
Abstract
Abstract
Introduction:
Open gastrectomy (OG) has long been the preferred surgical approach worldwide for treatment of gastric cancer (GC). Nowadays, several randomized prospective trials have confirmed improvements in postoperative outcomes for laparoscopic gastrectomy (LG) compared with open procedures, with similar oncologic outcomes. However, many of these studies come from Eastern countries.
Materials and Methods:
A prospective nonrandomized study was conducted with all patients operated of GC at Ramón y Cajal University Hospital from January 2015 to December 2017. Of the 96 patients enrolled, 47 patients underwent LG and 49 OG. Textbook outcome was defined as the percentage of patients who underwent a complete tumor resection with at least 15 lymph nodes (LNs) in the resected specimen and an uneventful postoperative course, without hospital readmission.
Results:
A textbook outcome was achieved in 51.04% of patients operated of GC. The outcome parameter “no severe postoperative complication” had the greatest negative impact on the textbook outcome. A statistically higher number of patients with early cancer (40% versus 16.3%) and subtotal gastrectomy (57.5% versus 34.7%) were found in the laparoscopic group. No statistical differences were found between open and laparoscopic approaches regarding operating time, rate of microscopic margin positivity, hospital stay, number of retrieved LNs, complications, reinterventions, mortality, and readmissions. No statistical differences in textbook outcome were found between both groups (57.14% versus 45%; P = .25).
Conclusions:
LG for treatment of GC seems to be safe and feasible with similar textbook outcomes compared with OG.
Introduction
Open gastrectomy (OG) has long been the preferred surgical approach worldwide for treatment of gastric cancer (GC). Laparoscopic gastrectomy (LG) is widely known to be associated with shorter hospital stay, less intraoperative blood loss and transfusions, reduced morbidity, decreased pain, better cosmetics, faster postoperative recovery, and better postoperative quality of life.1–4
Nowadays, several randomized prospective trials have confirmed improvements in postoperative outcomes for laparoscopic assisted distal gastrectomy (LADG), not only for early-stage GC5–7 but also for advanced GC.8–11 In fact, Kim and Yang 12 have reported in a final trilogy study that LADG is safe and feasible in early GC, and possible for advanced GC in skilled surgeons at high-volume centers. Furthermore, in the following years, LADG is expected to become the gold standard for the resection of distal gastric tumors particularly in Far East Asian nations.
Regarding laparoscopic assisted total gastrectomy (LATG), there is less evidence because it is technically more demanding and more randomized control trials are required. Chen et al. 13 have reported that the existing research shows that LATG is safe and feasible, with similar retrieved lymph nodes (LNs) as in OG and with the advantages of minimally invasive approach. More recently, the results from the Japanese nationwide web-based database showed that laparoscopic total gastrectomy could be a safe procedure to treat GC compared with open total gastrectomy. 14 However, most of the published studies were retrospective, the sample sizes were small, most of the cases were early GC, the follow-up periods were not long enough, and the results exhibited substantial heterogeneity.15,16
However, traditionally, quality assessment for complex surgical procedures, such as gastrectomy, has focused on outcome measures such as surgical mortality. However, this information is so simple to analyze the successfulness of this difficult procedure. In 2011, the Dutch Upper Gastrointestinal Cancer Audit (DUCA) group initiated a nationwide registry of all patients with esophageal or GC in whom a surgical resection was planned. The aim of this registry was to develop a composite measure of multiple outcome parameters, defined as a “textbook outcome,” to compare more strictly the quality of care that different surgical groups offer after esophagectomy and gastrectomy. 17
The aim of our study was to compare the outcomes between OG and LG for treatment of GC based on an analysis of this textbook outcome.
Materials and Methods
Patients
A prospective nonrandomized study was conducted with all patients operated of GC at Ramón y Cajal University Hospital from January 2015 to December 2017. A total of 126 patients were identified. Patients undergoing palliative gastrectomy having peritoneal seeding metastasis (15 cases), those with nonadenocarcinoma histology (8 cases), or those in whom GC was not resected (7 cases) were excluded. A total of 96 patients who met these criteria were identified and included in the global analysis. Patients were not randomized, divided into two groups whether surgery was performed laparoscopically or open. However, for comparison between open and laparoscopic procedures, patients who underwent attempted LG but who required conversion to an open procedure were similarly excluded (n = 7). Reasons for converting to open procedure were due to a bulky gastric tumor with suspicion of invading adjacent organs in 2 cases, adhesions in 1 case, esophagojejunal anastomoses leak in 1 case, bulky adenopathic tumor in celiac trunk in 1 case, anesthesiologist problems in 1 case, and obesity in 1 case (Fig. 1).
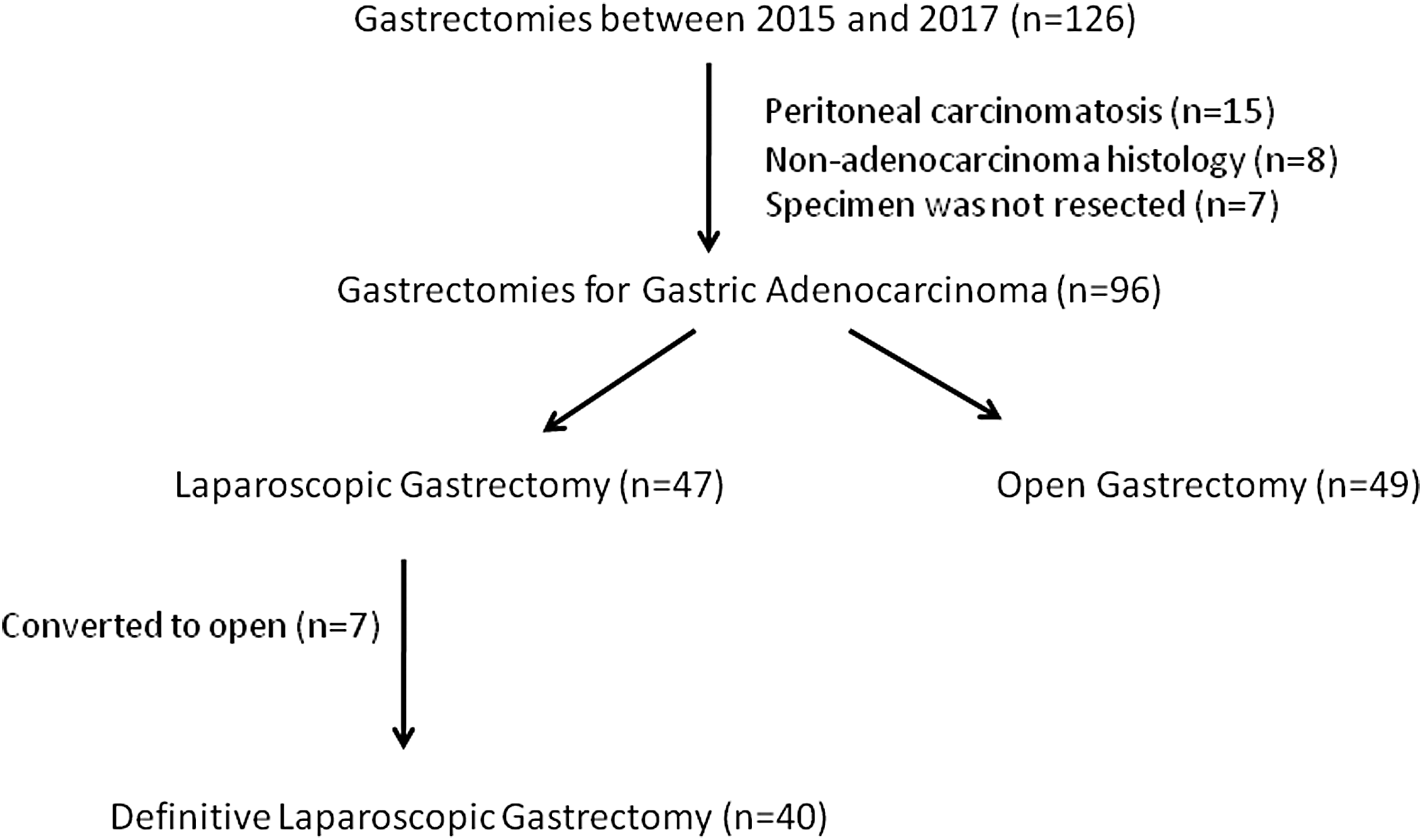
Flowchart of study selection.
Variables
Clinical and follow-up data were obtained from a prospectively maintained GC database. Textbook outcome was defined as the percentage of patients who underwent radical resection according to the surgeon at the end of surgery, tumor-negative resection margins (according to the College of American Pathologists, resection margins are considered positive when tumor cells are present within the surgical margin), at least 15 LNs retrieved and examined, no severe postoperative complication (postoperative complications of grade II or higher according to the Clavien–Dindo classification were considered severe), no reintervention (endoscopic or radiological reintervention are not considered), no readmission to the intensive care unit, no prolonged hospital stay (21 days or less), no postoperative mortality (postoperative mortality was defined as death during the initial hospital stay and/or within 30 days after the day of surgery), and no readmission after discharge from hospital. A textbook outcome was achieved when all nine parameters were realized.
Surgical technique
Surgical treatment varied from total or subtotal gastrectomy regarding the location and the nature of the tumor. Extent of LN dissection followed the Japanese Gastric Cancer Association guidelines. At our institution, LG is performed with an antecolic Roux-en-Y reconstruction normally using a linear stapler side-to-side anastomosis. OG was performed in the same manner as laparoscopic surgery through an upper midline incision, but the esophagojejunal anastomosis was performed with a conventional circular stapler.
Postoperative care
Postoperative mobilization was encouraged from postoperative day 1 (POD1). Recovery of oral intake was initiated on POD3 with water, followed by a dietary progression from liquid to soft food in cases of subtotal gastrectomy. However, a routine radiological study using a water-soluble contrast medium at POD7 was performed to all total gastrectomies to check the anastomosis before starting oral diet. Until water-soluble contrast was conducted, patients were treated with parenteral nutrition.
Statistical analysis
Statistical analysis was performed with the statistical software SPSS 23.0 for Windows (IBM SPSS, Inc., Chicago, IL). Quantitative variables that followed a normal distribution were defined by the mean and standard deviation. For non-Gaussian variables, the median and range were used. Qualitative variables were defined by number and percentage of cases. Comparison of variables was performed with a Student's t-test (Mann–Whitney test in non-Gaussian variables). Comparison of qualitative variables was performed with the chi-square test; in those cases with fewer than five observations in the cell, the Fisher exact probability method was used. P < .05 was considered statistically significant.
The overall proportion of patients for each separate outcome parameter included in a textbook outcome was described, together with the proportion of patients in whom each consecutive outcome parameter was realized, provided that all previous criteria were met.
Results
Dates of overall series
Of the 96 patients enrolled in the study, 59 were men and 37 women with a mean age of 72.25 ± 11.4 years. Perioperative patient risk was assessed using the American Society of Anesthesiology (ASA) Scoring System: ASA I: 9 cases (9.4%), ASA II: 54 cases (56.3%), ASA III: 32 cases (33.3%), and ASA IV: 1 case (1%). Twenty-nine cases (30.2%) received neoadjuvant treatment with chemotherapy and a laparoscopic approach was performed in 47 cases (49%) with a conversion rate of 14.9% (7 cases). Total and subtotal gastrectomy were performed in 54 cases (56.3%) and 42 cases (43.8%), respectively. The rest of the characteristics of patients are described in Table 1.
Characteristics of Global Series
LNs, lymph nodes.
A textbook outcome was achieved in 51.04% of patients (49 cases) with GC. The outcome parameter “no severe postoperative complication” had the greatest negative impact on the textbook outcome. No grade II or higher according to the Clavien–Dindo complications was found in 67.7% of patients. The overall proportion of patients for each separate outcome parameter included in a textbook outcome is described in Figure 2.
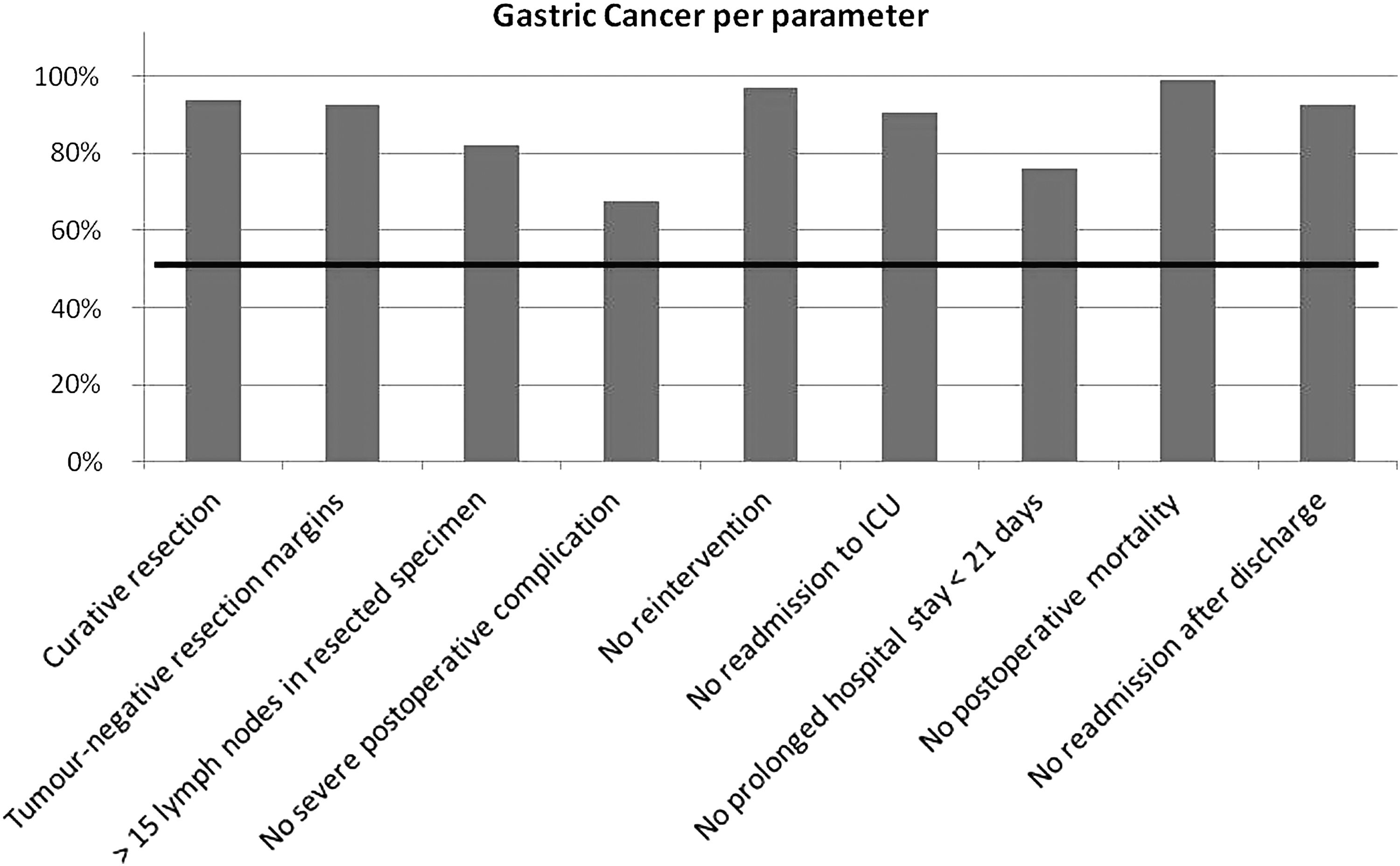
Textbook outcome: a composite measure of outcome parameters in patients undergoing surgery for gastric cancer. The horizontal line represents the percentage of patients (51.04%) in which the textbook outcome was completely achieved.
Comparison of the clinicopathological characteristics between OG and LG
No statistical differences were found between both groups regarding age, gender, ASA score, location of tumor, neoadjuvant treatment, and positive LNs. However, a higher rate of female patients was enrolled to LG against OG (47.5% versus 28.57%; P = .08). Moreover, location of tumor was not completely same to both approaches, with a higher rate of tumors in the antropyloric region in the LG than in the OG (57.5% versus 36.7%; P = .06). Furthermore, resections of tumors over a gastric stump were directly reserved to open surgery (14.3% versus 0%). However, a statistically higher number of patients with early cancer (in situ and T1) (40% versus 16.3%; P = .03) and subtotal gastrectomy (57.5% versus 34.7%; P = .05) were found in the laparoscopic approach group. The clinicopathological characteristics of LG and OG are summarized in Table 2.
Comparison of the Clinicopathological Characteristics
Bold values indicate statistically significant results.
ASA, American Society of Anesthesiology.
Comparison of surgical outcomes between OG and LG
No statistical differences were found in mean operative time, tumor-positive resection margins, retrieved LNs, reinterventions, hospital stay, mortality, and readmissions between both groups. The surgical outcomes are shown in Table 3.
Comparison of Surgical Outcomes
LNs, lymph nodes.
Comparison of postoperative complications between OG and LG
Sixteen cases out of 49 patients in OG and 17 out of 40 patients in LG developed postoperative complications, which was not statistically different between 2 groups (32.7% versus 42.5%; P = .33). According to Clavien–Dindo classification, there were six (12.1%) major (Clavien–Dindo III or higher) postoperative complications in the OG group and five (12.5%) major complications in the LG group (P = .78). The details of postoperative morbidities are summarized in Table 4.
Comparison of Postoperative Complications
Comparison of textbook outcomes between OG and LG
No statistical differences in textbook outcome were found between both groups (57.14% versus 45%; P = .25). The outcome parameter “no severe postoperative complication” had the greatest negative impact on the textbook outcome both for LG and OG (62.5% and 67.3%). More than 15 LNs in the resected specimen were identified in 77.5% in the laparoscopic group and in 87.8% in the open group (Fig. 3).
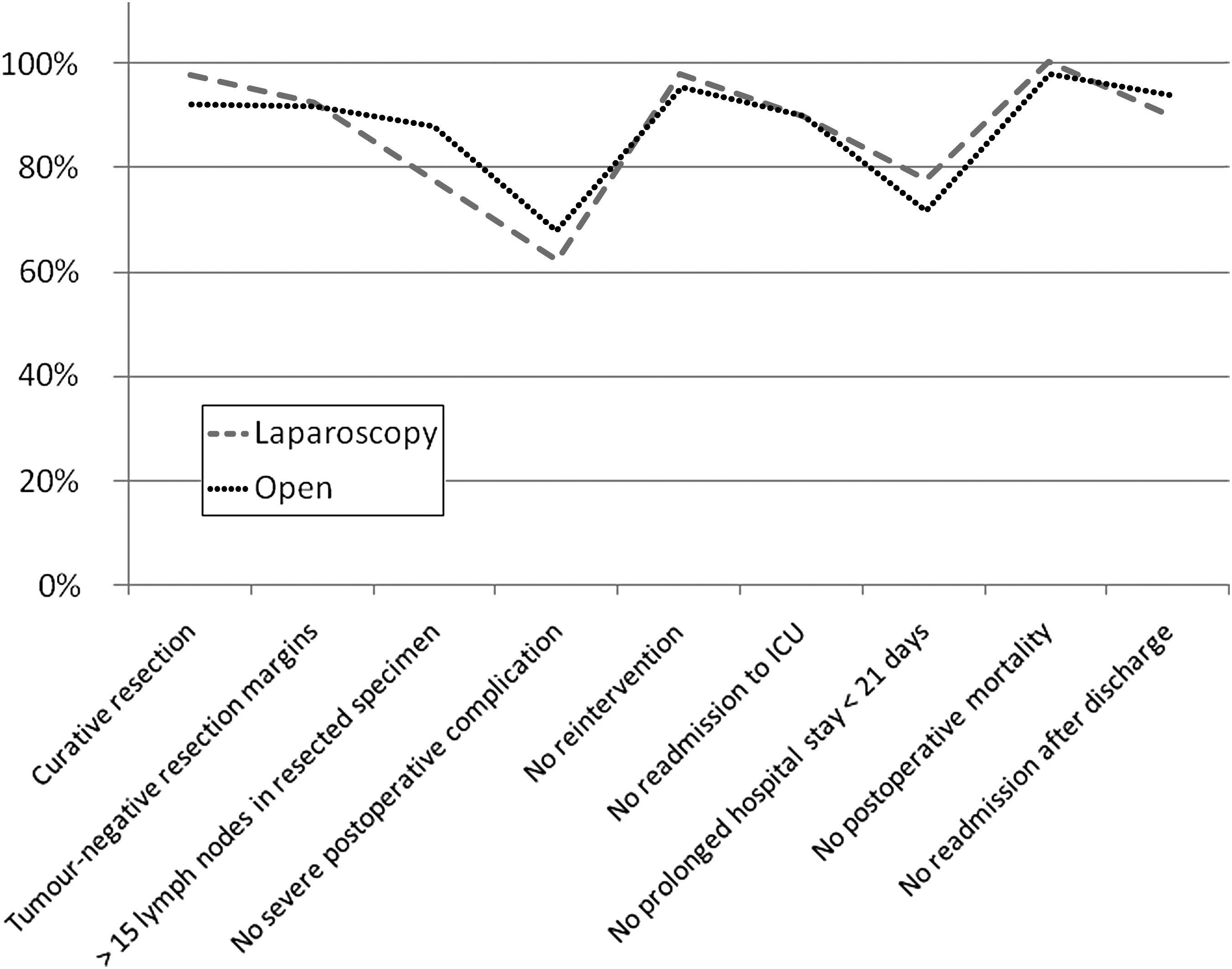
Comparison of textbook outcome between laparoscopy and open approaches.
Discussion
Nowadays, several randomized prospective trials have confirmed improvements in postoperative outcomes for LG compared with open procedures, with similar oncologic outcomes. However, many of these studies come from Eastern countries, and it is not clear whether these data can be applied to patients in Western countries.18–20 This study contributes to the Western experience by providing data on the safety and oncologic efficacy of LG in a series of patients in a high-volume hospital center of Spain.
Traditionally, quality assessment for complex surgical procedures, such as gastrectomy, has focused on surgical mortality. However, this information is so simple to analyze the successfulness of this whole surgical procedure. For these reasons, first of all, we have tried to assess the quality of our gastrectomies with a composite measure of multiple outcome parameters, defined as a “textbook outcome” created by DUCA, to compare with other European surgical groups. In our series, a textbook outcome was achieved in 51.04% of patients with GC, which is in the range compared with results published by DUCA group (adjusted textbook outcome rates ranged from 11.4% to 52.4% for hospitals undertaking resections for GC). 17 The outcome parameter “no severe postoperative complication” had the greatest negative impact on the textbook outcome. No grade II or higher according to the Clavien–Dindo complications was found in 67.7% of patients. However, we do not agree with this definition because, in our opinion, severe complications should be Clavien–Dindo IIIB or more. In our series, this rate of severe complications was 8.2% with a mortality rate of 1%, which corresponded well with other contemporary European results.21,22 The rest of the parameters of the textbook outcome were excellent, ranging more than 90% in all the cases except for “no prolonged postoperative stay <21 days” (76%), which is associated with the postoperative complications explained before.
Regarding the number of retrieved LNs, in our series, the mean of retrieved LNs has been 24.31. Although there is an agreement that at least 15 LNs should be dissected to provide an adequate and accurate postoperative N staging,23,24 our aim is to achieve at least 25 LNs in each gastrectomy for cancer. 25 However, and regarding the textbook outcome, the percentage of retrieved LNs >15 was 82.3%, which was higher than that published by the DUCA group (57.1%). 17
Perhaps in our series we have a high rate of tumor-positive resection margins of 7.3%, most of the times in diffuse-type adenocarcinoma. However, most of the patients had advanced gastric tumors (T4aN1-2), with gastric linitis adenocarcinoma or recurrence tumors over the gastric stump (2 cases). However, in those cases we had no apparent doubts about the surgical margins, so we did not decide to send intraoperative frozen section of the proximal or distal margin. Maybe rigorous frozen section analysis should be performed for patients with diffuse-type GC, which is more frequent in Western countries. In our algorithm of treatment, in cases with positive postoperative resection margin, a multimodal treatment with chemo- and radiotherapy was offered, not being candidates for resection due to the advanced staging of the disease (T3-4N+).
Laparoscopic procedure conversion rates were documented in 14.9%, which was so much higher than that published in the literature, ranging from 0.00% to 6.67%, with a weighted average of 1.68%.26,27 However, to be honest, some of these conversions were more to lack of selection of cases for laparoscopic approach due to advanced GC, rather than intraoperative complex complications (only 1 case due to an intraoperative-checked esophagojejunal leak that could not be solved laparoscopically).
Regarding comparison between open and laparoscopy, it is observed that there are no differences in outcomes in both groups. In summary, the laparoscopic approach seems to be feasible for treatment of GC with the typical advantages of the minimally invasive approach that we have not studied in our series.1–4 It is true that we have found a statistically higher number of patients with early cancer (40% versus 16.3%) and subtotal gastrectomy (57.5% versus 34.7%) in the laparoscopic group, which is in concordance with the international guides because, nowadays, the best indication for laparoscopic approach is early cancer tumors of distal location. Moreover, there are a nonstatistical higher number of retrieved LNs in OG versus. LG (28.53 ± 13 versus 24.73 ± 11; P = .16). However, the average of retrieved LNs in the LG group is already 25, getting our aim to achieve at least 25 LNs in each gastrectomy.
Furthermore, there were no differences in overall complications between open and laparoscopic approaches (32.7% versus 42.5%; P = .33). In our series, LG seems to be safe in comparison to OG, even though. 60% of patients (in LG group) had an advanced GC (T2-4). These results agree with the previous Asian articles of Kim and Yang 12 and Chen et al. 13 reporting that LG is safe and feasible, with similar retrieved LNs as in OG and with the advantages of minimally invasive approach.
Finally, there was no difference regarding the textbook outcomes between both groups, so the quality of care we are offering to our GC patients does not differ except for the surgical approach. However, we want to improve our rate of retrieved LNs and reduce the severe grade II or more Clavien–Dindo complications to reduce the hospital stay. Moreover, we are considering implementing an enhanced recovery program for GC surgery in the following months.
To be honest, there are some limitations in our study. Although the prospective nature of the investigation is a positive factor to stand out, the absence of randomization has created two nonhomogeneous groups that could influence in comparison with the results, with more antropyloric tumors, early cancers, and subtotal gastrectomies in the laparoscopic group.
To sum up, LG for treatment of GC seems to be safe and feasible in Western countries, with similar textbook outcomes compared with OG.
Footnotes
Disclosure Statement
No competing financial interests exist.