
Abstract
Abstract
Background:
The purpose of the study was to evaluate the safety and effectiveness of three-port laparoscopic right colectomy (3-LRC) for right-sided colon cancer compared with conventional five-port laparoscopic right colectomy (5-LRC).
Materials and Methods:
One hundred sixty-three patients diagnosed with right-sided colon adenocarcinoma underwent laparoscopic right colectomy (LRC) between April 2011 and December 2017. Seventy-four of these patients underwent 3-LRC procedure and 89 patients underwent 5-LRC. Clinical characteristics, perioperative short-term outcomes, and pathologic data were analyzed.
Results:
There were no differences in TNM stage, tumor location, estimated blood loss, complications, and open conversion rates. The operation time was shorter in the 3-LRC group than in 5-LRC group (140.9 ± 27.5 minutes versus 178.2 ± 38.2 minutes; P = .001). The number of harvested lymph nodes (28.5 ± 13.9 versus 22.6 ± 11.7; P = .004) was also higher in the 3-LRC group. The first passage of flatus and first oral diet were significantly faster in the 3-LRC group than in the 5-LRC group (2.8 ± 1.0 days versus 4.0 ± 1.2 days; P = .001, 3.6 ± 2.9 days versus 5.0 ± 1.5 days; P = .001). The number of patients who required analgesics is less in the 3-LRC group (32.4% versus 43.8%; P = .583).
Conclusion:
3-LRC for right-sided colon cancer is technically feasible and is associated with a short operation time. We believe that 3-LRC effectively reduces the costs associated with equipment and manpower and represents a standard procedure.
Introduction
Currently, laparoscopy is the standard operative technique for colon cancer treatment. Laparoscopic right colectomy (LRC) represents an alternative to open colectomy for the treatment of right-sided colon cancer.1,2 LRC is associated with improved pain management, faster restoration of bowel function, shortening of hospital stay, and improved cosmesis with comparable perioperative morbidity.3,4 Prospective randomized controlled trials comparing multiport laparoscopy with open colectomy have reported equivalent oncological outcomes with either procedure. 5
Recently, reduced port surgery has become increasingly popular for colectomy. Single-incision laparoscopic colectomy (SILC) has been rapidly adapted for application to colon surgery. SILC was first described in 2008.6,7 SILC has potential advantages as follows: (1) a single approach can reduce the risk associated with port placement such as incisional hernia, bleeding, surgical site infection, and port site recurrence; (2) decreased use of opioid analgesia due to less postoperative pain; (3) improved cosmesis; and (4) reduced ileus.8–10
However, SILC has several disadvantages compared to multiport laparoscopic surgery. Compared with conventional laparoscopic surgery, the operation time is prolonged and entails the use of multiple surgical instruments. In addition, the indications are limited, especially if the patient has a high degree of obesity or an obstruction is accompanied by difficulty in triangulation and securing the field of view is a challenge. 11 Therefore, additional ports or open conversions have been reported.11,12 Moreover, the single-port procedure needs up to 5 cm of inner incision for colon extraction to avoid the possibility of noncosmetic results or incisional hernias. One of the factors that limit SILC is the additional learning curve required.
Even after a decade since SILC was introduced, it is still difficult to overcome these disadvantages and is not widely practiced. Several studies suggest that 3-LRC is an appropriate alternative or intermediate stage of SILC because of inconvenience rather than the benefits of SILC.13,14 Based on this background, we also considered 3-LRC as an alternative to the difficult SILC and due to the reduced number of ports compared with conventional 5-LRC.
The aim of this study was to evaluate the role of 3-LRC in overcoming the disadvantages of SILC, as a safe and feasible alternative, by comparing the short-term outcomes to those involving conventional 5-LRC.
Materials and Methods
From April 2011 to December 2017, a total of 163 patients with right-sided colon cancer, including cecum, ascending colon, hepatic flexure colon, and transverse colon cancer, underwent laparoscopic colectomy at two hospitals. Surgery was performed by 4 colorectal surgeons. One operator who is the author for correspondence used the 3-port method and another surgeon performed the 5-port technique.
We examined patient variables, including age, sex, height, weight, body mass index, American Society of Anesthesiologists (ASA) score, underlying disease, history of previous abdominal surgery, and location of tumors. This project was approved by the Institutional Review Board of Gyeongsang National Hospital, the Gyeongsang National University of Korea on January, 2018 (GNUH 2018-01-010).
The intraoperative parameters were compared with operation time, intraperitoneal adhesion, the conversion rate (conversion to open surgery during laparoscopic operation), and factors contributing to the conversion. The postoperative parameters used to compare the restoration of postoperative bowel function (the first passage of flatus, the time to first oral diet), the duration of the hospital stay, additional analgesic use, and postoperative complications. The oncological adequacy of the tumor was assessed by the number of harvested lymph nodes and the length of the proximal and distal free margins. We retrieved all the data from the electronic medical records for retrospectively analysis. Statistical analyses were performed using the SPSS version 18.0 (SPSS Inc., Chicago, IL). The χ 2 and Student's t-tests were used to compare the data for each group. P < .05 was considered statistically significant.
Surgical techniques
Three-port laparoscopic right colectomy
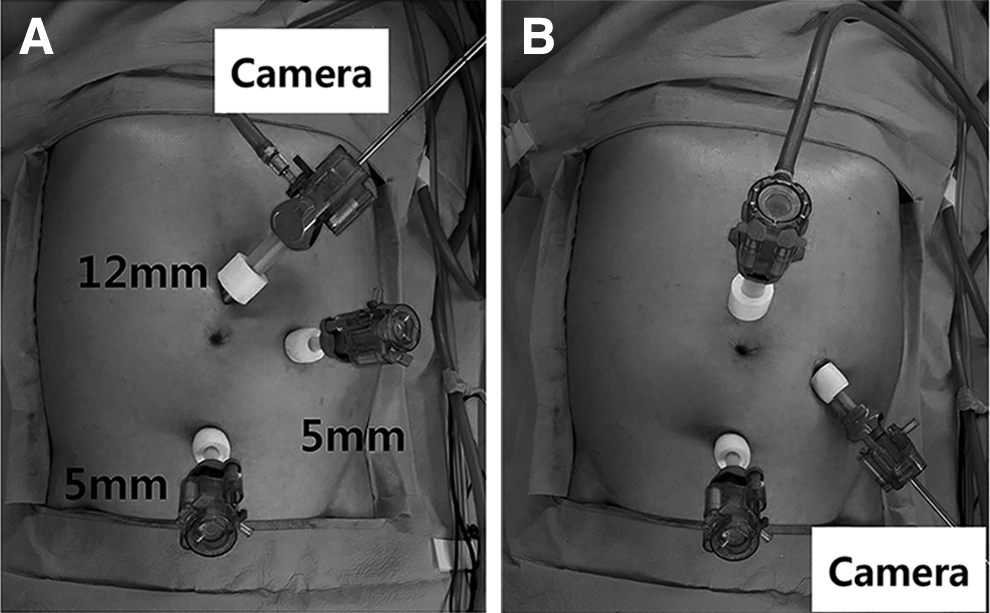
This procedure was performed by a single surgeon and a single camera operator. Under general anesthesia, the patient was placed in a supine position. The surgeon and scopist stood on the left side of the patient, without another first assistant (Fig. 1). One 12 mm camera port was inserted just above the umbilicus, and two 5 mm ports were placed in the left midclavicular line and suprapubic (Fig. 2A). The EndoEYE 5 mm flexible (Olympus, Tokyo, Japan) or 30° rigid telescope (Olympus) and traditional laparoscopic instruments were used. All the three ports of LRC were accessed via inferolateral to medial approach. The patient was moved into the Trendelenburg position and a left-tilted position. First, mobilization of terminal ileum, right colon, and hepatic flexure colon was performed, followed by the detachment of colon mesentery from duodenum and pancreas. The ileocolic, right colic and middle colic artery and vein were divided at the origin using a surgical clip and the LigaSure sealing system (Covidien, Norwalk, CT). If the tumor is located in the cecum and the ascending colon, the main pedicle of the middle colic artery was saved and divided at the right branch of middle colic artery. The patient was shifted to a reverse Trendelenburg position and the camera moved to the left port (Fig. 2B). Detachment of the greater omentum from the transverse colon was performed. After mobilization of the intestine and division of the vessel, a wound protector was placed in a mini-laparotomy with a supraumbilical or transumbilical extension, including camera port incision. Next, the segment containing the tumor was resected from the abdominal cavity via minilaparotomy. The OCTO™ OT501S2 Port 50 mm (DalimSurgNET, Seoul, Korea) was used if the tumor was less than 5 cm, and an Alexis® wound retractor C8302 50–90 mm (Applied Medical, Rancho Santa Margarita, CA) was used if the tumor was larger than 5 cm. Extracorporeal end-to-side anastomosis was accomplished using DST EEA 28™ or 31™ (Covidien) and Endo GIA Roticulator-60™ staples (Covidien). The anastomotic site and stump were performed with reinforcement sutures followed by mesentery repair with continuous suture using v-loc. The bowel was returned to the peritoneal cavity and pneumoperitoneum was reestablished. The drain was inserted through the suprapubic 5 mm port, and the wound was closed in layers.
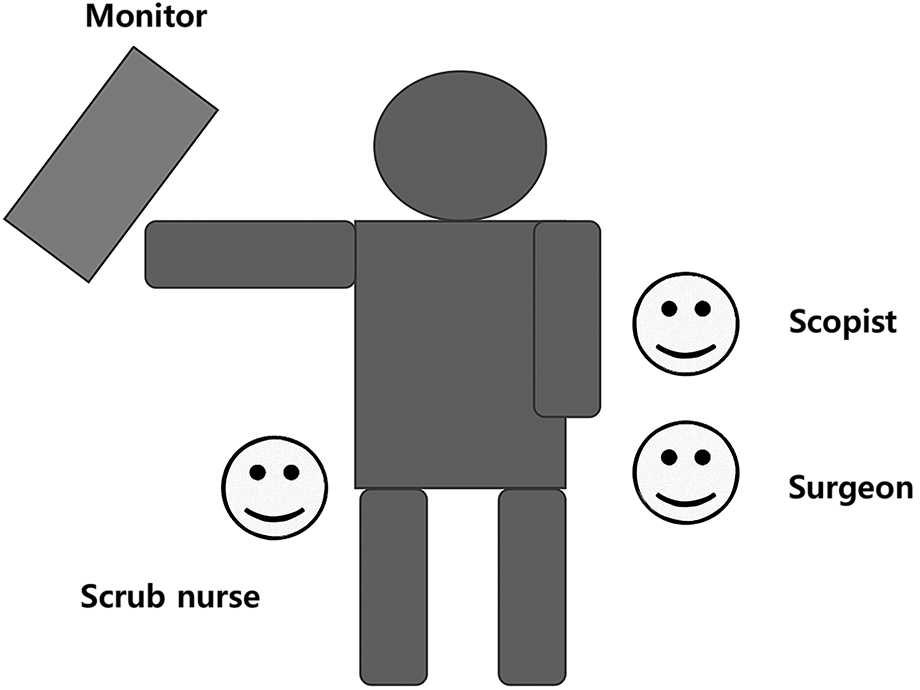
Schematic diagram of 3-LRC. The surgeon is located on the left side of the patient and the scopist is located on the right side of the surgeon. 3-LRC, three ports laparoscopic right colectomy.
One 12 mm Transport (DalimSurgNET, Seoul, Korea) was inserted just above the umbilicus, and two 5 mm Transports were placed in the low and left abdomen. The EndoEYE 5 mm flexible and rigid telescope (Olympus) and traditional laparoscopic instruments were used.
Conventional five-port laparoscopic right colectomy
Under general anesthesia, each patient was placed in a supine position. The surgeon stood on the left side of the patient, with the first assistant standing on the right side of the patient, and the scopist standing on the right side of the surgeon. One 12 mm camera port was inserted just above the umbilicus, and 4 additional working ports were placed in the abdominal quadrants. The size of the left upper quadrant port was 12 mm, whereas the remaining ports were 5 mm. The surgical procedure and order were similar to that of 3-LRC except that the first assistant created the surgical field.
Results
Between April 2011 and December 2017, 163 cases of LRC were performed by 4 surgeons to treat patients with right-sided colon adenocarcinoma. Among these cases, 74 patients underwent 3-LRC and 89 patients received 5-LRC for right-sided colon cancer. The gender ratio was similar in both groups. The average age involved the late 60s with no difference between the groups. The ASA score, presence of underlying disease, history of abdominal surgery, and tumor location were not different between the two groups. However, the mean body mass index varied: 22.6 ± 3.0 kg/m 2 in the 3-LRC group and 23.9 ± 3.2 kg/m 2 in the 5-LRC group (P = .006). Bowel obstruction due to cancer was somewhat higher in the 3-LRC group than in the 5-LRC group (55.4% versus 21.3%; P = .001). A higher number of emergency cases were found in the 3-LRC group. Other clinical data are shown in Table 1.
Clinical Characteristics
ASA, American Society of Anesthesiologists; 3-LRC, three ports laparoscopic right colectomy; 5-LRC, five ports laparoscopic right colectomy.
The mean operative time was shorter in the 3-LRC group than in the 5-LRC group (140.9 ± 27.5 minutes versus 178.2 ± 38.2 minutes; P = .001). There was no difference in the rate of open conversion between the groups: 9 (12.2%) in the 3-LRC group versus 12 (13.5%) in the 5-LRC group (P = .802). There were no differences in the rate of previous abdominal surgery and incidence of intra-abdominal adhesion in both groups (Table 2).
Intraoperative Outcomes
3-LRC, three ports laparoscopic right colectomy; 5-LRC, five ports laparoscopic right colectomy.
Restoration of postoperative bowel function, which is defined as the first passage of flatus, and the first oral diet were earlier in the 3-LRC group than in the 5-LRC group (2.8 ± 1.0 days versus 4.0 ± 1.2 days; P = .001 and 3.6 ± 2.9 days versus 5.0 ± 1.5 days; P = .001). The postoperative hospital stays were similar in both groups. Postoperative complications occurred in 3 patients of the 3-LRC group, which was lower than in the 5-LRC group in 10 patients, but was not statistically significant. No severe complications such as anastomotic leakage occurred in both groups. All patients in both groups underwent intravenous patient-controlled analgesia (IV PCA) for postoperative pain control (POPC). In addition to IV PCA, the proportion of patients who received additional analgesics was slightly lower in the 3-LRC group than in the 5-LRC group, without any statistically significant difference (Table 3).
Postoperative Outcomes
3 LRC, three ports laparoscopic right colectomy; 5-LRC, five ports laparoscopic right colectomy.
Among the pathological characteristics, tumor stage and lymph node metastasis were generally higher in the 3-LRC group than in the 5-LRC group. The tumor size was larger in the 3-LRC group than in the 5-LRC group (5.6 ± 2.8 cm versus 4.6 ± 3.1 cm; P = .0261). Both proximal and distal free margin were longer in the 3-LRC group than in the 5-LRC group (25.7 ± 16.0 cm versus 16.9 ± 6.9 cm; P = .001 and 17.9 ± 7.8 cm versus 12.3 ± 5.6 cm, P = .001). The number of harvested lymph nodes also tended to be somewhat higher in the 3-LRC group than in the 5-LRC group (28.5 ± 13.9 cm versus 22.6 ± 11.7 cm, P = .004). The pathology results are listed in Table 4.
Pathological Characteristics
3 LRC, three ports laparoscopic right colectomy; 5-LRC, five ports laparoscopic right colectomy.
Discussion
The COLOR (COlon carcinoma Laparoscopic or Open Resection), which is a European multicenter randomized trial, has shown the feasibility of laparoscopic surgery compared with open surgery as the standard surgical intervention for colon cancer treatment. 15 The advantages of laparoscopic surgery compared with open surgery for colorectal cancer patients include early postoperative recovery, reduced pulmonary dysfunction, reduced narcotic use due to decreased postoperative pain, and shorter hospitalization.4,11,16,17 In addition, the prognosis after surgery for patients with colorectal cancer was not significantly different between laparoscopy and open groups.3,15,18 Therefore, laparoscopic surgery has become the standard in patients with colorectal cancer.
Advances in surgical instrumentation and technology have popularized laparoscopic surgery. SILC is a minimally invasive surgery beyond conventional laparoscopic surgery. SILC was first introduced in 2008 and is currently used for colorectal cancer surgery. 6 The advantages of SILC include avoidance of port site-related complications (wound pain, infection, incisional hernia, and internal adhesion), improved cosmesis, and reduced incisional and parietal pain.11,19 However, the disadvantages that have yet to be overcome include long operating time, high operating costs, difficulty in patients with obesity or large tumor size, and a steep learning curve.20–22 SILC is not user-friendly because a single surgeon and a single scopist operate on three to four ports in one incision. Interference with the surgical instrumentation and collision with the camera are other limitations. Therefore, an alternative to SILC for colon surgery is based on three ports.13,14 The 3-port procedure is not substantially different from SILC because it uses only surgeon's ports instead of first assist ports used in conventional 5-port procedures. However, compared to SILC, the surgeon's hands are free to use ports that are located at different positions and do not interfere with the camera.
Therefore, we investigated 3-LRC compared with 5-LRC for its advantages and user-friendly features compared with SILC. Since the surgical procedures of 3-LRC and 5-LRC are essentially the same except for the number of abdominal incisions, the primary benefit of 3-LRC for patients is the short operating times, acceptable cosmetic results, and minimal wound pain. In addition, the rapid restoration of bowel function after the operation is an advantage in resuming meals early. Finally, the oncological outcomes in 3-LRC were not compromised compared with 5-LRC.
In this study, there was no significant difference between the two groups in terms of gender, ASA score, underlying disease, and tumor location. Operative morbidity and intraoperative outcome were considered as important factors. The rate of conversion to laparotomy was not different between the two groups. However, the operation time was significantly shorter in 3-LRC than in 5-LRC (140.9 ± 27.5 versus 178.2 ± 38.2, P = .001) due to the shortening of the insertion and closure time in 3-LRC. By contrast, an additional port and extra time are needed for the first assistant in the 5-LRC.
There was no statistically significant difference in postoperative complications between the two groups and the hospital stay was similar. However, in addition to the relatively short time required for resumption of first oral diet, the first passage of flatus as a reference point for recovery of intestinal function was short in the 3-LRC group. The rapid recovery of intestinal function is attributed to the reduced bowel handling of first assist in previous surgery and the shortening of operation time. However, there was no significant difference in hospital stay between the two groups of Korean patients due to the tendency to complete the wound closure and stitch out first and discharge the patient later. In addition, patients in Korea have a low economic burden due to well-established medical insurance system. The actual discharge date was earlier in the 3-LRC group than in the 5-LRC group (5.6 days versus 7 days).
Recent studies have also showed that the postoperative pain was reduced in procedures with fewer ports or a single-port laparoscopic colectomy.21,23 In our routine POPC procedures, we investigated the use of additional analgesics. However, contrary to our expectations, no significant differences were found between the two groups. In our study, we did not investigate pain scores such as Visual Analog Scales score, which may be a study limitation. Investigation into pain reduction in the 3-LRC group requires additional patients and a further study to investigate pain scores is needed.
Oncological outcome is the most important issue in cancer surgery. We found no significant differences in tumor size between the two groups. The TNM-based cancer stage was generally upregulated in the 3-LRC group compared to the 5-LRC group. Nonetheless, the proximal and the distal free margins were greater in the 3-LRC group without any positive margin in either group. The harvested numbers of lymph nodes in the 3-LRC and the 5-LRC groups were 28.2 and 22.5 in this study, respectively, which were higher than the minimum of 12 required for accurate staging. 18 These results suggest that the 3-LRC group contained a higher number of cases of obstruction and a higher rate of emergency operation, and therefore, more advanced stages, which lead to longer margins and additional harvested lymph nodes. We found that the 3-LRC group did not lag behind the 5-LRC group in oncological outcomes.
This study has a few limitations. First, only 1 author, the corresponding author, performed the 3-LRC, and the remaining 3 surgeons performed only the 5-LRC. However, all of the above 4 surgeons are experts in colorectal surgery. Second, it was retrospective and not based on randomization of surgical techniques or patients. Finally, the relatively small sample size and small-sized center study were additional limitations. Therefore, large-scale prospective studies of short- and long-term outcomes of 3-LRC are needed to fully demonstrate the benefits of 3-LRC compared with 5 LRC.
In conclusion, despite the reduced number of ports compared with 5-LRC, 3-LRC is a feasible and safe alternative without any adverse oncological outcomes and perioperative morbidity in the treatment of right-sided colon cancer. Cost savings due to the reduced number of ports obviating the need for first assist, improvement of cosmesis due to reduced number of incisions, shortening of operation time, effectiveness against bulky tumors, and quick recovery of intestinal function postsurgery are additional advantages. A well-designed prospective randomized trial is needed to provide a more robust assessment of the benefits of 3-LRC.
Footnotes
Disclosure Statement
No competing financial interests exist.