
Abstract
Abstract
Background:
The application of laparoscopic hepatectomy is gaining momentum. However, the safety and efficacy of laparoscopic right hepatectomy (LRH) on hepatocellular carcinoma (HCC) are yet to be adequately evaluated. We aimed to assess the surgical and oncological outcomes of LRH for HCC by comparing it with open right hepatectomy (ORH).
Materials and Methods:
Data of patients who underwent hepatectomy for HCC from May 2007 to January 2018 in our hospital were obtained. Baseline characteristics, postoperative recovery, and survival outcomes were compared. One-to-one propensity score matching (PSM) was used to minimize selection biases by balancing factors, including age, sex, preoperative therapy, tumor size, and pattern.
Results:
The original cohort included 109 patients (LRH, 41 patients; ORH, 68 patients). Of the 41 patients who underwent LRH, 8 patients (19.5%) required conversion to laparotomy. The overall morbidity was 19.5%, and no mortality in LRH was noted. After PSM, LRH was associated with a tendency of prolonged operative time (255.5 ± 93.4 minutes versus 225.9 ± 39.8 minutes, P = .08) and less intraoperative blood loss [300 (100–1200) versus 500 (200–2000) mL, P < .01]. LRH showed up a trend of less overall morbidity without statistical significance (18.4% versus 26.3%, P = .41). Moreover, the 3-year overall and disease-free survival did not differ significantly between the groups during a median follow-up of 19 (3–58) months for the LRH group and 23 (3–97) months for the ORH group.
Conclusions:
LRH can be performed as safe and effective as ORH for HCC in regard to both surgical and oncological outcomes. LRH holds the benefit in less intraoperative blood loss and appears to achieve less postoperative morbidity, which could serve as a promising alternative to ORH in selected individuals.
Introduction
Although the incidence of hepatocellular carcinoma (HCC) has decreased, HCC is still the fifth common malignancy and the third leading cause of cancer-related deaths worldwide. 1 HCC represents a great challenge for health care providers and requires a multidisciplinary approach in which surgery remains the primary curative treatment for patients without distant metastasis. 2 Since laparoscopic hepatectomy (LH) was first reported in 1996,3,4 it has been rapidly adopted globally. Thousands of LHs have now been performed worldwide for the treatment of benign diseases and malignancies and for living donor hepatectomy. 5 Majority of HCC patients have underlying liver diseases, such as liver cirrhosis and viral hepatitis, which inevitably damage liver function. Theoretically, a minimally invasive surgery preserves the integrity of the abdominal wall and minimizes surgical trauma, thereby making it an ideal surgical approach for HCC patients. 6 Recently, increasing series highlighted the superiority of LH over open hepatectomy for HCC patients; LH was characterized by less blood loss, shorter hospital stay, lesser morbidity, and quicker recovery while maintaining comparable oncologic safety. 7 Studies also argued that nonanatomic or minor hepatic resection could maximally preserve the surrounding nontumorous parenchyma and decrease postoperative liver failure incidence.8,9
Laparoscopic minor hepatectomy is technically easier, but is limited in eliminating intrahepatic recurrence, which is the most common type of recurrence and usually develops secondary to portal venous invasion. Moreover, a limited liver resection would result in the lack of an adequate surgical margin for lesions at posterosuperior liver segments or for large HCC. 10 Thus, major hepatectomy is preferable to minor resection for patients with multiple large neoplasms or those with sound functional reserve.11–13 However, laparoscopic major anatomic liver resections, especially right hepatectomy, which is technically demanding, were initially considered unfeasible because of mobilization of a heavy fragile organ, transection of a bulky parenchyma, and major vascular dissection, which is associated with the risk of major vessel injury. Currently, comparative studies restricted to right hemihepatectomy for HCC are rarely published. 14 In this study, we evaluated the feasibility and safety of laparoscopic right hepatectomy (LRH) by comparing its short- and long-term clinical outcomes with those of open right hepatectomy (ORH) through a propensity score–matched analysis to minimize selection bias.
Materials and Methods
Patients
This study was approved by Zhejiang University's Ethics Committee. Data were acquired from patient medical records and a prospectively maintained surgical database of all patients who had undergone hepatectomy. The study period was from May 2007 to January 2018. The diagnosis of HCC was mainly based on preoperative imaging, specifically triphasic computed tomography (CT). In selected cases, we performed magnetic resonance imaging (MRI) to detect additional lesions. Inclusion criteria were as follows: pathology confirmed HCC, right hepatectomy performed with the intention to cure, and Child–Pugh class A liver function without signs of severe portal hypertension. Exclusion criteria were the following: patients with cholangiocarcinoma, mixed-cell carcinoma, or other tumors; patients with imaging evidence of extrahepatic metastasis or presence of main portal vein or inferior vena cava cancer embolus; patients with recurrent HCC; and patients who had emergency operation due to traumatic or spontaneous tumor rupture.
Data on patient demographics, surgical procedure, and postoperative outcomes were compared. Patients were evaluated in an intention-to-treat (ITT) manner. Surgical data, including conversion, operative time, estimated blood loss, intraoperative blood transfusion, length of hospital stay, morbidity, and mortality, were compared. Based on the complication reporting system of Memorial Sloan-Kettering Cancer Center, 15 postoperative complications are categorized into medical complications (pleural effusion; renal, respiratory, cardiovascular, or metabolic events; arrhythmia; cerebrosis; and deep vein thrombosis) or surgical complications (bleeding events, any complication that required reoperation, wound complications, liver-specific complications, delayed gastric emptying, and ileus). The severity of postoperative complications was based on the Clavien-Dindo classification. 16 For the LRH group, we compared the effect of conversion to laparotomy with that of complete resection under laparoscopy.
Surgical procedure
LRH was performed as described previously. 17 Briefly, the patient was placed in the supine and 30° reverse Trendelenburg position with the right upper abdomen elevated. The trocar ports were generally placed in the abdomen, as previously described. Pneumoperitoneum was established at a pressure of 13 mm Hg. The right lobe of the liver was fully mobilized after dividing the falciform ligament, round ligament, caudata ligament, peritoneum reflection anterior to the inferior vena cava, right triangular ligament, and right coronary ligament. The anterior surface of the inferior vena cava was clearly exposed, and the short hepatic veins were ligated (Fig. 1A). Then, the lesser omentum was dissected, and an elastic tape was subsequently passed around the right hepatoduodenal ligament, which was not routinely used and was only applied to control hemorrhage in some cases. The portal pedicles were bluntly dissected. The right hepatic artery and the right branch of the portal vein were visualized and clamped (Fig. 1B). The resection line was marked along the ischemic line (Fig. 1C). The right pedicle was transected using an endoscopic linear stapler (Fig. 1D). Hepatic parenchymal transection was performed using Peng's Multiple Operative Dissector or an ultrasonic scalpel. Subsequently, the second porta hepatis was dissected. The right hepatic vein was identified and divided (Fig. 1E). After the right lobe of the liver was removed and retracted, a careful assessment for any suspected bleeding and bile leakage was performed (Fig. 1F).
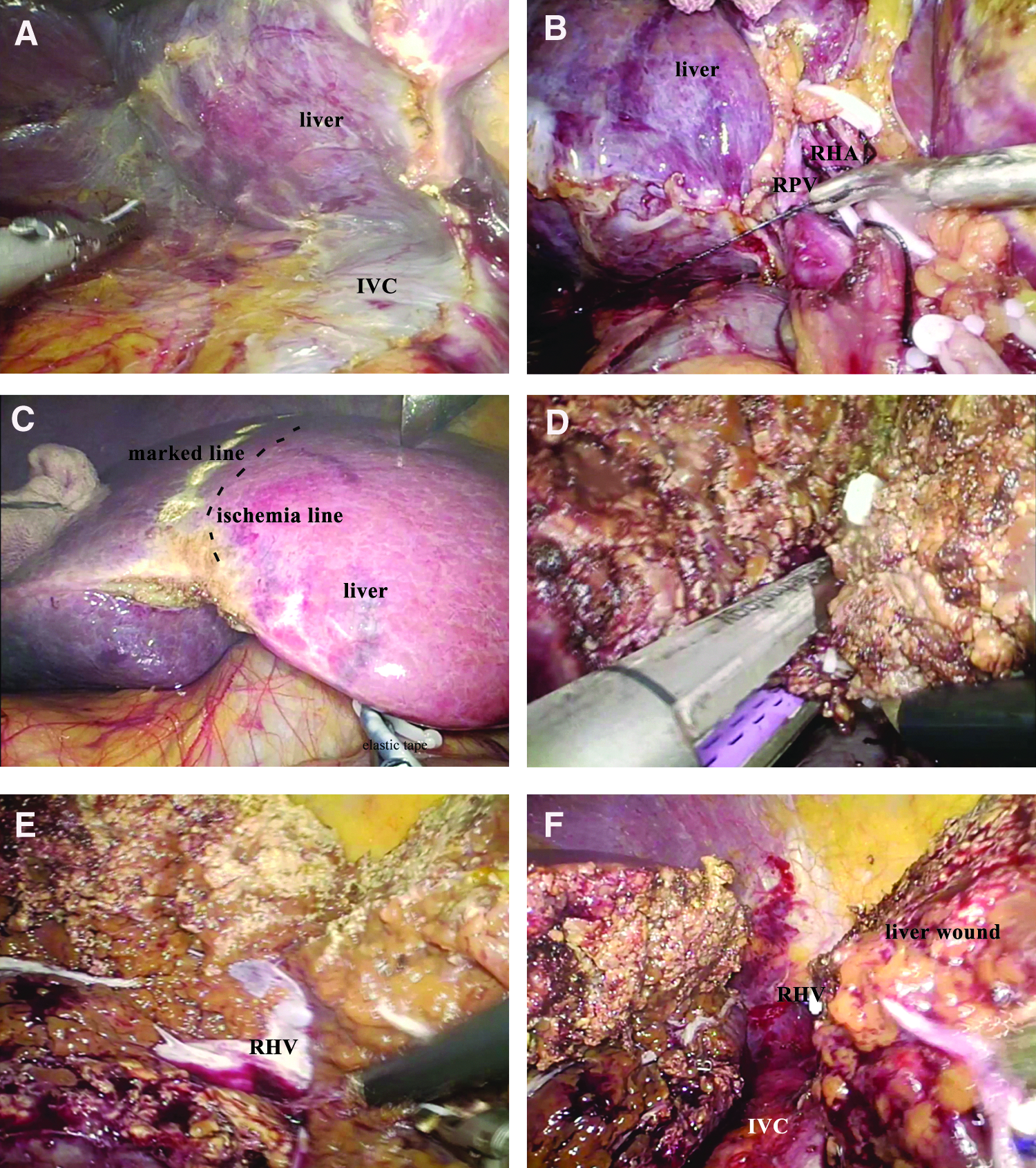
Representative photographs and laparoscopic views of LRH:
Follow-up evaluation
Postoperative follow-up began at 1 month after the operation, followed by once every 3–6 months or whenever the patients presented symptoms of or were suspected to have tumor recurrence. Patients who failed to attend a follow-up visit were contacted by telephone. Routine blood tests, liver function tests, and ultrasonography were performed. CT or MRI was performed when indicated clinically. Treatment options for tumor recurrence included repeated liver resection, transcatheter arterial chemoembolization (TACE), local ablation therapy, and targeted therapy, depending on tumor characteristics and the patient's liver function.
Statistical analyses
To minimize selection biases, 1:1 propensity score matching (PSM) was performed using a logistic regression model and the following covariates: age, sex, preoperative TACE, tumor size, and pattern. Patients for whom the propensity score could not be matched exactly were excluded. Continuous variables with a normal distribution are reported as mean ± standard deviation. Variables not fitting a normal distribution are presented as median (range). Continuous data were compared by Student's t-test if normally distributed; otherwise, the Mann–Whitney U test was used. Chi-square analysis or Fisher's exact test was used to compare categorical variables. Survival curves were compared between groups using the log-rank test. Disease-free survival (DFS) was defined as the time from surgery to the time of HCC recurrence, and overall survival (OS) was defined as the time from surgery to death of any cause. All statistical tests were two sided, and differences were considered significant when P < .05. All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY).
Results
Clinicopathological characteristics before and after matching
During the study period, two surgeons performed 41 cases of LRH for HCC, and 68 cases of ORH were performed by 5 surgeons. After PSM, 38 patients for the LRH group and 38 patients for the ORH group were included in the final analysis. Clinicopathological characteristics of the two groups before and after PSM are summarized in Table 1. Before matching, the mean age and percentage of male patients tended to be higher in the LRH group. Moreover, the ORH group tended to have higher preoperative TACE proportion, as well as larger tumor size and a multifocal pattern. After matching, all of these characteristics, which could influence surgical results, were comparable between the matched groups (Table 1).
Clinicopathological Characteristics Before and After Matching
Values were showed as mean (standard deviation) and tested by Student's t-test.
Including heavy smoker.
Values were showed median (range) and tested by Mann–Whitney U test.
Pulmonary comorbidity included heavy smoker.
AFP, alpha fetoprotein; ALB, albumin; ALT, alanine transaminase; ASA, American Society of Anesthesiologists; AST, aspartate transaminase; BCLC, Barcelona clinic liver cancer; BMI, body mass index; ICG-R15, indocyanine green retention rate at 15 minutes; LRH, laparoscopic right hepatectomy; ORH, open right hepatectomy; PLT, platelet; PT, prothrombin time; TACE, transcatheter arterial chemoembolization; TB, total bilirubin.
Operative findings and postoperative clinical course before and after matching
Operative findings and postoperative clinical course are shown in Table 2. For the 41 LRH cases, conversion to open surgery was necessary in 8 cases (19.5%) because of intraoperative bleeding from the inferior vein cava (n = 2) and middle hepatic vein (n = 1), advanced tumor that required difficult intrahepatic vascular resections (n = 2), hepatic portal adhesions due to a history of gastrectomy (n = 1) and preoperative TACE (n = 1), and suspected portal vein involvement (n = 1). Before PSM, the LRH group had a comparable mean operative time (250.2 ± 91.9 minutes versus 233.7 ± 44.7 minutes, P = .28), but less median blood loss (300 versus 600 mL, P < .01), than the ORH group. After PSM, data showed a tendency of longer mean operative time in the LRH group with marginal difference (255.5 ± 93.4 minutes versus 225.9 ± 39.8 minutes, P = .08), and still significantly less median blood loss (300 versus 500 mL, P < .01). Before PSM, 9 (21.9%) and 28 (41.2%) cases in the LRH and ORH groups, respectively, required intraoperative transfusion. After PSM, the intraoperative transfusion rate was not significantly different between the groups (10.5% versus 23.7%, P = .13).
Operative Findings and Postoperative Clinical Course Before and After Matching
Values were showed mean (standard deviation) and tested by Student's t-test.
Values were showed median (range) and tested by Mann–Whitney U test.
Repeated cases not included.
LRH, laparoscopic right hepatectomy; ORH, open right hepatectomy.
The postoperative morbidity and mortality are presented in Table 2. Two in-hospital mortalities in the ORH group were noted: a 62-year-old male patient who developed liver failure, hepatic encephalopathy, and renal failure died of multisystem organ failure on postoperative day 30; on postoperative day 104, a 33-year-old male patient who had subphrenic collection and abdominal abscess requiring another intervention and whose liver function worsened died of multisystem organ failure secondary to sepsis. For specific complications, although several common complications were more frequent in the ORH group (after PSM: ascites 7.9% versus 10.5%, liver failure 0.0% versus 5.3%, hemorrhage 2.6% versus 7.9%, and pleural effusion 5.3% versus 7.9%), the difference between the groups did not reach the statistical significance. Before PSM, the overall morbidity in the LRH group was lesser than that in the ORH group; however, the difference was not statistically significant (19.5% versus 30.9%, P = .19). The overall morbidity also did not reach statistical significance after PSM (18.4% versus 26.3%, P = .41). Based on the Clavien-Dindo classification, no significant differences in the severity of complications between the two groups were found (P = .65).
Comparison of completely laparoscopic resection with conversion to open surgery
As shown in Table 3, except for preoperative platelet, no significant differences between the complete laparoscopy and conversion groups with regard to age, sex, body mass index, preoperative TACE, the remaining preoperative blood tests, Barcelona clinic liver cancer stage, and tumor size and pattern were found. For surgical outcomes, operative time was comparable between the complete laparoscopy and conversion groups. Blood loss was significantly less in the former, as was intraoperative transfusion. The median postoperative hospital stay was longer in the conversion group. The overall morbidity (P = .17) and the severity of complications (P = .06) tended to be higher in the conversion group.
Comparison of Completely Laparoscopic Resection with Conversion to Open
All continuous data were showed as median (range) and compared by Mann–Whitney U test due to abnormal distribution.
AFP, alpha fetoprotein; ALB, albumin; ALT, alanine transaminase; AST, aspartate transaminase; ICG, indocyanine green; PLT, platelet; PT, prothrombin time; TACE, transcatheter arterial chemoembolization; TB, total bilirubin.
Recurrence and survival before and after matching
The mean follow-up was 19 (3–58) months for the LRH group and 23 (3–97) months for the ORH group. Survival data were available for all LRH patients, whereas five patients in the ORH group were lost to follow-up. Intrahepatic recurrence was the most common initial recurrence site. Table 4 and Figure 2 show the differences in recurrence and survival. Three-year DFS and 3-year OS both before and after PSM were not significant between the groups.
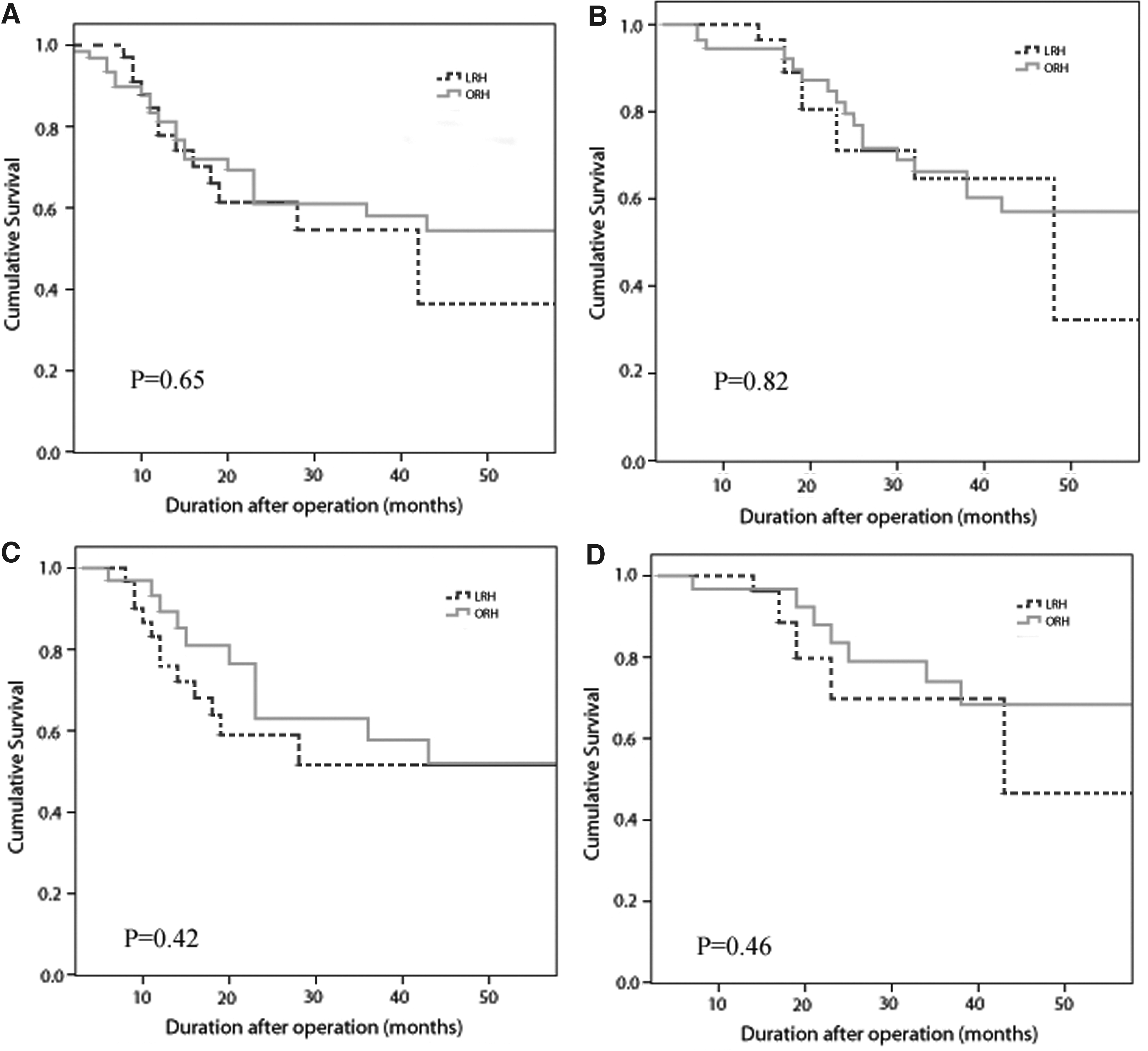
Kaplan–Meier survival curves.
Recurrence and Survival Before and After Matching
Two in-hospital deaths in ORH group were not calculated in survival analysis.
DFS, disease-free survival; LRH, laparoscopic right hepatectomy; ORH, open right hepatectomy; OS, overall survival.
Discussion
This study suggests that LRH is technically feasible and safe. In this study, the duration of operation is slightly longer in LRH than in ORH. LRH and ORH had comparable mortality and 3-year survival rates. Intraoperative blood loss was less in LRH than that in ORH before and after PSM. There was no statistically significant difference regarding the postoperative morbidity between LRH and ORH, whereas a trend was observed that LRH was superior (after PSM, 18.4% versus 26.3%). The less blood loss and complications could consider convictive evidence that favored LRH. The results could be a valuable addition to the existing data in the literature for several reasons. First, LRH could be used in several diseases, including hepatolithiasis, benign tumors, HCC, and colorectal cancer liver metastasis. Exclusively studying regarding LRH for HCC is appropriate to determine differences in surgical outcomes. Second, although controversies in the feasibility and safety of LRH for HCC exist, studies focusing on this topic are limited. Thus, direct comparisons clearly have value.
In this ITT analysis, the conversion rate (19.5%) was apparently higher than the conversion rates of laparoscopic minor or combined resection for HCC (0%–9.4%).18–22 The main reason for the conversion of nonanatomic or minor resection is insufficient tumor margin, 23 while that for the conversion of major resection was related to uncontrollable hemorrhage or failure to progress. A high conversion rate indicates that LRH remains a challenging procedure. de'Angelis et al. reported that in 36 cases of laparoscopic resection for HCC, three conversion patients underwent LRH, and all were due to intraoperative hemorrhage. 24 Komatsu et al. reported a conversion rate of 42.9% for LRH for HCC. 25 The primary causes were hemorrhage and failure to recognize hepatic pedicles and severe adhesions. Similarly, by reviewing our converted patients, we found that the conversions generally were due to hemorrhage that is difficult to control or suspected major vascular involvement and severe adhesions. Cirrhosis and preoperative treatment are significant risk factors for conversion. 25 The former leads to increased risk of bleeding and increased difficulty of parenchymal transection, while the latter, such as TACE, could result in adhesions.
Laparoscopic surgery could be a suitable technique for anatomic hepatectomy. The essential steps and principles of laparoscopic surgery are in accordance with those of open surgery. In theory, the magnified surgical vision and meticulous manipulation allow safe dissection of portal pedicles, as well as control and division of the supply vessels. In our institution, laparoscopic selective right inflow occlusion (LSIO) is routinely performed. LSIO could nearly have the same hemostasis effect as that of total vascular occlusion (Pringle maneuver). With LSIO, ischemia–reperfusion injury is attenuated, and the compensatory capacity of the remnant liver is secured. A proper transection line could be precisely achieved to ensure safe resection margins and preserve the vascular structures of the remnant liver with minimal blood loss. LSIO with separate isolation of the hepatic artery, duct, and portal vein is better than the Glissonian approach as blunt maneuvers of the Glissonian pedicle are technically difficult because of the limited angulations of laparoscopic instruments, which in turn could be dangerous. 26 However, for severe hilar adhesion cases, the Pringle maneuver is recommended because of the increasing difficulty in vessel dissection and the risks for uncontrollable hemorrhage. Our study demonstrated less blood loss in LRH even though there were several conversion cases with extremely high blood loss in LRH group. The advantage of less blood loss in LRH was more obvious when data on conversion were omitted (data not shown).
Our data showed a tendency of prolonged operative time in LRH (after PSM, 255.5 ± 93.4 minutes versus 225.9 ± 39.8 minutes, P = .08). Conversely, previous studies demonstrated that nonanatomic or minor resection could be performed in a shorter time compared with open surgery.19,20,22 This could be mainly due to the simple steps of nonanatomic or minor resection, and quick management of trocar incision could offset the operation time of laparoscopic resection. In LRH, the primary steps, including dissection of portal pedicles and control and division of the supply vessels, are time consuming. Notably, in our center, we conventionally used laparoscopic Peng's Multiple Operative Dissector (LPMOD), which is a special instrument combining an electrotome and aspirator. 17 With LPMOD, blunt dissection and aspiration could be performed alternatively by surgeons, thereby making the operation more efficient. An average duration of 255 minutes in our series is shorter than other LRH cohorts, which reported about 300–350 minutes.14,27,28 However, this study still revealed a slightly prolonged duration of LRH compared to ORH. Considering early LRH cases to be during learning curve, we believe that the operative time of LRH can be close to or even shorter than that in ORH with accumulated experience.
The substantial risk of perioperative mortality and morbidity remains a major concern that limits the development of LRH for HCC. Patients with HCC and concurrent cirrhosis tend to have a higher incidence of postoperative complications of greater severity. 29 A substantially reported morbidity range from 5.4% to 35.7% means that LRH for HCC is still an immature procedure.14,25,30 In our study, for overall morbidity, LRH tended to be superior to ORH (18.4% versus 26.3%); however, the difference was not statistically significant. Xu et al. compared laparoscopic major resection for HCC with open surgery in patients with cirrhosis using PSM and revealed no significant difference in postoperative complications. 31 Similar to the findings in our study, Komatsu et al. reported less postoperative morbidities in laparoscopic major resection than those in open surgery (31.6% versus 60.5%); however, severe morbidity rates were equivalent. 25 In their study, patients with smaller HCC tended to undergo laparoscopic surgery, which had considerable effects. Furthermore, several comparative studies of major hepatectomy reported a lower complication rate for laparoscopic surgery as less than 10%,14,25 in which the mainstay of tumors was less than 5 cm. The indication of LH with respect to tumor size remains to be clearly established, and a number of studies still recommended that <5 cm is suitable for laparoscopic surgery.32–34 Based on the present findings of right hepatectomy, we speculate that an increased tumor size adversely affects the advantages of LRH, but does not make LRH inferior to ORH.
There were two in-hospital deaths in the ORH group; both were due to secondary liver failure and subsequent multiple organ failure. This suggested that right hepatectomy remains a high-risk procedure for patients with poor liver compensatory capacity. No patients in the LRH group developed liver failure, which could be associated with the minimally invasive nature of the technique. However, the smaller sample size weakens the effect of the result, and statistical difference was not observed. In Komatsu's study, a significantly lower postoperative liver failure incidence in the laparoscopic group was noted (15.8% versus 36.8%). 25 In our study, patients in the LRH and ORH group had similar risks for major postoperative morbidity. Theoretically, laparoscopic surgery could avoid a large subcostal incision and minimize alteration of collateral circulation in the abdominal wall and lymphatic flow of the diaphragm. 35 The integrity of the abdominal wall contributes to the maintenance of stable electrolyte and albumin levels. Consequently, less pleural effusion and ascites, which also serve as main components of minor complications, were observed in LRH. The pain due to a large incision after laparotomy, which could make coughing difficult for patients, could explain the increased respiratory complications. Moreover, in contrast to complete LRH with conversion cases, we found that complications (overall and severe) were higher in the conversion group (overall 15.2% versus 37.5%; severe 6.1% versus 37.5%); however, the difference did not reach statistical significance due to the limited number of cases.
The lack of palpation in laparoscopic surgery was presumed to result in inadequate surgical margin and poorer prognosis. However, several comparative studies revealed that the oncology-specific outcomes of laparoscopic nonanatomic or minor liver resection are not inferior to those of open surgery.19–21 More importantly, during anatomic resection, the surgical margins in LRH could be as sufficient as those in open surgery. Moreover, indocyanine green fluorescence imaging or endoscopic ultrasound could be used to locate the tumor, even tumors located near the resection line, to obtain adequate surgical margin. Therefore, neither procedure is technically superior, but efficiency would largely depend on the technique of the surgeon and on pathologic analytic variability. Thus, considering the principles of radical resection, a technically similar oncologic resection could be performed regardless of whether the open or laparoscopic approach is used. In this study, LRH could achieve sufficient surgical margins and have comparable R0 resection rate to that in ORH, and the 3-year OS and DFS between LRH and ORH were also comparable. These results indicated that LRH possibly has oncological outcomes equivalent to those in open surgery, as factors, including tumor size, tumor stage, tumor pattern, and microvascular invasion, were all balanced. In addition, HCC has a propensity to disseminate into the portal venous territory; recurrence in liver remnants could account for ∼80% of postoperative recurrence. 36 Although therapy such as radiofrequency ablation and TACE can be used to treat these tumors, the use of such methods is limited by a large tumor size, severe peritoneal adhesions, tumor location, and nonradical treatment; repeat surgical resection is an effective radical treatment. 37 Since further salvage treatment is often anticipated, laparoscopic surgery is beneficial in producing fewer adhesions, thereby reducing the need of adhesiolysis during re-resection.38,39
Our case-matched study had certain limitations. First, this is a retrospective study, and selection biases are inevitable despite using PSM to balance the baseline characteristics and enhance the compatibility between the two groups. Second, due to the nature of HCC and technical difficulties of LRH, the sample size of our study is small to strengthen our findings, although some notable trends were observed. Furthermore, this study included data of early cases, and the surgeon performing LRH in our study has vast experience in laparoscopic surgery. The actual influence of learning curve on surgical outcomes remains unclear. Currently, no study reporting the learning curve of this emerging technique has been conducted. Further studies should include the analysis of the learning curve of LRH using sufficient data. Nevertheless, as more surgeons gain more experience and the technology and instruments improve further, the remaining concerns and questions about this procedure will also be addressed.
In conclusion, LRH can be as safe and effective as ORH for HCC. Except for less blood loss, however, LRH has no distinct superiority to ORH. Nevertheless, LRH holds the benefit of less blood loss and appears to achieve less overall and severe postoperative complications, and its oncological results were comparable to those of ORH. LRH could serve as a promising alternative to ORH in selected patients and is worth further investigation for optimization, especially in more specialized medical centers.
Footnotes
Disclosure Statement
No competing financial interests exist.