
Abstract
Abstract
Introduction:
Few centers worldwide have advanced single-incision pediatric endosurgery (SIPES) splenectomy. The safety and feasibility of SIPES performed by trainees were not assessed before. SIPES splenectomy is a demanding technique that needs high level of skills. This is the largest series of 39 SIPES splenectomies performed by 14 trainees in one single center.
Aims:
To assess the safety, feasibility, and technical challenges of SIPES splenectomy performed by trainees and to compare it with other published series.
Materials and Methods:
Retrospective study of all patients operated with SIPES splenectomy for 7 years. SIPES port was inserted through 1.5 cm umbilical incision. One type of port and straight regular instruments were used in all cases.
Results:
Forty-nine patients underwent SIPES splenectomy. Eighty percent was done by our trainees. Six cholecystectomies were done simultaneously. Forty-five patients with sickle cell disease, two with thalassemia, one spherocytosis, and one Fanconi's anemia. Mean operative time (MOT) for splenectomy was 182 minutes (130–190) and 251 minutes for splenectomy with cholecystectomy (230–270) depending on severity of adhesions and size of the spleen; P value <.001. Two conversions have to be opened due to bleeding. There is neither wound infection nor incisional hernia up to date.
Conclusion:
SIPES splenectomy is safe and feasible when performed by surgical trainees without adding any morbidity to the patient. Learning curve can quickly improve with more exposure of trainee to different SIPES procedures and hands-on workshops. More than one procedure could be done at the same time. It has excellent cosmesis and almost invisible scar.
Introduction
M
Aims
To assess the safety, feasibility, and technical challenges of SIPES splenectomy performed by trainees and to compare it with other published series.
Materials and Methods
This is a retrospective study of all patients who underwent SIPES splenectomy from April 2011 to August 2017. After induction of general anesthesia and endotracheal intubation, patients were placed in supine position with left side tilted 30°. SIPES port was inserted through transumbilical single incision of 1.5 cm. Covidien (Medtronic) 12–15 mm port was used in all cases. Pneumoperitoneum has been created and maintained at a constant pressure of 10–12 mmHg. Three millimeters extra port was inserted in left flank for splenic retraction. Long 50 cm laparoscope and straight regular instruments were used in all procedures. Dissection was performed by LigaSure in four stages: division of splenocolic ligament at lower pole, dissection of vascular hilum, division of short gastric vessels, and detachment of diaphragmatic ligaments. The spleen was retrieved in a plastic bag from umbilicus after morcellation with Pean forceps.
Results
Total of 49 patients underwent SIPES splenectomy by 18 surgeons. Thirty-nine (80%) were done by 14 trainees. Twenty-five (51%) were boys and 24 (49%) were girls. Mean age was 6.9 years (2.5–14.8 years). Six cholecystectomies were done simultaneously. The underlying pathology was sickle cell disease in 45 patients (91.8%), thalassemia in two, spherocytosis in one, and Fanconi's anemia in one. Mean HbS for sickle cell disease was 36.86% (19.80–51.50). Mean operative time (MOT) was decreasing yearly, it was 237 minutes in 2011 and declined to 160 minutes by 2017 (Fig. 1). MOT for splenectomy was 182 minutes (130–190) and 251 minutes (230–270) for splenectomy with cholecystectomy; P value <.001 (Fig. 2). We have two conversions to open due to bleeding. There is neither wound infection nor incisional hernia up to date.

MOT per year. MOT, mean operative time.
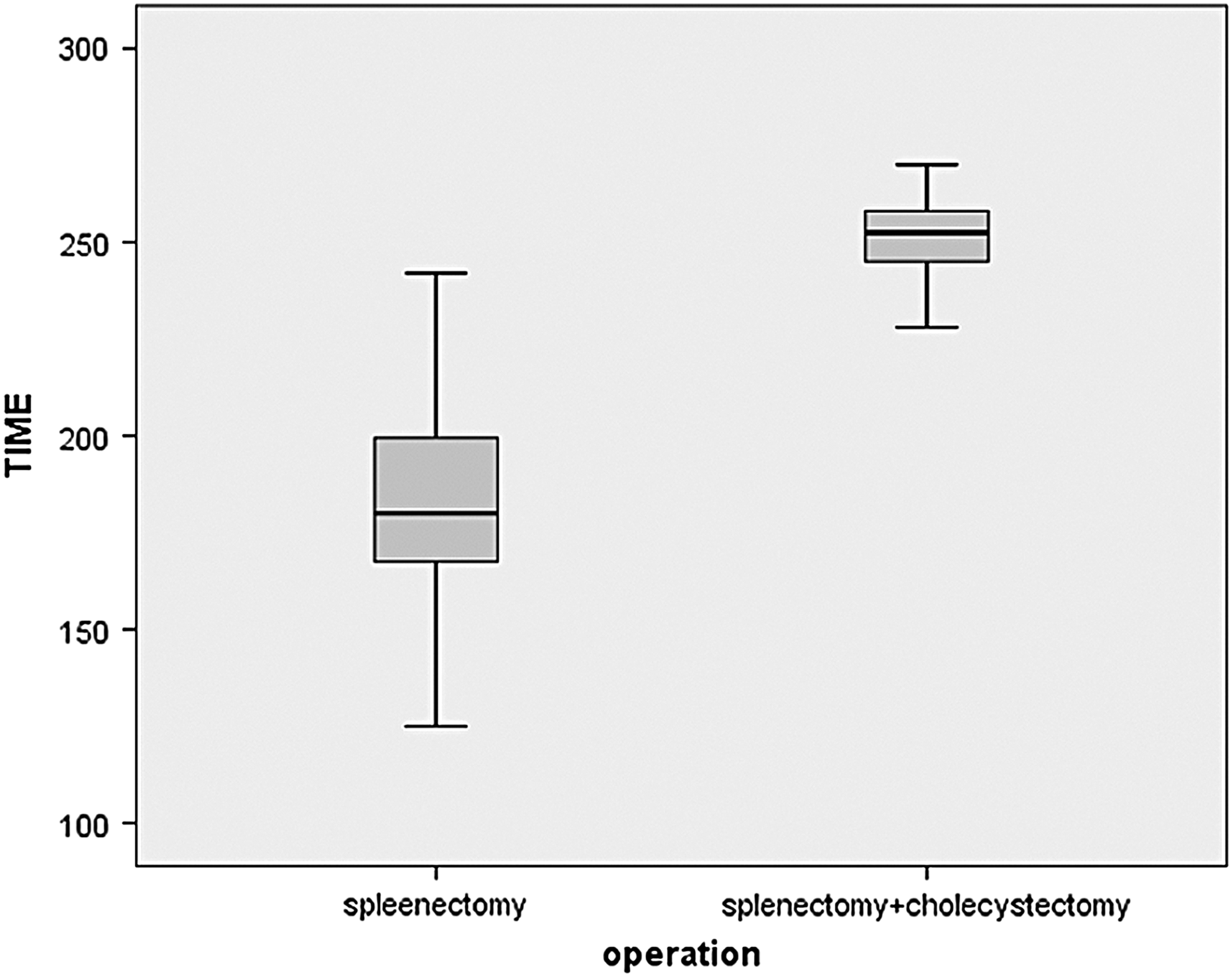
MOT of splenectomy alone and splenectomy with cholecystectomy. MOT, mean operative time.
Discussion
Laparoscopy has revolutionized surgical treatment, as “scarless surgery” is highly demanded by patients and their families especially in younger age group. Barbaros and Dinççağ published the first 2 adult cases of single-incision splenectomy in 2009. 7 Dutta reported the first pediatric SIPES splenectomy in 2012. 1 Few centers worldwide have advanced SIPES recently.4,6,8–17 Up to our knowledge this is the largest study of 39 SIPES splenectomies, which were performed by 14 different surgical trainees in one single center. SIPES splenectomy is rapidly gaining popularity, 4 and our aim is to standardize this approach in pediatric age group.
SIPES has been introduced in our unit in 2008 and it became our standard technique for many procedures such as cholecystectomy, splenectomy, appendectomy, Mitrofanoff, ovarian cystectomy, and fundoplication since 2011. We have performed >500 SIPES cases up to date.
There are many types of ports with different sizes in the market,5,6,17 and from our experience we have found that Covidien© port is the most suitable one as it is small in size and it can adopt 15 mm port for introducing gastrointestinal anastomosis stapler if needed.4,11 Collision of instruments is considered the main limiting factor for popularizing this technique. Other surgeons overcame this problem by using articulating instruments and angled tip fiber optic camera. 17 The use of articulating instruments was difficult and almost impossible in small age group due to narrow and small working space, so we have replaced it by straight instruments. Cameraman can stand away from the operating surgeon by using long 50 cm laparoscope.
One of the important advantages of SIPES is the good access for retrieving large-sized spleen through the umbilicus, instead of Pfannenstiel–Kerr incision used in conventional laparoscopic splenectomy. Extra 3 mm port was inserted in left upper quadrant for splenic retraction to facilitate hilar dissection; it has no effect on the cosmesis (Fig. 2). There is some argument about the use of extra port that it contradicts the concept of SIPES. There are some options to replace this port by using tug-exposure or suture suspension techniques.15,18 We have started to use this technique recently.
Our MOT was longer at the first 3 years of our series (Fig. 1), but nowadays it is almost comparable to other published series (Table 1).4,6 Cholecystectomy, when done simultaneously with splenectomy, did not add more morbidity although the MOT was longer (Fig. 3).

Photo 6 months postoperative scar.
MOT, mean operative time; SILS, single-incision laparoscopic surgery; SIPES, single-incision pediatric endosurgery.
Surgeons performing SIPES should have minimal invasive surgery skills and should attend advanced SILS workshops. We are providing our trainees with advanced laparoscopic and SILS animal workshop in our institution. The trainees are doing many SIPES procedures during their rotation, such as appendectomies, cholecystectomies, and splenectomies. Although our rotating trainees did not have previous experience in SILS, as we are the only SILS center in the region, by the end of their rotation they will be able to perform SIPES safely.
Conclusion
SIPES splenectomy is safe and feasible when performed by surgical trainees without adding any morbidity to the patient. The effects of instrumental crowding, as well as the absence of triangulation, are among the common technical challenging issues. The confusion of crossing image will be adapted after the first 10–15 minutes.
Trainee's learning curve can be improved with exposure to different SIPES procedure under supervision of experienced mentor. The advantages of SIPES are excellent cosmesis with almost invisible scar and more than one procedure could be done at the same time. SIPES splenectomy is now the standard technique in our unit, and we are recommending it with caution as an excellent approach for splenectomy. We agree with others that SIPES is a more demanding surgical technique for the surgeon and is having a greater risk for complications. We recommend surgeons to attend many simulation and/or animal laboratories and start with simpler procedure before starting off SIPES splenectomy.