
Abstract
Abstract
Aim:
There is no evidence indicating that survival improvement is associated with anatomical laparoscopic liver resection (ALLR) rather than non-ALLR (NALLR) to treat solitary hepatocellular carcinoma (HCC). The aim of our study was to compare the oncological outcomes of ALLR versus NALLR.
Materials and Methods:
From January 2008 to September 2014, 231 patients underwent LLR as the primary treatment for solitary HCC without portal vein tumor thrombus. After matching one-to-one propensity scores, 118 patients were included in 2 groups: NALLR (n = 59) and ALLR (n = 59).
Results:
In the propensity-matched cohort, the 1-, 3-, and 5-year recurrence-free survival rates were 84.4%, 73.8%, and 68.4% in the ALLR group and 87.7%, 78.7%, and 73.5% in the NALLR group (P = .602). In multivariate analysis, the independent risk factors affecting HCC recurrence were higher preoperative PIVKA-II (prothrombin induced by vitamin K absence or antagonist-II) levels (P = .041) and microvascular invasion (P = .030). The risk factor affecting liver-related mortality was determined to be higher preoperative PIVKA-II levels (P = .007).
Conclusions:
In the propensity-matched cohort, long-term outcomes of the NALLR group were not inferior to those of the ALLR group.
Introduction
E
Although anatomical liver resection is the preferred surgical procedure for HCC, there is little evidence that it offers an improved survival rate when compared with nonanatomical resection (NAR). In this article, we utilized propensity score matching (PSM) analysis to perform comparative analysis of oncological outcomes in HCC patients who underwent ALLR and NALLR. In addition, we assessed the clinical characteristics of recurrent HCC and identified risk factors of recurrence and liver-related mortality in propensity-matched patients who underwent ALLR and NALLR.
Materials and Methods
Study design and population
We retrospectively assessed the data of 247 patients who underwent LLR for solitary HCC at a single institution between January 2008 and September 2014. Patients who underwent previous locoregional treatment, such as transarterial chemoembolization (n = 7) or radiofrequency ablation (n = 5), who were diagnosed with synchronous cancer requiring simultaneous operation (n = 1), and who had preoperative portal vein tumor thrombus (n = 3) were excluded in this study. The remaining 231 patients were included and divided into the NALLR (n = 84) and ALLR (n = 147) groups according to the type of LLR received. To decrease confounding and selection bias of the baseline characteristics in the 2 groups, PSM was utilized at a 1:1 ratio. As a result, 118 patients were involved in both groups of this study: NALLR group (n = 59) and ALLR group (n = 59). The study was approved by the institutional review board of our institution (No. 2017-03-004).
Indications for LLR and resection type for solitary HCC
If solitary HCC was diagnosed by abdominal computed tomography without extrahepatic involvement, liver resection was considered in patients who had preserved liver function with Child–Turcotte–Pugh (CTP) grade A and an American Society of Anesthesiologists (ASA) score <III. 5 The surgeon determined whether to proceed with the open or laparoscopic approach for liver resection. In general, LLR was performed when tumors were 5 mm or more away from major vascular or biliary structures, allowing them to technically secure surgical margins. ALLR was defined as complete resection, using a totally laparoscopic approach, of an anatomical region that was demarcated by preceding ischemia, along with division of the Glisson's capsule, associated with tumor location. In the case of solitary HCC located peripherally or presenting with exophytic growth, NALLR was performed according to the surgeon's preference, and when patients required limited resection due to poor liver function. The surgical procedures of LLR are detailed in our previous study. 6
Study criteria
The main purpose of our study was to compare recurrence-free survival (RFS) and overall survival (OS) in the ALLR and NALLR groups, and to identify risk factors affecting HCC recurrence and liver-related mortality in a propensity-matched cohort of patients who underwent LLR. Tumor location was defined as follows: anterolateral segments were segment 2, 3, 4b, 5, and 6; PS segments were segment 1, 4a, 7, and 8. 7 Major hepatectomy was defined as the removal of three or more segments of the liver. 8 Major vascular proximity was defined as a tumor within 1 cm from the Glisson's capsule or 5 mm from the hepatic vein in the expected transection plane. 9 A subcapsular tumor was defined as a lesion located less than 1 cm from the liver's edge. 10 The histological grade of HCC was assigned according to the Edmondson–Steiner system in addition to being defined as “well differentiated” (W, grade I), “moderately differentiated” (M, grade II), or “poorly differentiated” (P, grade III, IV). 11 Propensity scores were created using demographic factors (age, sex, body mass index, previous abdominal operation, etiology, CTP grade, and ASA score), preoperative laboratory factors (albumin, total bilirubin, aspartate aminotransferase, alanine aminotransferase, prothrombin time international normalized ratio, platelet counts, indocyanine green retention rate at 15 minutes [ICGR15], alpha-fetoprotein, and prothrombin induced by vitamin K absence or antagonist-II [PIVKA-II]), pathological factors (LC, tumor size, histological grade, vascular invasion, surgical margin, and tumor location), and surgical factors (operating time, blood loss, blood transfusion, and open conversion).
Statistical analysis
To adjust for the difference in baseline characteristics between the 2 groups and to decrease possible selection bias, a 1:1 PSM was applied using multiple logistic regression with the nearest-neighbor matching method. Continuous data were presented as mean ± standard deviation. Categorical data were described in numbers and percentages. Statistical analysis was conducted using an independent-samples T-test or a Mann–Whitney test for continuous values and a chi-squared test or Fisher's exact test for categorical values, especially when expected cell frequencies were below five. RFS and OS rates were analyzed via the Kaplan–Meier method. The log-rank test was used to compare 2 survival curves produced from 2 groups. Univariate and multivariate analyses for risk factors affecting HCC recurrence or liver-related mortality following LLR were conducted using a Cox proportional hazard model. A P value below .05 was considered statistically significant. Data handling and analysis were performed using the Statistical Package for Social Science for Windows™ 22.0 release (SPSS, Inc., Chicago, IL).
Results
Baseline demographic, laboratory, pathological, and surgical factors
As demonstrated in Table 1, we assessed baseline factors, including demographic, laboratory, pathological, and surgical factors, in the ALLR and NALLR groups. In the entire cohort of ALLR versus NALLR groups, there was a significant difference in preoperative serum albumin level (4.4 ± 0.4 g/dL versus 4.3 ± 0.5 g/dL, P = .049), ICR R15 (10.3% ± 4.9% versus 13.2% ± 11.0%, P = .024), tumor size (3.1 ± 1.6 cm versus 2.5 ± 1.6 cm, P = .005), proportion of poorly differentiated HCC (10.9% versus 3.6%, P = .028), surgical margin (2.0 ± 1.5 cm versus 1.3 ± 1.0 cm, P < .001), and operating time (308.5 ± 127.0 minutes versus 242.5 ± 109.1 minutes, P < .001).
Patient Characteristics Before and After Propensity Score Matching
Fisher's exact test.
AL segments are 2, 3, 5, 6, and 4b, and PS segments are 1, 7, 8, and 4a.
AFP, alpha-fetoprotein; AL, anterolateral; ALLR, anatomical laparoscopic liver resection; ALT, alanine aminotransferase; ASA, American Society of Anesthesiologists; AST, aspartate aminotransferase; B, hepatitis B; BC, hepatitis B and C; BMI, body mass index; C, Hepatitis C; CH, chronic hepatitis; CTP, Child-Trucotte-Pugh; HCC, hepatocellular carcinoma; ICG R15, indocyanine green retention rate at 15 minutes; M, moderately differentiated; LC, liver cirrhosis; NALLR, non-anatomical laparoscopic liver resection; NBNC, neither hepatitis B nor C; P, poorly differentiated; PIVKA-II, prothrombin induced by vitamin K absence or antagonist-II; PS, posterosuperior; PT INR, prothrombin time international normalized ratio; W, well differentiated.
In 118 cases of propensity-matched cohort, all baseline characteristics were similar in both groups. Mean tumor size was 2.6 cm. There were 62 cases (52.5%) of cirrhotic features in the liver. Tumors were located in the PS segment in 28 cases, at the same proportion (23.7%) in both groups.
Postoperative surgical outcomes and long-term oncological outcomes
The mean follow-up duration of the ALLR and NALLR groups in the propensity-matched cohort was 55.5 ± 26.4 and 62.3 ± 29.5 months, respectively (P = .184). Table 2 summarizes comparison of clinical characteristics for recurrent HCC between the 2 groups. Resection site recurrence occurred in 2 cases (11.8%) and 5 cases (25.0%) in the ALLR and NALLR groups, respectively (P = .416). Intrahepatic recurrence patterns were significantly different in the 2 groups; specifically, ipsilateral intrahepatic recurrence was more prevalent in the NALLR group than in ALLR (6 cases [42.9%] versus 3 cases [16.1%], P = .043).
Clinical Characteristics of Recurrent Tumors in Propensity-Matched Patients with Anatomical Laparoscopic Liver Resection and Nonanatomical Laparoscopic Liver Resection
Fisher's exact test.
ALLR, anatomical laparoscopic liver resection; HCC, hepatocellular carcinoma; NALLR, nonanatomical laparoscopic liver resection; RFA, radiofrequency ablation; TACE, transarterial chemoembolization; TACE+RT, combined treatment of transarterial chemoembolization and radiation therapy.
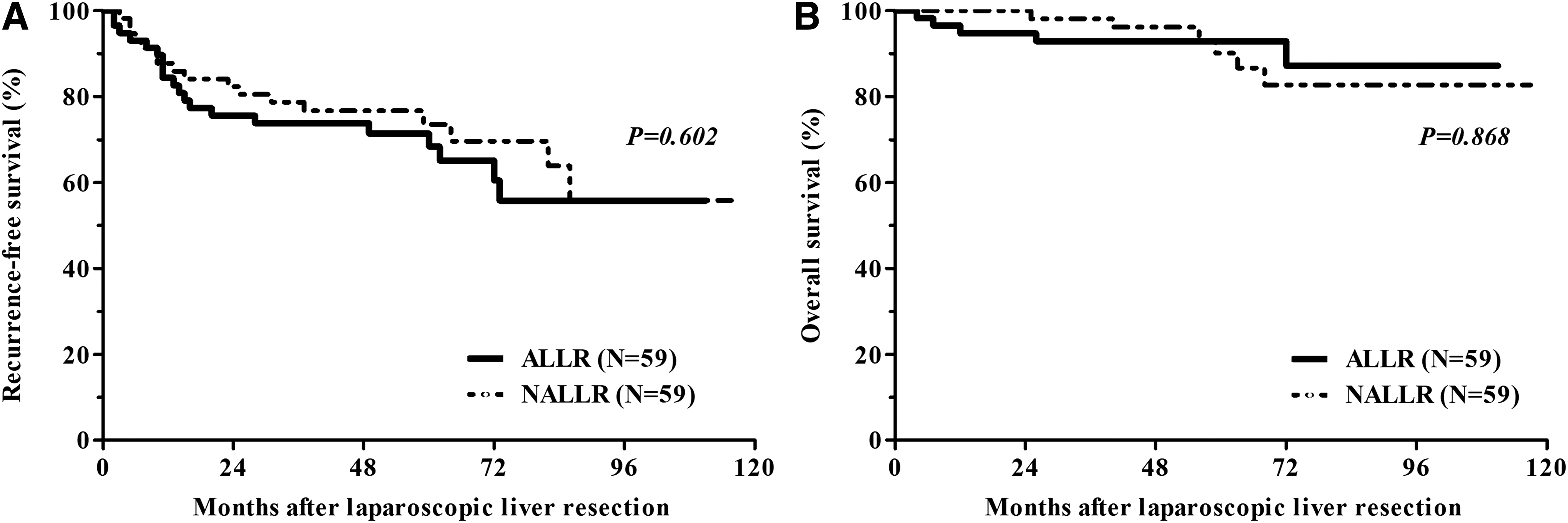
In the entire cohort, the liver-related OS rate in the ALLR group was higher than in the NALLR group, although this trend was not statistically significant (P = .236; Fig. 1). In the propensity-matched cohort, the 1-, 3-, and 5-year RFS rates were 84.4%, 73.8%, and 68.4% in the ALLR group and 87.7%, 78.7%, and 73.5% in the NALLR group. The 1-, 3-, and 5-year liver-related OS rates were 94.8%, 92.9%, and 92.9% in the ALLR group and 100%, 98.2%, and 90.1% in the NALLR group. However, these tendencies of RFS and liver-related OS were not significantly different between the groups (P = .602 and P = .868; Fig. 2).

Recurrence-free survival
Recurrence-free survival
Risk factors for disease-free survival and liver-related mortality
The results of univariate and multivariate analyses for risk factors affecting HCC recurrence and liver-related mortality in propensity-matched patients who underwent LLR are included in Tables 3 and 4. Multivariate analysis revealed that higher preoperative PIVKA-II levels and microvascular invasion were significantly associated with HCC recurrence (P = .041 and P = .030, respectively; Table 3). In the same patient group, the risk factor affecting liver-related OS was determined to be higher preoperative PIVKA-II levels (P = .007; Table 4). NALLR did not correlate significantly with HCC recurrence or liver-related mortality (P = .598 and P = .860, respectively).
Univariate and Multivariate Analysis of Risk Factors for Hepatocellular Carcinoma Recurrence in Propensity-Matched Patients Who Underwent Laparoscopic Liver Resection
AFP, alpha-fetoprotein; AL, anterolateral; ALT, alanine aminotransferase; CI, confidence interval; ICGR15, indocyanine green retention rate at 15 minutes; NAR, nonanatomical resection; PIVKA-II, prothrombin induced by vitamin K absence or antagonist-II; PS, posterosuperior; PT INR, prothrombin time international normalized ratio.
Univariate and Multivariate Analysis of Risk Factors for Liver-Related Mortality in Propensity-Matched Patients Who Underwent Laparoscopic Liver Resection
AFP, alpha-fetoprotein; AL, anterolateral; ALT, alanine aminotransferase; CI, confidence interval; ICGR15, indocyanine green retention rate at 15 minutes; NAR, nonanatomical resection; PIVKA-II, prothrombin induced by vitamin K absence or antagonist-II; PS, posterosuperior; PT INR, prothrombin time international normalized ratio.
Discussion
Liver resection is the primary treatment considered for HCC patients with good liver function. 12 However, the long-term survival rate is unsatisfactory due to the high recurrence of HCC even after a curative procedure.13,14 Because HCC tends to invade intrahepatic vascular structures and is often close to the portal vein, 15 anatomical resection (AR), including the area covered by the tumor-feeding portal vein, was proposed in the 1980s as a theoretical therapeutic surgical method. 16
It is difficult to reach any conclusions when comparing the oncological outcomes of patients who underwent AR and NAR for HCC because of the substantial differences between the 2 groups. In previous studies, patients in the NAR group had more impaired liver function than those in the AR group, and tumors of those in the NAR group tended to be more progressive than of those in the AR group.17–19 Some studies have suggested that, for HCC, AR is superior to NAR.17,20,21 However, other studies comparing the OS of patients with solitary HCC smaller than 5 cm indicated that the oncological outcomes of patients who underwent NAR were comparable with those of patients who underwent AR.22,23 Therefore, it is still unclear what the optimal approach is for liver resection in patients with solitary small HCC and poor liver function.
To reduce the potential bias of factors that influence HCC recurrence, we performed PSM, including tumor size, grade, LC, and ICGR15, among others. In our PSM-matched cohort of 118 patients who underwent LLR, the tumors of 114 patients (97%) were less than 5 cm in size, and 115 patients were found to have chronic hepatitis (53 patients, 45%) or LC (62 patients, 53%). Our cohort demonstrated that there was no significant difference between the ALLR and NALLR groups in RFS and liver-related OS rates.
Once the use of LLR for HCC began, technical considerations for performing AR have become important. First, inexperienced surgeons must overcome the learning curve of using a minimally invasive approach for liver resection. To complete ALLR, the surgeon must first understand the anatomy of hepatic vessels and adequately manage new laparoscopic instruments, including a flexible laparoscope, laparoscopic stapler, and ultrasonic shears. Glissonian pedicle control is also important to minimize bleeding or bile leakage, and to identify a demarcation line for the transection plane. Contrary to OLR, tumor localization is difficult in LLR because tumors in the deep areas of the liver cannot be identified by touch. Surgeons performing LLRs should make full use of intraoperative ultrasonography to overcome the difficulties of locating the tumor and identifying the transection plane. 24 Beginners may hesitate to perform ALLR, as these issues make it a technically challenging procedure.
Tumor extent and remnant liver function determined whether ALLR or NALLR was performed. At our institute, NALLR did not just comprise enucleation of the tumor, but was based on the concept of a wide excision involving sufficient surgical margin. Multivariate analysis of our PSM-matched cohort demonstrated that undergoing NALLR rather than ALLR was not an independent risk factor affecting HCC recurrence. Significant risk factors associated with HCC recurrence were PIVKA-II (P = .042) and microvascular invasion (P = .030), which had previously been identified as risk factors for early recurrence after hepatectomy.25,26 This implies that HCC recurrence after LLR may be influenced by tumor biology rather than the procedure of anatomical resection, provided a sufficient surgical margin was achieved.
Although our study was well balanced by PSM, the small sample size of the ALLR and NALLR groups is a major limitation. In addition, our study was conducted as a preliminary report with a relatively short follow-up period to assess oncological outcome after curative laparoscopic hepatectomy. Further studies with long-term follow-ups in a larger cohort are necessary to confirm our results.
In conclusion, we determined that when using PSM to adjust potential clinical differences in oncological outcome after curative laparoscopy in HCC, the long-term outcomes of patients in the NALLR group were not inferior to those of patients in the ALLR group. Multivariate analysis showed that NALLR was not a risk factor for HCC recurrence and liver-related mortality. Our study establishes that NALLR, when conducted with a safe surgical margin, can be considered for patients with solitary small HCC and poor liver function when ALLR is not feasible.
Footnotes
Acknowledgment
This work was supported by the 2018 Yeungnam University Research Grant.
Disclosure Statement
No competing financial interests exist.