
Abstract
Abstract
Purpose:
Traditional intersphincteric resection is a technically demanding procedure that required a perineal approach dissection and a handsewn coloanal anastomosis. Our study was to investigate the feasibility and the prognostic factors of completely abdominal approach partial intersphincteric resection (APISR) after neoadjuvant chemoradiotherapy (CRT) for low rectal cancer with initial stage cT3.
Methods:
A total of 101 consecutive patients with initial stage cT3 juxta-anal rectal cancer who underwent APISR after neoadjuvant CRT between January 2010 and March 2015 were enrolled. Survival rates were estimated and compared using the Kaplan–Meier method and log-rank tests. Cox proportional hazard model was utilized for multivariable analysis for disease-free survival (DFS). The cutoff values of residual tumor size calculated by X-tile were used in the multivariate analysis as well.
Results:
The median follow-up was 39 months. The local recurrence rate within 3 years was 2.5%. The 3-year DFS rate was 80.2%, and the 3-year overall survival rate was 95.3%. The 3-year DFS in pathological stage 0–III were 96.2%, 94.4%, 85.7%, and 44.7% respectively (Log-rank = 29.791, P < .001). In multivariate analysis, stage ypN1-2 (hazard ratio (HR) = 8.256, 95% confidence interval [CI]: 2.742–24.855, P < .001) and tumor size after CRT more than 2.8 cm (HR = 3.077, 95% CI: 1.036–9.137, P = .043) were the independent factors for worse DFS.
Conclusions:
Laparoscopic and open APISR after CRT produces satisfactory mid-term oncological outcomes for juxta-anal rectal cancer downstaged from initial cT3 especially in stage ypN0 or with tumor size after CRT <2.8 cm. Hence, stage ypN1–2 and tumor size after CRT more than 2.8 cm are poor prognostic factors that should be estimated for APISR.
Introduction
A
Partial ISR for juxta-anal tumors remains technically demanding for surgeons in the small field of vision due to the sphincter complex structures of the long “tube within a tube.”12,13 For obese patients with bulky tumors in the narrow pelvis, a transanal total mesorectal excision is usually required.14,15 In the era of minimally invasive surgery, laparoscopy and robotic system facilitate the accomplishment of ISR by a completely abdominal approach in some experienced centers.16–19 Abdominal approach partial intersphincteric resection (APISR) with laparoscopic surgery in our institute was described in 2010 in China, and the midterm favorable results were reported in 2015. 18 However, there were few studies on the oncological outcomes of APISR for juxta-anal rectal cancer after CRT. This study was to evaluate the feasibility and prognostic factors of APISR for cT3 juxta-anal rectal cancer after downstaging by CRT.
Methods
Patients
This was a retrospective cohort study of a prospectively collected data from the database in Department of Colorectal Surgery, Fujian Medical University Union Hospital. A total of 101 consecutive patients who underwent APISR after CRT were enrolled from January 2010 and March 2015. The inclusion criteria were as follows: (1) low rectal cancer within 1 cm above the anorectal ring; (2) tumors with the initial clinical stage T3, with or without suspected regional lymph node involvement according to high-resolution magnetic resonance imaging (MRI) and endorectal ultrasonography before radiotherapy; (3) post-CRT clinical stage was not more than ycT3 without threatening mesorectal fascia according to MRI. The patients who received short-term radiation, those with fecal incontinence before surgery, invasion of external sphincter, levator muscles, or adjacent organs, suspected lateral pelvic lymph node involvement, or distant metastases were all excluded from this study.
Treatment regimens
Neoadjuvant long-course radiotherapy consisted of 50.4 Gy delivered in fractions of 1.8 Gy with five fractions per week for five consecutive weeks followed by a 5.4-Gy boost. Concurrent CRT was administered including two different regimens as follows: (1) Four cycles of Capecitabine and Oxalipatin regimens: oxaliplatin 130 mg/m2 intravenous on day 1, and capecitabine 1000 mg/m2 twice daily days 1–14 every 3 weeks; (2) capecitabine 825 mg/m2 for 25 days, followed by 1–2 cycles of capecitabine 1000 mg/m2 for 14 days with a 7-day interval. The APISR was performed 8–10 weeks after the end of the radiation.
Surgical procedures
As was described previously, an APISR was performed by the top-down approach. The surgical procedures included the following five steps: high ligation of inferior mesentery artery, proximal mobilization of the left colon (including the splenic flexure if necessary), total mesorectal excision (TME), intersphincteric dissection, and diverting stoma, 18 as were shown in Figure 1.
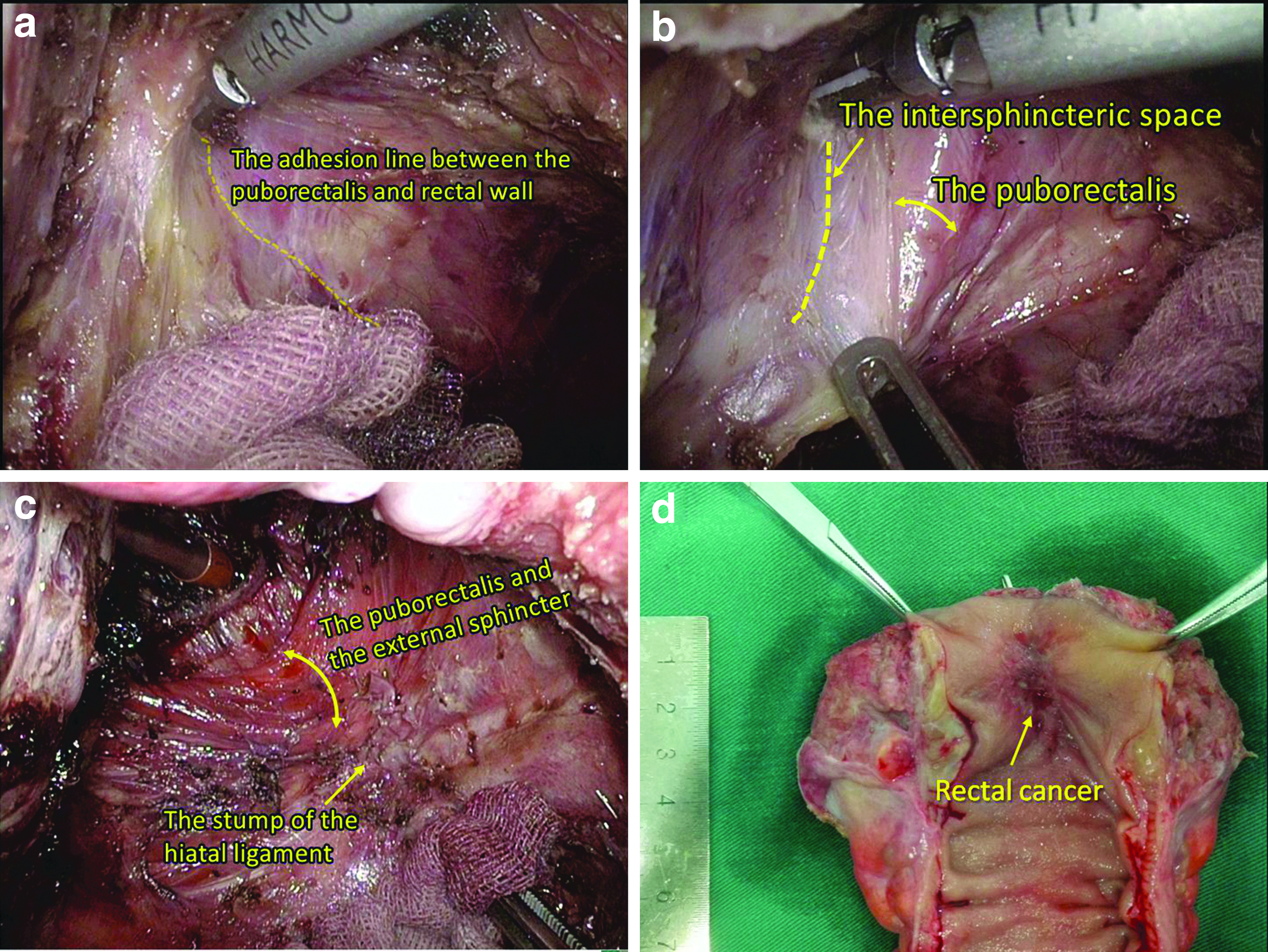
Completely abdominal approach partial intersphincteric resection for low rectal cancer after chemoradiotherapy: The adhesion line between the puborectalis and rectal wall is exposed and the dissection in the intersphincteric space continues at the lateral side of the rectum from the abdominal side
A standard TME was accomplished taking care to protect the hypogastric nerves and neurovascular bundles. The embryonic plane between the rectum and the surrounding levator sphincter muscles was clearly identified from the abdominal side. 20 The procedure of APISR was shown in Figure 1. Intersphincteric dissection between the rectum and the puborectalis was carried out distally from the lateral to the posterolateral side. After that, circular dissection moved to the posterior side distally to the hiatal ligament, which was then transected just close to the rectum. The dissection of the intersphincteric space was continued caudally at the anterior side of the rectum. The low rectum was mobilized for 2–3 cm from the inferior margin of the tumor to ensure a 1 cm distal margin. The inferior margin of the tumor should be checked accurately by digital examination. A titanium clip or a suture on the bowl wall was applied to mark the lower edge of the tumor. A 3-cm silk thread was used to measure the planned length of distal margin. The rectum should be washed out before stapling. Two 45-mm flexible linear staplers were fired with the cutting line lower than the upper edge of the puborectalis. After checking distal margin of the specimen, a stapled end-to-end coloanal anastomosis was constructed without any tension. The anastomoses were at the dentate line. In laparoscopic surgery, the specimen was removed from the planned incision for the stoma. A diverting stoma was constructed routinely for all patients and was closed 3 months after surgery or 1 month after the last cycle of adjuvant chemotherapy.
Clinicopathological parameters and definitions
Morbidities were defined as complications within 30 days after surgery that required additional treatment or prolonged hospital stay. The residual tumor size was defined as the long axis diameter of tumors obtained from the specimen immediately after resection. The specimens were examined by at least two experienced pathologists using a standard method. When <9 lymph nodes were found, reexamination of the specimen was performed to guarantee a maximum lymph node yield. 21 Tumor regression levels were graded according to the Rectal Cancer Regression Grade (RCRG) method by Wheeler et al. 22 The three RCRGs were defined as follows: RCRG 1, sterilization or only microscopic foci of adenocarcinoma remaining, with marked fibrosis; RCRG 2, marked fibrosis but macroscopic disease present; RCRG 3, little or no fibrosis, with an abundant macroscopic disease.
Follow-up
A follow-up evaluation was performed every 3 months for the first 3 years, then every 6 months for the next 2 years, and annually thereafter. At each visit, a physical examination, carcinoembryonic antigen (CEA), carbohydrate antigen19-9 (CA19-9), chest X-ray or computed tomography scans, and abdominopelvic MRI were performed. A colonoscopy was performed annually after surgery. DFS was measured from the date of surgery to that of recurrence or death. Recurrence was diagnosed via radiological detection of lesions with increasing size or by histological confirmation.
Statistical analysis
Statistical analysis was performed using SPSS software version 21.0 (IBM, Inc., Armonk, NY). Survival rates were assessed and compared using the Kaplan–Meier method and log-rank tests. Backward stepwise Cox proportional hazard model was utilized for multivariable survival analysis. The cutoff values of residual tumor size calculated by X-tile 3.6.1 (copyright Yale University 2003–2005) for DFS were used in the multivariate analysis. 23 Statistical significance was defined as P < .05.
Results
Patients' characteristics
The characteristics of the 101 enrolled patients and their chemotherapy regimens during CRT are summarized in Table 1. Laparoscopic surgery was performed for 63 patients (62.4%). Twenty-six patients (25.7%) had a pathologic complete response, and 73.3% patients were ypN0.
Patients' Characteristics
BMI, body mass index; ASA, American Society of Anesthesiologists; AR, anorectal ring.
Perioperative results
The operative results are summarized in Table 2. The operation time in laparoscopic group was 33 minutes longer than open surgery, while the estimated blood loss was less in the laparoscopic group. The two groups had similar lymph node number harvested (12 ± 6 versus 11 ± 5, P = .698) and positive CRM rates (1.6% versus 5.2%, P = .555). Laparoscopic APISR had less postoperative pneumonia (3.2% versus 21.0%, P = .010), overall complications (15.9% versus 36.8%, P = .010), and shorter postoperative stay in hospital than open group. The mortality was nil in this study.
Short-Term Results of Abdominal Approach Partial Intersphincteric Resection After Chemoradiotherapy
Significant differences are indicated in bold.
Fisher exact test.
CRM, circumferential resection margin.
Mid-term outcomes
During the median follow-up of 39 months, four patients suffered a local recurrence and 18 developed distant metastases. The 3-year LRR, DFS, and OS were 2.5%, 80.2%, and 95.3% respectively. The 3-year DFS in stage 0, I, II, and III were 96.2%, 94.4%, 85.7%, and 44.7% (Log-rank = 29.791, P < .001), as were shown in Figure 2. There were no significant differences of DFS between the pathological stage 0 and I (log-rank = 0.016, P = .899), between the stage I and II (log-rank = 3.496, P = .062). Patients in stage III had worse DFS than stage II (log-rank = 6.339, P = .012), as were shown in Figure 1. Laparoscopic and open APISR produced similar 3-year LRR (1.7% versus 3.7%, P = .199) and DFS (82.2% versus 77.5%, P = .429).

Kaplan–Meier survival curve comparing DFS in different pathologic stages; The 3-year DFS in pathological stage 0, I, II, and III were 96.2%, 94.4%, 85.7%, and 44.7% respectively (Log-rank = 29.791, P < .001). There was no significant difference of 3-year DFS between stage 0 and I (Log-rank = 0.016, P = .899). Patients in stage II has a slightly worse DFS than stage I, but they did not reach statistical differences (Log-rank = 3.496, P = .062). The 3-year DFS in stage III were significantly worse than that in stage II (Log-rank = 6.339, P = .012). DFS, disease-free survival.
Univariate analysis
The best cutoff value of residual tumor size for DFS was 2.8 cm, which was calculated by X-tile. In univariate analysis using the Kaplan–Meier method and log-rank tests, stage ypT3, ypN1-2, RCRG more than 2, and residual tumor size more than 2.8 cm were risk factors associated with poor DFS. The other variables that were evaluated (sex, age, ASA score, distance from the anal verge, laparoscopic surgery, tumor differentiation, mucinous adenocarcinoma, pre-CRT and post-CRT CEA, and CA19-9) were not associated with prognosis of APISR after CRT, as were shown in Table 3.
Univariate Analyses of Risk Factors Associated with Disease-Free Survival of Abdominal Approach Partial Intersphincteric Resection After Chemoradiotherapy
Significant differences are indicated in bold.
ASA, the American Society of Anesthesiologists; AV, anal verge; BMI, body mass index; CA19-9, carbohydrate antigen19-9; CEA, carcinoembryonic antigen; CRT, chemoradiotherapy; DFS, disease-free survival; OXA, oxalipatin; RCRG, Rectal Cancer Regression Grade.
Multivariate Cox analysis
In multivariate analysis, stage ypN1-2 (hazard ratio = 8.256, 95% confidence interval: 2.742–24.855, P < .001) and residual tumor size more than 2.8 cm (Hazard ratio = 3.077, 95% Confidence interval: 1.036–9.137, P = 0.043) were the independent prognostic factors for poor DFS, as shown in Table 4.
Multivariate Cox Analysis for Prognostic Factors Associated with Disease-Free Survival After Abdominal Approach Partial Intersphincteric Resection
CI, confidence interval; RCRG, Rectal Cancer Regression Grade; SE, standard error.
Discussion
This study suggested that APISR for low rectal cancer downstaging from initial stage cT3 after CRT had the 3-year LRR of 2.5%, DFS of 80.2%. The DFS in pathologic stage 0–III were 96.2%, 94.4%, 85.7%, and 44.7% respectively, similar to the previous results of traditional ISR after chemoradiation that was estimated to be 96.2%, 84.8%, 72.9%, and 38.0% respectively. 24
Although completely abdominal approach ISR was performed by some experienced institutions,16–19 it remains controversial considering the higher risk of circumferential resection margin (CRM) involvement in the abdominal approach group. 25 However, positive CRM rates between the abdominal approach group and the perineal approach group were similar (9% versus 10%) in Kanso et al.'s study. 26 Our previous study of APISR also produced favorable mid-termed outcomes with a CRM rate of 1.1%–4.2%. 19 To date, it has been documented that no significant difference of long-term outcomes between the two groups as well. 27 In this study, the 3-year LRR for APISR after CRT was as low as 2.5% similar to the previous result of transanal TME. 15 In the previous report of transabdominal ISR with 33.6% of patients received CRT, the local recurrence occurred in 3.2%–6.1% patients within 3 years. 18 As we know, the crucial independent risk factor for LRR is the CRM. It is rather remarkable that no distal margin and only 3.0% of the CRM were involved in this cohort. The lower rate of positive CRM may reflect the strict selection of surgical indications, implementation of CRT, and meticulous operation. As was previously mentioned in ESMO guidelines in 2013, even for very low tumors (especially located anteriorly) in baseline clinical stage T2, CRT may be indicated since the distance to the mesorectal fascia is very small. 28 These radical strategies have been changed in the new edition of ESMO guidelines in 2017. 9 After CRT, the reassessment should be made according to high-resolution MRI. Patients with more advanced stage than ycT3 or suspected lateral lymph node metastases should receive more extensive surgery.
In this study, laparoscopic APISR had the similar 3-year LRR (1.7% versus 3.7%) and DFS (82.2% versus 77.9%) comparing with open surgery. It was consistent with our previous results. 18 Laparoscopy may provide wider vision in the deep pelvis and facilitate precise, sharp dissection, and the accomplishment of APISR. Although the operation time was longer, the morbidity including pneumonia was less in the laparoscopic group. Laparoscopic APISR had advantages in short-term results without compromising the midterm oncological outcomes. 15 The long-term outcomes need to be addressed in future.
This study suggested that for patients with stage ypT3 had slightly worse DFS than patients with ypT0-2 (75.8% versus 81.7%) in univariate analysis. However, there was no significant difference in the multivariate analysis. The staging for distal third rectal cancer is confusing for some surgeons. For tumors above the levator muscle, T3 represents the invasion only within mesorectum, while for tumors below the superior margin of anorectal ring T3 indicates the involvement of conjoint longitudinal muscle with a distance to external sphincter or levator muscle more than 1 mm.29,30 In the latter case, patients may possibly receive partial external sphincter resection or more extensive surgery as a result of over staging. In fact, all the cases in stage ypT3 in this study were the juxta-anal tumors above the anorectal ring that invading within the mesorectum after CRT. Our study suggested that even for ypT3 juxta-anal tumors, APISR was indicated and produced favorable midterm outcomes in the specialized center.
This study showed the residual tumor size more than 2.8 was the independent prognostic factors for APISR after CRT. As we know, tumor size represents the treatment response in modified Response Evaluation Criteria in Solid Tumors. 31 In addition, it is one of the staging indexes for various solid tumors such as breast cancer, hepatocellular carcinoma, and gastrointestinal stromal tumors but not for rectal cancer. In fact, whether pretreatment tumor size could be the significant prognostic factor for rectal cancer remains controversial. 32 It is reasonable to speculate that pretreatment tumor size does not always reflect the stage of rectal cancer and tumor loading of carcinomatous components with the similar degree of differentiation, such as a large polyp with early malignancy. CRT might sterilize rectal cancer and select the tumor cell colonies, leaving only relatively insensitive colonies. In fact, post-treatment tumor size after CRT was one of the most important indicators of tumor response to select the candidates of organ-sparing management in many clinical trials.33–35 It was also reported that post-CRT tumor size more than 3 cm was the independent risk factor of positive CRM and local recurrence. 36 Lee et al. confirmed that residual tumor more than 3.5 cm was associated with a poor prognosis for traditional ISR after CRT. 24 However, previous cutoff values of residual tumor size were determined empirically. In our study the cutoff point of residual tumor size calculated by the software of X-tile would be valuable for further evaluation.
Another strong prognostic predictor for APISR was regional lymph node involvement after CRT. Patients with stage ypN1–2 had significant worse 3-year DFS than stage ypN0 (44.7% versus 92.9%), in accordance with the 3-year DFS of traditional ISR (38% versus 82.9%) in Lee's report. 24 Lymph node response should be taken into account for the indications of ISR after CRT. Residual lymph node metastases may indicate the insensitive cohort after chemoradiation and the progress of the disease. In the condition of improved local control with the benefit of CRT, distant metastases have become a challenge for low rectal cancer to date. 37 A recent study has suggested that intensive chemotherapy could improve the response of CRT. 38 Future researches should be focused on more intensive neoadjuvant treatments to increase the organ-preservation candidates and improve the prognoses. 39
For cT3 low rectal cancer within 1 cm above the anorectal ring, APISR is feasible after downstaging with the negative mesorectal fascia by CRT. In the procedure, the surgical plane extending from the holy plane could be easily identified from the abdominal side especially in the wide vision of laparoscopic surgery. The dissection plane is kept continuous and intact by a completely abdominal approach without interruption. The APISR avoids excessive traction on anal sphincter to maintain good continence. Besides, it reduces the difficulties and is time-saving to construct a stapled anastomosis, which might reduce the incidences of anastomotic leakage and stricture as well. 40 However, if the distal mobilization was not sufficient, it would be better to turn to perineal approach and perform a hand sewn anastomosis. Although laparoscopic APISR remains technically demanding due to the dissection in the deep narrow pelvis with rigid instruments, it could be performed by a well-coordinated specialized team with careful patient selection. Maybe with the help of the robotic system, the learning curve will be shorter.
This study was limited by its retrospective nature, the small sample with the midterm follow-up in a single center, missing pathological lymph node regression scoring, clinical substaging T3, and the information of extramural vascular invasion according to the high-resolution MRI. Other limitations included lack of comparison with traditional ISR or transanal TME. In addition, due to overstaging some patients who were appropriated for organ-sparing management had received APISR. Nevertheless, to our knowledge, this was one of the very few studies evaluating the feasibility and potential prognostic factors of APISR for cT3 low rectal cancer after downstaging by CRT.
In conclusions, laparoscopic and open APISR for cT3 juxta-anal rectal cancer after downstaging by CRT produced satisfactory mid-term oncological outcomes particularly for those with stage ypN0 and the residual tumor size <2.8 cm. In contrast, regional lymph node involvement and residual tumor larger than 2.8 cm after CRT were poor prognostic factors that should be estimated for surgery in future.
Footnotes
Acknowledgments
This study was supported by the National Clinical Key Specialty Construction Project (General Surgery) of China (No. 2012-649), Fujian Minimally Invasive Medical Center Construction Project (No. 2017-171), Ethicon Exellence in Surgery Grant of Wu Jieping Medical Foundation (No.320.2710.1845), and Health care Joint fund of Fujian Provincial Natural Science Foundation Projects (No. 2018J01183). The authors thank all the staff in the Department of Colorectal Surgery and Department of Radiotherapy at Fujian Medical University Union Hospital.
Disclosure Statement
No competing financial interests exist.