
Abstract
Abstract
Objectives:
To assess the role of three-dimensional (3D) reconstruction in aiding preoperative planning for highly complex renal tumors amenable to robotic partial nephrectomy (RPN).
Materials and Methods:
Computed tomography (CT) scans and respective 3D reconstructions of 20 highly complex renal tumors were displayed to the attendees/urologists of the 6th Techno-Urology Meeting (www.technourologymeeting.com). These 20 cases had already undergone RPN performed by a single experienced surgeon. The attendees were asked to watch the videos of the CT scans first, and then the respective 3D reconstructions of 5 of the 20 cases who were randomly selected. A purpose-built questionnaire collected responders' surgical experience and surgical indication (RPN versus nephrectomy) after viewing the CT scan and the respective 3D reconstructions.
Results:
Twenty expert urologists, 27 young urologists, and 61 residents (total = 108) participated in the study. Five hundred forty-two views of the cases were obtained. Based on CT scans, RPN was indicated in 256 cases (47.2%). After viewing the respective 3D reconstructions, in 148 cases the responders changed their idea: indication to RPN raised in 404 cases (74.5%) (P < .001). The opinions changed regardless of the surgical experience.
Conclusions:
The findings of this study are encouraging, and they might represent a significant step toward the validation of the use of 3D reconstruction for surgical planning in patients undergoing robotic kidney surgery. The use of this technology might translate into a larger adoption of nephron-sparing approach. Further investigation in this area is warranted to corroborate these findings.
Introduction
T
More recently, authors began to investigate novel tools based on three-dimensional (3D) reconstruction of cross-sectional imaging to allow advantages for both the surgeons and the patients, namely more accurate case-by-case preoperative planning, counseling, and education.5,6 Thus, the feasibility of 3D “image guidance” has been explored as an additional tool to facilitate minimally invasive surgery.5–7
Our group recently reported an early experience with “hyper-accuracy” 3D reconstruction of anatomical structures from CT images in a series of robotic partial nephrectomies (RPNs) for highly complex renal tumors. 8 This technology demonstrated to be valuable in maximizing the understanding of the kidney anatomy, particularly of the renal vasculature and the tumor relationships. However, this emerging technology is still under scrutiny, and barriers challenging its wide clinical application still remain. 5
In this study, our aim was to assess the role of 3D reconstruction in aiding preoperative planning for highly complex renal tumors amenable to partial nephrectomy.
Materials and Methods
Study design
CT scans and respective 3D reconstructions of 20 highly complex renal tumors were made available for display to the attendees/urologists of the 6th Techno-Urology Meeting, held at San Luigi Gonzaga Hospital (Orbassano, Turin, Italy) (www.technourologymeeting.com). These 20 cases had already undergone RPN performed by a single experienced surgeon (>800 minimally invasive partial nephrectomy procedures performed).
The attendees were offered a separated booth and asked to watch the videos of the CT scans first, and then the respective 3D reconstructions of 5 of the 20 cases who are randomly selected.
A purpose-built questionnaire was created and submitted to the attendees after they watched the videos.
The questionnaire included three items/questions (an extract of the questionnaire is reported as Supplementary Data). First, the participants were asked to define their experience (“resident,” “young urologist,” or “experienced urologist”—the latter if with >10 years of robotic surgery practice). Second, they were asked what kind of robotic procedure (partial versus radical nephrectomy) they would have considered after watching the video of the CT scans. Third, after watching the video of the respective 3D reconstructions, they were asked again which procedure they would recommend, in other words to either confirm their previous choice based on CT scan or switch to a different one. To note, the responders were blinded to the procedure that had been performed for these cases and the related outcome. Answers were collected and analyzed.
3D reconstruction
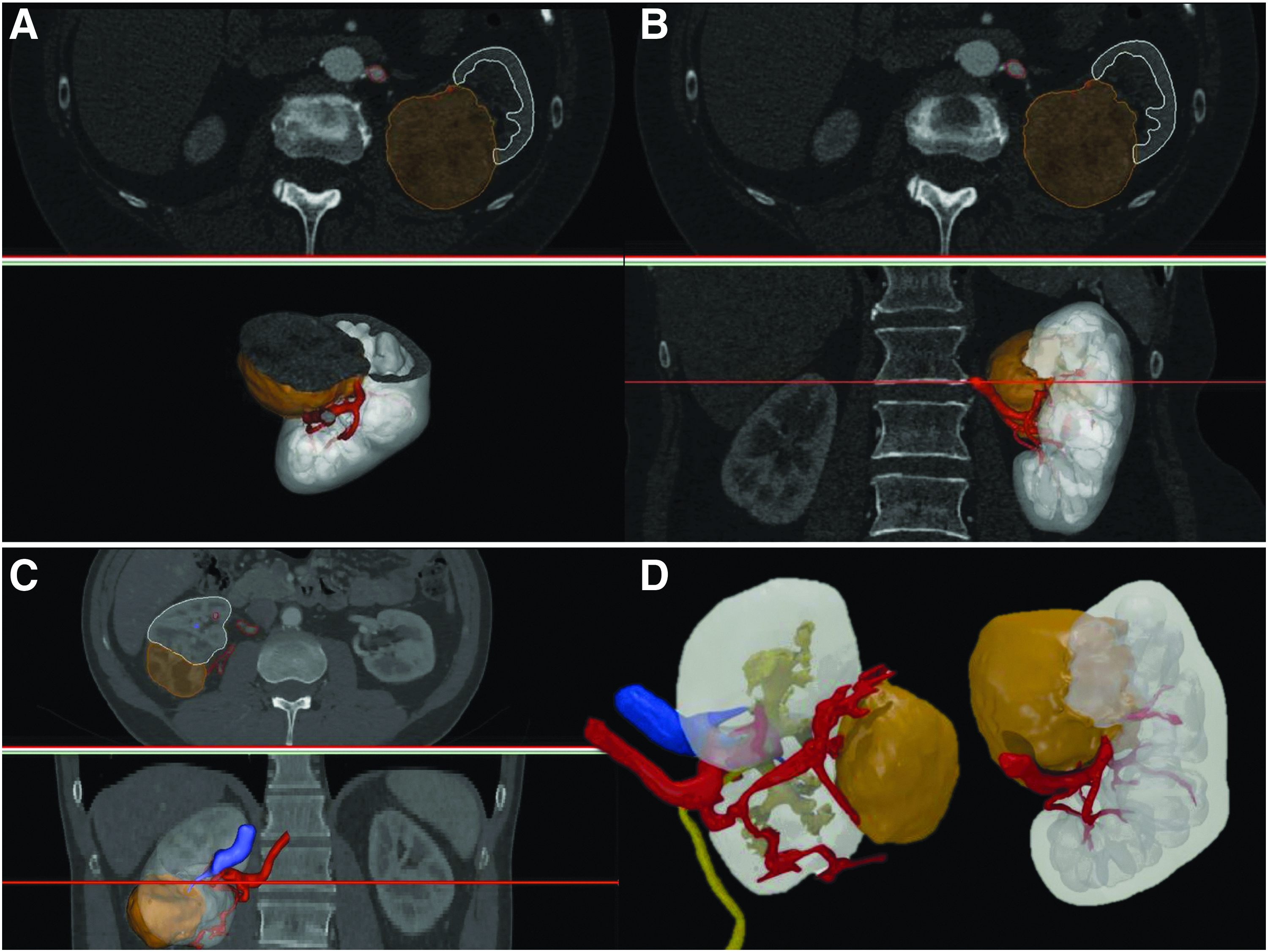
The obtained images from CT scans in DICOM (Digital Imaging and COmmunications in Medicine) format were processed using a dedicated software by M3DICS (Turin, Italy). As previously described, the process consisted of the rendering of a 3D virtual model of the affected kidney on the basis of high-resolution CT scans. 8 The 3D reconstruction was performed by professional bioengineers. It was focused on the renal vasculature, the collecting system, the kidney shape, and the tumor characteristics (Fig. 1).
The obtained virtual models were reviewed by a bioengineer and 2 urologists (D.A. and E.C.), to evaluate the accuracy and the reliability of the reconstruction. The next step was the creation of an interactive 3D-PDF allowing for the navigation during the preoperative and the intraoperative surgical planning. Specifically, for the purpose of the study, the created virtual models were saved as videos, so that they were able to be displayed.
Statistical analysis
Descriptive statistics were performed for the available variables. Categorical variables were reported as frequency and percentage.
The answers given by the responders were analyzed by using the Sign and the Cochran Q tests.
Univariate regression analysis was performed to test the impact of surgeon's experience in changing the opinion. Statistical significance was set at P < .050. The statistical analysis was carried out using “Statistic” 8.0 Software (StatSoft, Tulsa, OK).
Results
The baseline tumor characteristics (tumor size and complexity as assessed by PADUA score 9 ), intraoperative data (operative time, ischemia time, blood losses, and complications), postoperative complications, and final pathology of the clinical cases used for this study are reported in Tables 1 and 2.
UCS, urinary collecting system.
EBL, estimated blood losses; ISUP, international society of urological pathology; UCS, urinary collecting system; WIT, warm ischemia time.
One hundred eight participants (20 expert urologists, 27 young urologists, and 61 residents) agreed to participate in the study, and a total of 542 views of the cases were obtained. Overall, based on CT scans only, in 256 cases (47.2%) a RPN was indicated. After viewing the respective 3D reconstructions, in 148 cases the responders changed their idea, so that the indication to RPN raised in 404 cases (74.5%) (P < .001). After stratifying by expertise, the number of modified indications remained significant in the subgroups, with the expert urologists, the urologists, and the residents in urology, changing their opinions in 22, 28, and 98 cases, respectively (P < .001, Tables 3 and 4).
The Q value is the number of nontie judgments between the first (based on CT-scan) and the second (based on 3D reconstruction) evaluation.
3D, three-dimensional; CT, computed tomography; PN, partial nephrectomy; RN, radical nephrectomy.
Univariable regression analysis did not found the responder's experience as significantly impacting in changing the surgical indication for the displayed cases (P > .050).
Discussion
The implementation of robotic surgery allowed us to expand the indications to partial nephrectomy, and ultimately favored the adoption of a nephron-sparing approach for a higher number of renal masses, including more complex ones.1,2
In the era of “precision surgery,” 10 robotic technology has progressively been paired to sophisticated navigation technologies, with the intent of optimizing the surgical outcomes. Among them, the 3D reconstruction of the bidimensional cross-sectional imaging has been explored as a tool aiming to improve the quality of surgical planning, to facilitate surgical training, and to aid in patients' counseling.5–8
Recent reviews about the topic have been performed by Manning, Langridge et al., and Hoang et al.5,6,11 The overall feeling from the available literature is that the 3D printing and other 3D virtual technologies are demonstrating promising results in the field of urology. Many experiences have been described in the field of the 3D printing in urology.11–21 The 3D printing has been confirmed to be a valuable tool in improving the surgical planning, the younger surgeon's training, and the patient's counseling and education. 6 Partial nephrectomy is particularly considered being a challenging procedure.15–22
As concerning the other 3D technologies, in the specific context of nephron-sparing surgery previous experiences found the 3D virtual guidance technologies to be of valuable help in improving the quality of the surgery when compared with the standard imaging.23–26
Ukimura and Gill first applied an augmented reality visualization system during ablative techniques for renal tumors, concluding that it was a helpful tool to understand 3D anatomies beyond the surgical view during laparoscopic approach. 23
Shao et al. studied a 3D renal vasculature model during laparoscopic PN, concluding that it provided effective orientation for a more precise clamping technique. 24
Similarly, Chen et al. studied 3D models of renal tumor, aimed to facilitate visible-imaging-guided tumor resection during laparoscopic PN for intrarenal tumors. 25
Komai et al. published an experience with case-specific 3D anatomic video images of the kidney. Video simulation of the surgery was possible using the system, and the authors concluded that clampless PN was more likely to be performed thanks to the technology. 26
More recently, Wang et al. reported on the use of individualized 3D visualization technologies for laparoscopic PN, which aimed to provide precise information on the anatomical structures in the operative area and reliable guidance for preoperative planning and intraoperative guidance compared to the standard. 27
Notwithstanding the aforementioned advantages, the 3D reconstruction technologies involve additional direct and indirect costs, and therefore there is a need to determine their real impact in daily surgical practice.5–7
In our recently published study on robotic PN, we demonstrated the reliability of the 3D reconstruction in reproducing the in vivo anatomical structures of the kidney visualized during robot-assisted PN for highly complex renal masses. Moreover, we found that 3D reconstruction allowed for a more accurate preoperative planning in terms of management of renal pedicle when compared with the standard preoperative planning based on the bidimensional cross-sectional imaging. 8
In this study, we tried to do a step forward aiming to test and confirm the utility of the 3D reconstructions over the respective bidimensional CT scans at the time of the surgical planning and counseling for highly complex renal masses.
Our study population was represented by urologists attending a major international meeting focused on new technologies in urologic surgery. These attendees had different levels of expertise. Interestingly, regardless of the experience, in >25% of the cases, the responders changed their indication/recommendation after reviewing the 3D reconstruction.
Even in the subgroup of “expert” urologists (with >10 years of robotic surgical experience), ∼20% changed their indication from radical to partial nephrectomy. Notably, the responders were blinded to either the indication assigned to each case or the outcomes after the surgery, and we underline that all the clinical cases showed had already underwent a successful RPN.
In summary, based on our findings, we confirm that 3D reconstruction technology should be regarded as a valuable tool for both surgeons and patients, the latter with the advantage of being more likely to receive a conservative treatment for renal tumor. 28
This study was not devoid of limitations: first, the fact that the responders were unblinded when watching the displayed clinical cases. One could argue that they were pushed in changing the indication just because of the impressive and attractive 3D reconstruction. Nevertheless, we underline that many responders did not change their idea even after viewing the 3D reconstruction. Instead, the responders were blinded to the successful partial nephrectomies performed for the displayed clinical cases. Moreover, as aforementioned, they were offered a separated “voting booth” to ensure anonymity of their answers.
We underline that the segmentation of the kidney and the renal tumors required to get the showed hyperaccuracy 3D reconstructions was performed manually: experienced urologist, radiology technicians, and bioengineers are necessary before embarking in this technology.
As aforementioned, another issue comprises the costs. To date, the limited diffusion of such technology has still prevented performing studies on cost effectiveness. Once demonstrated, the real utility of the 3D reconstruction cost analysis should be the topic for future studies.
Conclusions
Notwithstanding these limitations, the findings from this study are encouraging, and they might represent a significant step toward the validation of the use of 3D reconstruction for surgical planning in patients undergoing robotic kidney surgery. The use of this technology might translate into a larger adoption of nephron-sparing approach even in case of highly complex renal masses. Further investigation in this area is warranted to corroborate these findings.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.