
Abstract
Abstract
Extrahepatic congenital portosystemic shunts (CPSSs) can be occluded by surgical or endovascular approaches. However, when the estimated portal vein (PV) pressure after the closure is high enough to induce symptoms associated with portal hypertension, partial closure is recommended to avoid life-threatening events. In this study, we attempted laparoscopic partial closure of a CPSS in two patients. Along with intraoperative real-time measuring of the PV pressure and angiography, laparoscopic partial closure was performed to achieve a PV pressure of ≤25 mmHg. Subsequently, the intrahepatic portal system grew in both patients. The partially ligated CPSS closed spontaneously in the first patient. In the second patient, laparoscopic complete closure was performed for the residual CPSS 6 months after the first operation. To our knowledge, this is the first report of laparoscopic partial closure for CPSS. Minimally invasive laparoscopic partial ligation of CPSS is technically feasible and useful when the estimated PV pressure is too high to tolerate one-step complete closure.
Introduction
Congenital portosystemic shunts (CPSSs) are a rare disease entity1–3 originally described by Abernethy in 1793 4 that potentially led to serious complications, such as encephalopathy, hepatopulmonary syndrome, and pulmonary arterial hypertension. 5 It is well known that closure of the shunt allows subsequent growth of the portal vascular system and prevents or even reverses such serious complications.6,7 Although the intrahepatic shunt must be occluded using an endovascular approach,8,9 the methodology of closing extrahepatic shunts varies depending on the location, caliber, length of the shunts, and whether or not they can be closed completely or partially based on the estimated portal vein (PV) pressure afterward.7,10
We herein report two patients with CPSS who underwent laparoscopic partial closure for their shunts. The technical details and the criteria for deciding to perform laparoscopic partial closure approach are discussed.
Case 1
A 4-year-old boy weighing 14.3 kg was admitted for the further workup of his pulmonary hypertension. He had 21-trisomy and had undergone corrective surgery for ventricular septal defect at 4 months of age. Mild hepatic dysfunction with hyperammonemia was noted when he underwent the surgery. Despite the correction of his congenital heart disease, his pulmonary hypertension progressed again. The patient's serum ammonia and total bile acid were 63 μM (normal: <50 μM) and 72.9 μM (normal: <10 μM) on admission. Abdominal computed tomography (CT) revealed a CPSS arising from the portal trunk into the inferior vena cava (IVC) approximately 6 mm in diameter and very short in length (Fig. 1a).
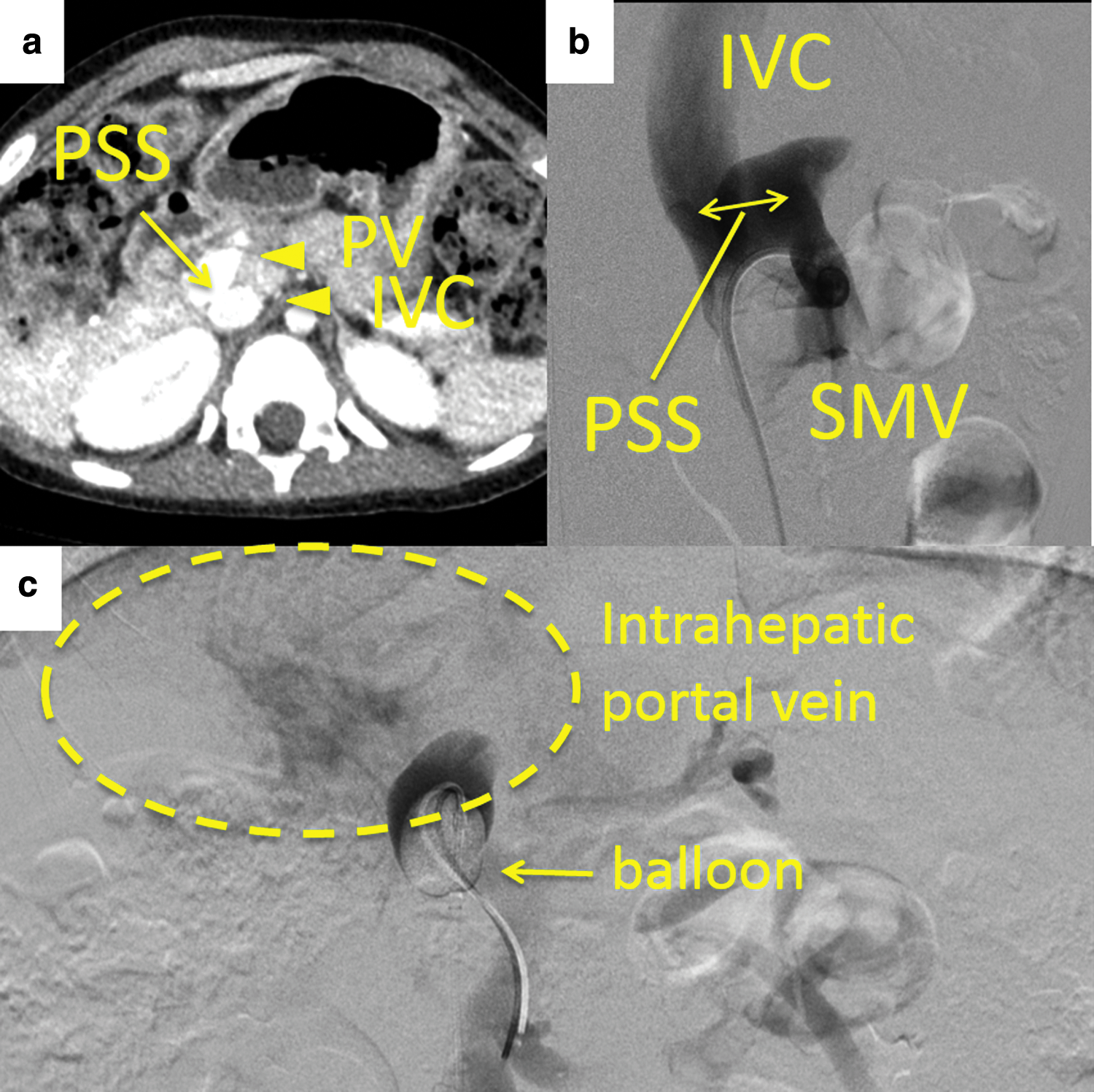
Angiography through the CPSS revealed a severely hypoplastic intrahepatic portal system (Fig. 1b, c), which was only visualized in the setting of test occlusion with a balloon. The PV pressure before, immediately after, and 30 minutes after the temporary occlusion of the shunt with a balloon were 15, 29, and 28 mmHg, respectively. An endovascular approach was not indicated because of the risk of coil migration due to the short length of the CPSS. As the estimated PV pressure after the complete closure was >28 mmHg, which might have caused life-threatening complications associated with portal hypertension, a partial closure approach was attempted.
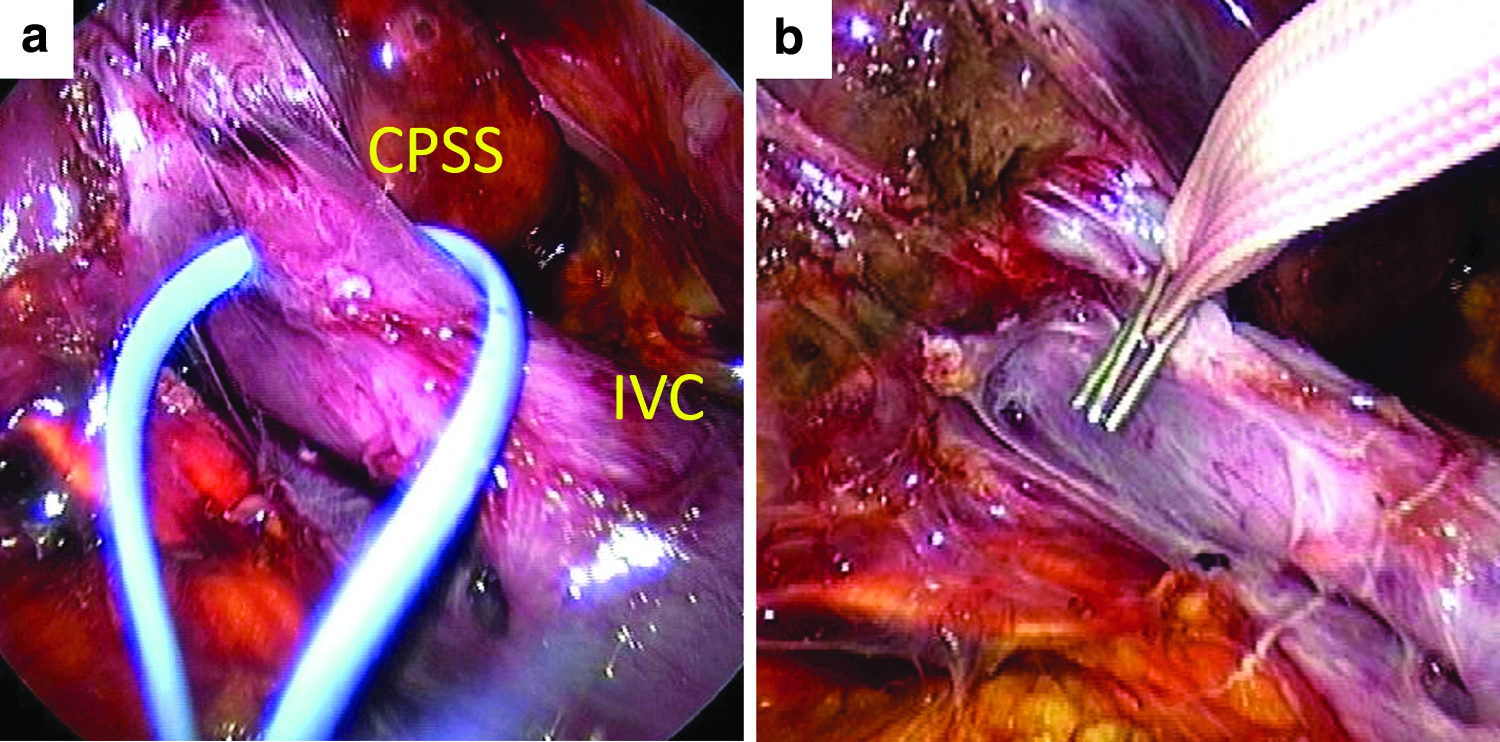
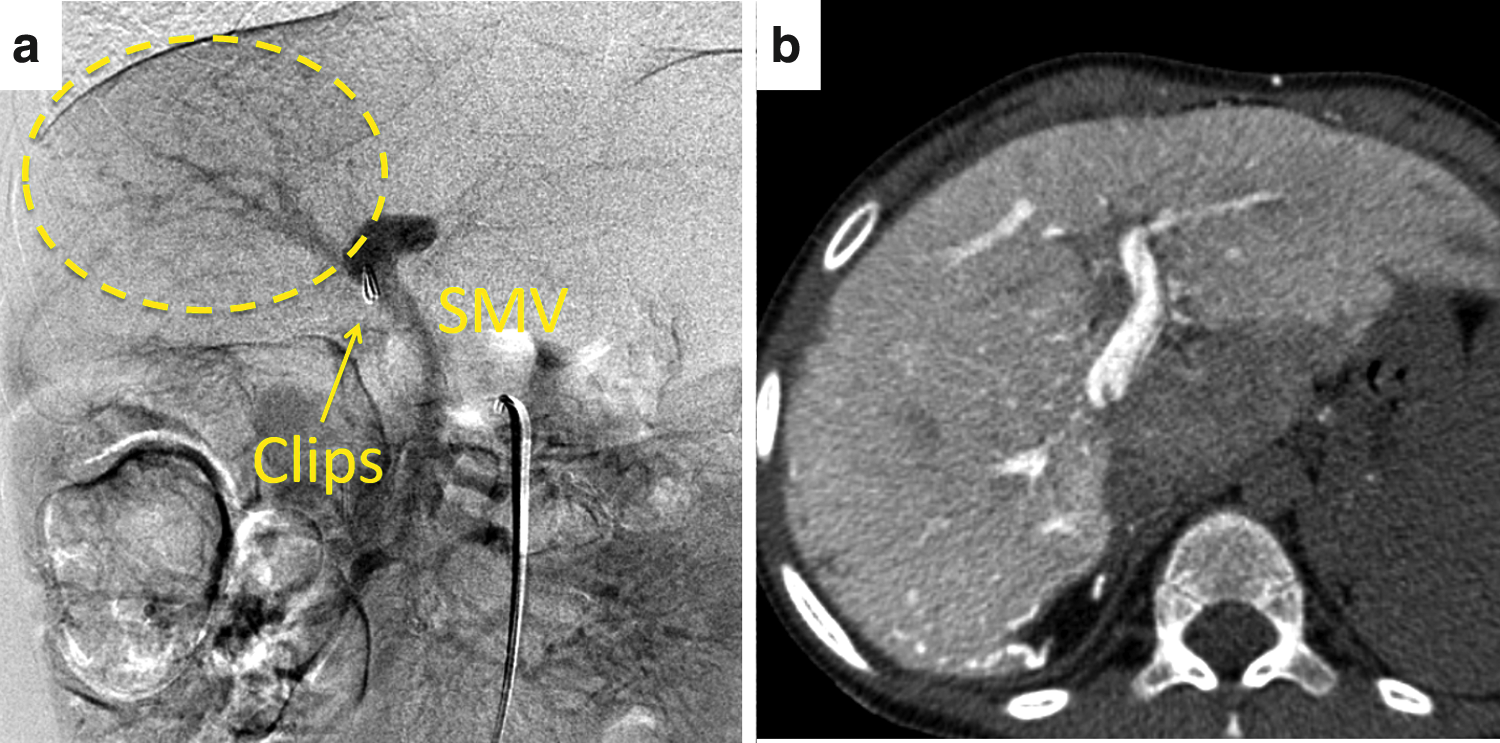
The procedure was performed under general anesthesia with the patient placed in a slight left lateral decubitus position. Before laparoscopy, a catheter was placed retrogradely in the superior mesenteric vein through the CPSS using the IVC from the right femoral vein to monitor the PV pressure. An initial 12-mm port for optics was placed in the umbilical area. The intra-abdominal pressure was maintained below 8 mmHg. At laparoscopy, the liver looked fatty, but the spleen looked normal. Three additional 5-mm working ports were subsequently placed in right lower abdomen, right lateral abdomen, and upper abdomen. The duodenum was first mobilized to expose the IVC. Dissection was then carried out along the IVC, and the CPSS was identified cephalad to the junction of the right renal vein, which was behind the caudate lobe (Fig. 2a). After careful adhesiolysis, the CPSS was encircled using a 5-mm wide piece of tape. While performing PV pressure measurement, clips were applied in stages (Fig. 2b), and when the PV pressure reached 20 mmHg, partial closure was completed. Before the partial closure, 40 units/kg of heparin was administered. Portal angiography through the catheter confirmed that the CPSS was partially closed, and the intrahepatic portal vein was visualized (Fig. 3). We carefully checked that the bowel loops did not look congested.

Portography after applying clips confirmed that the shunt vessel was partially closed, and both the IVC and intrahepatic PV were visualized.
The operative time was 240 minutes. No major intraoperative complications were encountered, and the postoperative course was uneventful. After the operation, heparin was intravenously administered to prevent PV thrombosis, with the activated partial thromboplastin time (APTT) being controlled between 45 and 55 seconds. Dynamic CT performed on the seventh postoperative day revealed a growing portal system without thrombus or ascites. Subsequently, heparin was switched to warfarin with a target international normalized ratio of prothrombin time between 1.5 and 2 international unit (IU). The values of ammonia decreased from 76 μM (before) to 15 μM (after), and the total bile acid was normalized from 95.7 μM (before) to 11.5 μM (after). Angiography from the superior mesenteric artery 4 months after the partial closure showed that intrahepatic portal system had grown significantly, and the partially ligated CPSS had been completely occluded spontaneously (Fig. 4). After angiography, warfarin was discontinued. A histological examination of liver biopsies indicated improvements in fibrosis and steatosis. Importantly, the main pulmonary arterial pressure decreased from 37 mmHg (before) to 31 mmHg (6 months) and 25 mmHg (12 months) after the intervention. No signs of portal hypertension have been observed.
Portography
Case 2
The second patient was a 4-year-old girl weighing 9.3 kg when CPSS was diagnosed. At another hospital, the patient was noted to have hypergalactosemia after birth, and she subsequently developed acute encephalopathy at 2 years of age, with hepatic dysfunction with hyperammonemia (250–350 μM) observed. She was then treated conservatively with protein restriction by changing to enteral nutrition thereafter.
The patient's serum ammonia and total bile acid values were elevated at 60 μM (normal: <50 μM) and 253.3 μM (normal: <10 μM) at the first visit. Abdominal CT identified a CPSS, specifically a ductus venosus type, that was approximately 7 mm in diameter (Fig. 5a). Angiography through the CPSS revealed a rudimentary intrahepatic portal venous system (Fig. 5b). The PV pressure increased to 40 mmHg from 15 mmHg after temporary occlusion of the shunt with a balloon. Since the estimated PV pressure after the occlusion was high enough to risk the appearance of complications secondary to portal hypertension, partial closure of the CPSS was planned. As an endovascular approach for partial closure was technically challenging and irreversible, we opted for a laparoscopic approach.

The procedure was performed under general anesthesia with the patient placed in a supine position. Before laparoscopy, a catheter was placed retrogradely in the superior mesenteric vein through the CPSS. An initial 12-mm port for optics was placed in the umbilical portion, and three additional 5-mm working ports were placed in the bilateral abdomen and below the right costal arch. At laparoscopy, the liver and spleen appeared normal. The CPSS was identified inside the lesser omentum (Fig. 6a) and completely encircled using a 5-mm-wide piece of cotton tape, with clips applied in stages. When the PV pressure reached 25 mmHg, partial closure was completed (Fig. 6b). As the intraoperative activated coagulation time was over 200, heparin was not administered.
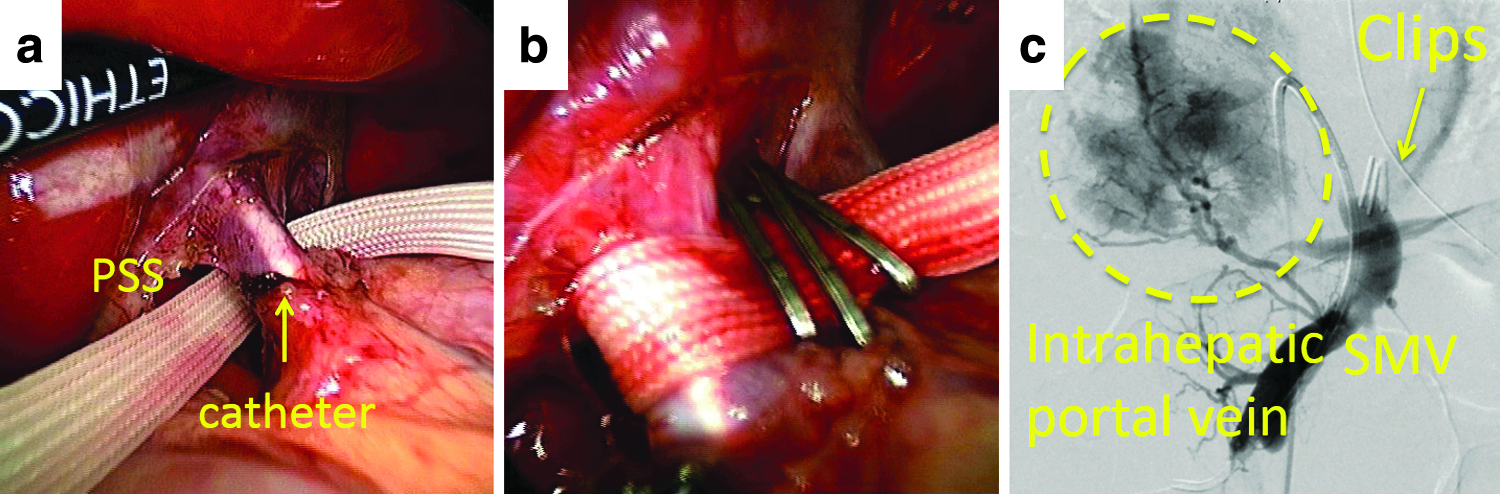
Portography findings after the partial closure of the CPSS are shown in Figure 6c. The operative time was 145 minutes. No major intraoperative complications were encountered, and the postoperative course was uneventful. After the operation, heparin was intravenously administered to prevent PV thrombosis, and the APTT was controlled with a target of 45–55 seconds. Dynamic CT on the seventh postoperative day demonstrated the patent portal venous system without thrombus or ascites. Portography from the superior mesenteric artery 4 months after partial closure showed significant growth of the intrahepatic portal venous system and the narrowed residual CPSS (Fig. 7).
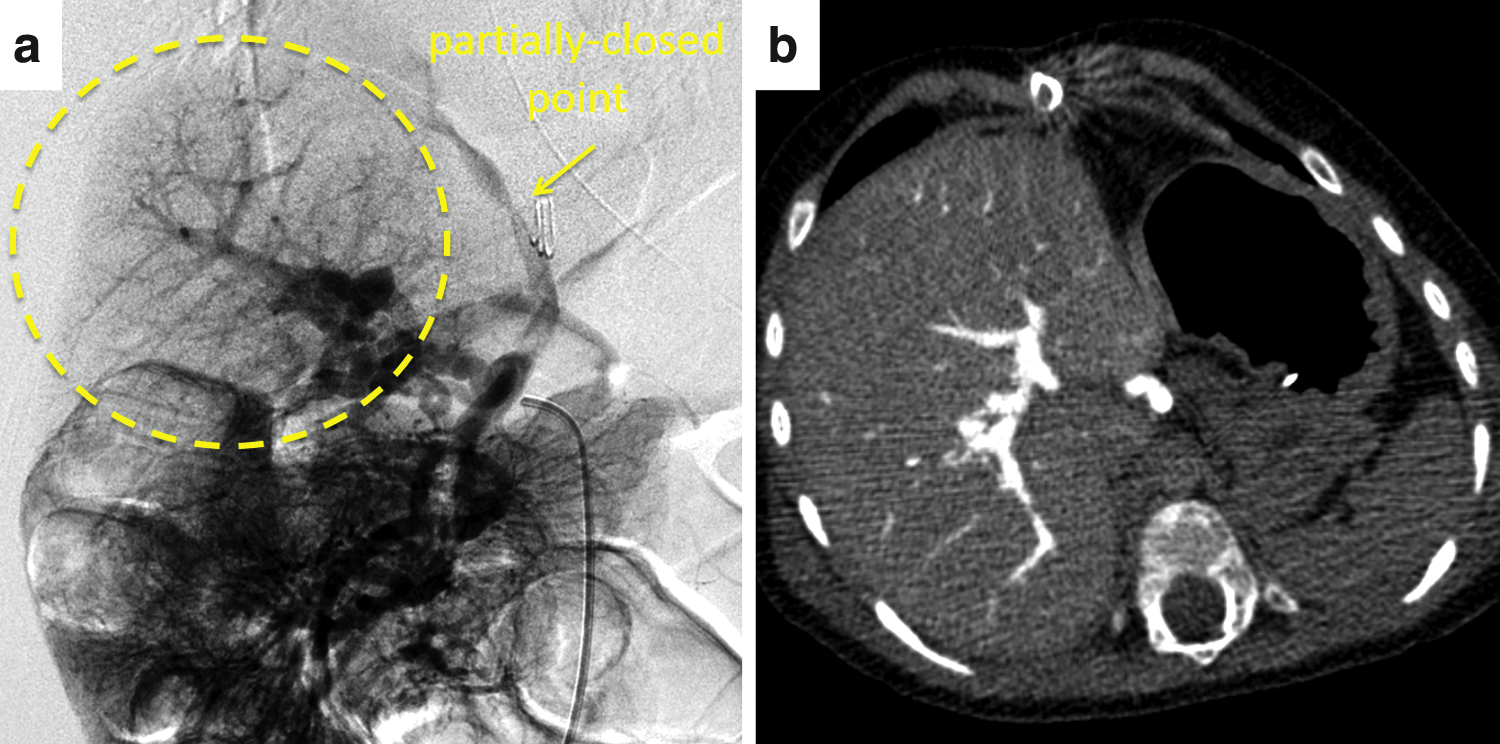
Portography from the SMA 4 months after partial closure shows the significant growth of the intrahepatic portal venous system
Complete closure by a laparoscopic approach was performed 6 months after the first intervention (Fig. 8). The estimated PV pressure obtained as the hepatic vein-wedged pressure was 6 mmHg, and it did not rise after complete ligation. The values of ammonia decreased from 104 μM (before) to 19 μM (after complete closure), and the total bile acid level normalized from 238.4 μM (before) to 9.2 μM (after complete closure). A pathological examination of needle-based liver biopsies before and after complete closure also revealed the growth of the portal venous system. The patient tolerated the procedures well, and no symptoms of liver dysfunction or encephalopathy recurred during the following 6 months.

Complete closure in the second laparoscopic approach. The residual CPSS was closed directly using clips.
Discussion
The treatment strategy of CPSS depends on the patient's age, symptoms, location and length of the shunt, and the estimated rise in PV pressure after closure.6,7,11,12
Once the decision to close a CPSS is made, estimation of the PV pressure after ligation is the top priority. If the estimated PV pressure after complete ligation is deemed too high, two-step closure is recommended to avoid symptoms associated with a sudden increase in the PV pressure. Choosing two-step closure is based on several criteria, including the absolute values of PV pressure and PV pressure gradient obtained through test occlusion. The visual presence of intestinal congestion after complete ligation is also an important indicator. 13 Regarding the absolute values of PV pressure, the upper limits for one-step closure are reported to range from 22 to 32 mmHg,7,13,14 while one-step closure is deemed feasible if the PV pressure gradient is <15 mmHg.5,12
However, there is a report of a new shunt forming postoperatively when the PV pressure gradient exceeded 11 mmHg. 15 Furthermore, in another report, one-step closure through an endovascular approach for patients with a severely hypoplastic portal system, defined as little or no visualized intrahepatic portal system by the occlusion test, resulted in sepsis associated with portal hypertension after the procedure. 16 Based on these findings, our institution selects two-step closure if the absolute value of PV pressure is >25 mmHg or the PV pressure gradient is >10 mmHg.
In such cases, either an endovascular or a surgical approach is the viable choice. 11 When deciding on either approach, two factors need to be taken into consideration. First, when the CPSS is short, an endovascular approach carries a risk of migration of material. 11 Second, if two-step closure is regarded as necessary for the above reasons, endovascular two-step closure is technically challenging. Knirsch et al. reported the details of two-step closure using IVR approach. 12 Two different diabolo-shaped covered stents were used to reduce the shunt flow by creating a stenosis. However, for technical reasons, these procedures require a personalized device suitable for partial closure, and the strategies can be quite sophisticated. 12
Minimally invasive laparoscopic ligation of CPSS has been reported to have good outcomes.13,17,18 However, no cases of partial closure using laparoscopic approaches have been reported. We opted for laparoscopic partial closure for the two patients in the present study for several reasons, as described below.
In the first patient, the length of the CPSS, as indicated by the distance between the main portal trunk and the IVC (Fig. 1a), was too short to be embolized using an endovascular approach without affecting the blood flow at either the PV or IVC. In addition, a preoperative endovascular occlusion test suggested that there would be a significant increase (from 15 to 28 mmHg) in the PV pressure, prompting concern about performing one-step complete closure. In the second patient, although the length of the CPSS was long enough to be embolized using an endovascular approach, the PV pressure after the closure was estimated to exceed 40 mmHg; we therefore opted for a partial closure method due to concerns that irreversible closure might cause life-threatening events. From a technical perspective, 5-mm-wide cotton tape with surgical clips was used for both patients and left inside the body without complications. Alternatively, Gore-Tex® might be more useful for minimizing adhesion and the foreign body response.
Anticoagulative strategies are also essential parts of the treatment. In these two patients, we achieved an activated clotting time (ACT) of over 200 intraoperatively just before starting the test clamp. The APTT was then controlled to a value between 45 and 60 for 1 week, followed by conversion to an oral anticoagulant. The appropriate duration of anticoagulation remains controversial. 14 The portal flow (by ultrasound), the presence of ascites, and the fibrinogen degradation product (FDP) levels should be carefully monitored postoperatively. Our first patient was on warfarin for 4 months because the PV was almost invisible on intraoperative angiography after partial closure. Although CT with contrast a week after partial closure revealed a growing PV system with traces of ascites and normal FDP values, we decided to continue anticoagulation just in case. In contrast, the second patient was given no heparin during the operation because the coagulative panels were abnormal (APTT >45 seconds and international normalized ratio of prothrombin time >1.5, before operation).
Regarding the timing of the second step, a 6-month interval after partial closure is recommended. However, this decision depends completely on the intrahepatic portal flow and associated symptoms. In the first patient, as CT with contrast was inconclusive regarding whether or not the CPSS was completely shut, the patient underwent angiography through the superior mesenteric artery to achieve better visualization of the portal system. As the results indicated the complete closure of the CPSS along with a well-grown intrahepatic PV, no further treatment was planned. In contrast, angiography through superior mesenteric artery in the second patient revealed a patent CPSS in a half-occluded manner, so the CPSS was closed completely by laparoscopy 6 months after the first intervention.
In conclusion, laparoscopic partial closure of CPSS is a useful approach when the length of the CPSS is too short for an endovascular approach and the estimated PV pressure is high enough to make surgeons worry about complications associated with portal hypertension.
Footnotes
Disclosure Statement
No competing financial interests exist.