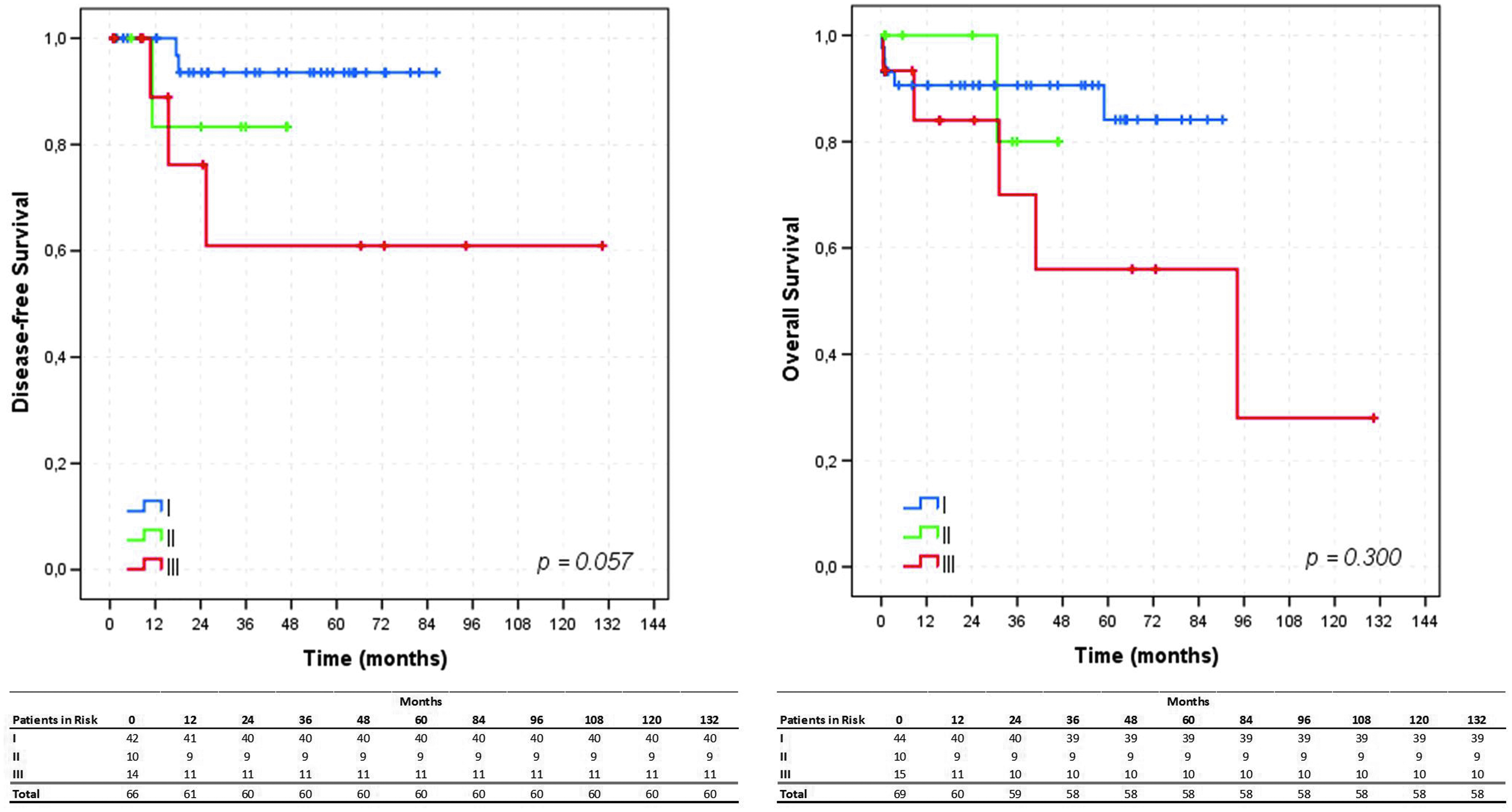
Survival according to TNM staging (n = 69).
Discussion
The access
The advantages of the laparoscopic access in abdominal surgery are undoubtful: lower rate of wound complications, less pain, better cosmetic result, shorter hospitalization time, etc.7,17–21 But the main issue of using this access for gastric cancer is whether the same oncological results of the open surgery can be obtained. Initially, laparoscopy was indicated for early gastric cancer in the distal stomach, since the prognosis is favorable and the procedure simpler (lymphadenectomy and reconstruction are considerably less complex or morbid). 8
Distal gastrectomy in early gastric cancer proved to be safe, with lower intraoperative bleeding, lower postoperative pain, equivalent number of resected lymph nodes, lower short-term morbidity, and similar 5-year survival.5,6,20,22 So, it became widely accepted and the long-term results of two large studies (KLASS 1, n = 1415 and JCOG 0912, n = 920) will confirm these findings.23,24
As for advanced gastric cancer, preoperative staging inaccuracy led to the resection of a significant number of these cases. 25 In addition, experienced surgeons, who surpassed the learning curve and were comfortable with the method, began to indicate the procedure for these patients.20,26 As some studies demonstrated lower lymph node count with the laparoscopic access, suggesting an inferior lymphadenectomy, the main concern in advanced disease is the risk of lower survival.5,6,27 However, two recent meta-analyzes (n = 2.596 and 1.456) have shown that with adequate patient selection, well-trained teams obtain the same number of lymph nodes and the same survival compared with the open access.18,19 It was also demonstrated in these studies that laparoscopic access resulted in less analgesic requirements, faster oral intake, lower hospitalization, lower morbidity, and similar rates of reoperations and mortality. It should be emphasized that there is always a selection bias, even in randomized studies, since extremely advanced cases are not considered for inclusion. Three multi-institutional studies should clarify the safety and efficacy of laparoscopy in advanced gastric cancer: KLASS 2, JLSSG 0901, and CLASS 01.20,28,29
Type of gastrectomy and reconstruction
While in the eastern world, more restricted resections are performed, in western countries, where tumors are more advanced and patients less favorable (e.g., greater visceral obesity), the surgical option is usually for total or distal gastrectomy. Total gastrectomy is less performed, since proximal tumors are less frequent and it is technically more demanding due to the esophagojejunostomy. Additionally, there is the controversial matter as whether this anastomosis has a greater risk of leakage when performed by laparoscopy. A multicenter cohort study with paired analysis of 753 patients with early gastric cancer noted that although overall and disease-free survival were similar for open and laparoscopic total gastrectomy, anastomotic complications (8% versus 4.2%, P = .015) and deaths in the recent postoperative period (1.6% versus 0.2%, P = .045) were higher in the laparoscopic cases. 30 A recent meta-analysis with 2.560 patients, also observed more complications in the laparoscopic esophagojejunostomy; however, this was not statistically significant (P = .08). 31 As this anastomosis is difficult to perform, it is likely that the learning curve influenced the results reported so far. In addition, it seems to be a greater risk of stenosis (8.3% versus 1.8%) and fistula (4.7% versus 1.1%) when it is made with circular staplers. 32 Our preference is for intracorporeal side-to-side anastomosis with linear stapler, as described elsewhere. 33
Regarding reconstruction in subtotal gastrectomy, our choice is for intracorporeal Roux-en-Y gastrojejunostomy with linear stapler. A prospective, randomized study has shown that Roux-en-Y has a lower incidence of biliary reflux after 12 months, with quality of life and nutritional status similar to Billroth I and Billroth II+Braun anastomosis. 34 In addition, Roux-en-Y has a lower incidence of biliary esophagitis and stump gastritis. 35
Patients
We chose to report only laparoscopic D2 gastrectomy for gastric adenocarcinoma since, in our knowledge, there is no Brazilian publication addressing survival after this procedure.
Cases in this series were favorable: small lesions (mean size of 3.3 cm), predominantly distal tumors (73.9% were subtotal resections), most were early gastric cancer, generally patients had good clinical status, and low BMI by national standards.
Regarding the results, the number of lymph nodes, complications, and mortality rates are all similar to open cases from our institution and to the national multi-institutional report.3,25,36,37
To analyze the learning curve, we divided patients in two groups (the first 35 cases versus the last 34), lymph node count significantly increased over time and the operative duration decreased. This is in accordance to what other authors observed.38–40 Indications for laparoscopic access also increased in the second period: patients had higher BMI and cases were more advanced (but this was not statistically significant, probably due to the low n; P = .056 for pN+). Major complications in both groups occurred in 22.9% and 11.8%, respectively, but again this was not significant. Total complications and major complications are also similar to previous literature reports.2,40
Regarding severe complications (Table 4), the univariate analysis showed a greater risk for patients over 65 years of age and ASA > II. In multivariate analysis, ASA was the only independent risk factor for the occurrence of these complications.
The margins were free of neoplasia in all cases, indicating the quality of the surgery and the correct use of methods to locate the lesion: preoperative identification by endoscopy and CT scans, endoscopic marking before the procedure, intraoperative identification of the lesion (by haptic touching, visualization of serosal irregularities, or by intraoperative endoscopy), and by intraoperative frozen section examination in specific cases. Free margins also suggest selection bias, since borderline and advanced cases were referred for open surgery. Other evidence of patient selection was oncotic cytology, collected before dissection, negative in all cases. 41
Regarding specimen retrieval, our preference is for the Pfannenstiel incision. In the presence of abdominal hernias, we regularly remove the specimen through the hernia defect and repair it. This does not add morbidity to the procedure. 42
Another quality indicator was related to overall survival and disease-free survival, which when stratified by stages were favorable and comparable to literature reports with both open and laparoscopic accesses.40,43,44
It is important to emphasize that the team's commitment was always with the oncologic result and not the access.
Limitations
Despite the prospective data collection, there are the limitations of a retrospective study. The number of patients enrolled is relatively small and some cases have a short follow-up, which limits some analyses. In addition, there is no control group submitted to the standard treatment (open access).
Conclusions
Laparoscopic D2 gastrectomy can be performed safely and efficiently with excellent results in the short and mid term. Adequate patient selection and oncologic staging are key to achieving favorable outcomes. As experience increases, surgical duration is reduced and lymph node count rises.
Footnotes
Disclosure Statement
No competing financial interests exist.