
Abstract
Abstract
In an email to the Editor-in-Chief dated June 3, 2019, the authors of the article entitled, “Endoscopic Treatment of Endoscopic Retrograde Cholangiopancreatography,” published in the March 2019 issue (v29, n3) of Journal of Laparoendoscopic and Advanced Surgical Techniques, have requested the withdrawal of the article since, according to the email, their “…endoscopy information system had been updated twice, [and] some of the original data had been omitted, which might lead to errors in statistical results.”
The Editor-in-Chief of the Journal, P. Marco Fisichella, MD, MBA, FACS, determined the request for withdrawal was valid, and therefore is officially retracting the article from the published literature.
Journal of Laparoendoscopic and Advanced Surgical Techniques
is committed to upholding the highest standards of peer review and scientific publishing.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP)-related duodenal perforation resulting from ERCP procedures is an uncommon but serious complication accompanied by severe morbidity and significant risk of mortality. In previous studies from other medical centers worldwide, overall mortality rate and operative mortality rates ranged from 4.2%–34.4% to 13.3%–60%, respectively.1–7 In a study by Jin et al., the surgical mortality rate (16.7%) was higher than the mortality following conservative nonsurgical treatment (4.9%). 4 With continuous improvement in the understanding of physiology and treatment methods for duodenal perforations, outcomes have improved significantly.8–10
Timely and correct diagnosis accompanying the appropriate treatment can minimize adverse effects and improve treatment outcomes.1,11,12 Although type I perforation can be successfully managed by surgery,2,3,13,14 the associated trauma and longer hospital stay often cause significant distress among these patients. Surgical treatment of type II perforation still has a high mortality (in ∼50% of cases). 3 Surgery is also controversial for type II duodenal perforations because the perforation site often cannot be found in these patients.2,3,13,14
Some studies have reported successful endoscopic treatment in cases of ERCP or endoscopic ultrasound-related duodenal perforation.1,15,16 When endoscopic treatment is correct and appropriate, the hospital stay can be shortened and thus any iatrogenic adverse effects are reduced. With the increasing success of endoscopic treatment for duodenal perforation,11,15–20 endoscopic management has been recommended for ERCP-related duodenal perforation in selected patients.11,21
In this study, we analyzed our experience in endoscopically managing duodenal perforations caused by ERCP to determine optimal management.
Materials and Methods
This study was conducted at three large hospitals in China: Ningbo No. 2 Hospital, the First People's Hospital of Yuhang District, and No.1 People's Hospital of Hangzhou. Clinical information was approved by the Medical Ethics Committee of the above hospitals, and medical records of all patients with ERCP-related perforation were retrospectively reviewed. Age, gender, indication for ERCP, ERCP procedure, clinical presentation, laboratory findings, diagnosis methods, type of perforation, final management strategy, and length of hospital stay were analyzed.
In the three endoscopy units, almost all ERCP procedures were performed for therapeutic reasons. According to radiological imaging results, including computed tomography (CT), magnetic resonance cholangiopancreatography, combined clinical symptoms, and laboratory results, ERCP indications were established. Endoscopic sphincterotomy was performed in 16,645 patients (85.5%), 2823 patients (14.5%) underwent a precut papillotomy; and 3578 (18.4%) cases were performed with balloon dilatation after endoscopic sphincterotomy. Standard sphincterotomy and balloon dilatation were performed by an experienced endoscopist with extensive experience in therapeutic ERCP. Precutting techniques were used only in cases with unsuccessful cannulation.
After ERCP, the operator or assistant conducted clinical follow-up of the patients. Routine laboratory tests—including routine blood test, serum amylase, and C-reactive protein (CRP)—were performed the first day following ERCP. If white blood cell counts and CRP levels increased significantly after ERCP, or if patients had abdominal pain or fever that could not be explained by a primary disease or pancreatitis, then abdominal CT scans were performed.
ERCP-related duodenal perforation has been divided into four types according to Stapfer's classification system, 20 which consists of the following types: (1) lateral duodenal wall perforation results from the scope itself; (2) perivaterian injury related to sphincterotomy; (3) bile or pancreatic duct injury related to wire/basket instrumentation; and (4) retroperitoneal air alone.7,20,22
Once type I perforation was diagnosed, endoscopic closure was performed immediately using multiple hemoclips (Micro-Tech, Nanjing Co., Ltd., Nanjing, Jiangsu, China or Olympus Corp., Tokyo, Japan). If endoscopic closure was not possible, surgical intervention was considered. If type II perforation was diagnosed during ERCP, the fully covered SEMS (Micro-Tech, Nanjing Co., Ltd.) was implanted after completing the corresponding treatment. If type II perforation was diagnosed after ERCP and extensive retroperitoneal fluid collection occurred within 48 hours, then nasobiliary drainage tube would be replaced as a fully covered SEMS.
For patients with biliary perforation of type III who had been implanted with the nasobiliary drainage tube, no special treatment was needed. For patients with pancreatic duct perforation of type III, surgical intervention was considered. For type IV perforation, no special treatment was needed.
In addition to type IV perforations, other types of perforations were treated simultaneously with gastrointestinal decompression, fasting, and use of broad-spectrum antibiotics on the basis of the endoscopic treatment. Immediate emergency surgery is often required if signs and symptoms of peritonitis develop within the first 72 hours.
Results
Between March 2005 and March 2017, 19,468 ERCPs were performed in the three hospitals. A total of 58 ERCP-related perforations (0.29%) were identified in this study; 36 were female and 22 patients were male, with a mean age of 68.5 years (range 37–87 years). In total, there were 8 type I perforations, 44 type II perforations, 4 type III perforations, and 2 type IV perforations. Patient demographics are shown in Table 1.
Patient Demographics
The same patient.
CRP, C-reactive protein; ES, endoscopic sphincterotomy; CT, computed tomography.
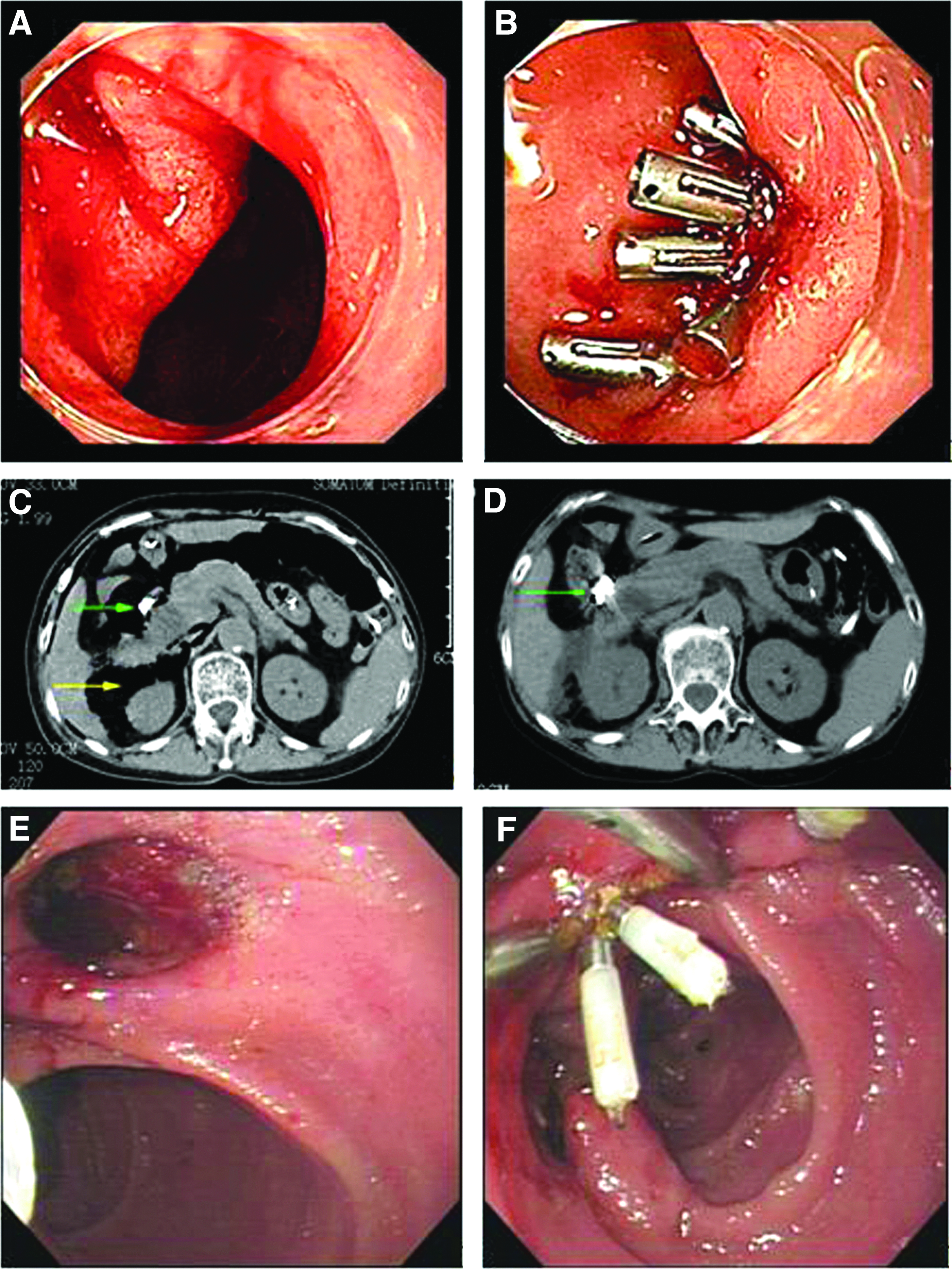
Eight cases with type I perforation were diagnosed by endoscopic direct visualization of the retroperitoneal space (Fig. 1A) or fluoroscopy revealing retroperitoneal free air during ERCP (Fig. 1B). Five cases with type II perforation and 3 with type III were diagnosed by endoscopy and X-ray during ERCP (Fig. 1C, D). The other cases were diagnosed by CT (Fig. 1E, F).

Intraoperative and postoperative photographs of type I and type II perforations during ERCP;
Of 8 cases with type I perforation, 2 cases were located in the duodenal bulb, 3 in the proximal duodenal flexure, 2 in the duodenal descending segment, and 1 in the duodenal horizontal segment. Seven cases with type I perforation were managed successfully using multiple endoclips (Fig. 2A, B, E, F). On the 10th day after endoscopic closure, CT showed that the retroperitoneal free air significantly decreased compared with 10 days earlier (Fig. 2C, D). Another type I perforation was located in the horizontal segment of duodenum; endoscopy could not show its exact location so surgery was performed. All patients made uneventful recoveries after management.
Two patients experienced duodenal perforation, which was immediately recognized and treated with hemoclips.
Of 44 cases with type II perforation, 11 cases were managed successfully using fully covered SEMS (Fig. 3A–C), in the remaining cases, patients received no special treatment after nasobiliary drainage, in which 13 cases had retroperitoneal abscess formation successfully treated by CT-guided percutaneous external drainage, but 1 patient died due to sepsis.

Intraoperative and postoperative photographs of type II and type III perforations.
In 1 patient with type III perforation, the pancreatic duct was cannulated repeatedly by the wire and catheter, but bile duct cannulation was not completed. The patient presented severe upper abdominal pain 8 hours after ERCP, and the operation confirmed that pancreatic parenchyma had been pierced by the wire and catheter (Fig. 3D). The patient had intermittent fever for 39 days after retroperitoneal drainage, which had more pancreatic juice with a high concentration of amylase. ERCP was performed again and a pancreatic duct stent was placed and the retroperitoneal drainage tube was pulled out on the 46th day. The other cases with type III did not receive any special treatment after nasobiliary drainage. All patients were discharged uneventfully.
Overall, mean hospital stay was 19.6 days (range: 13–67 days). The mean hospital stay of 7 cases with type I treated by endoscopy (16.5 ± 2.1 days) was lower compared to 1 case treated by surgery (21 days) (P = .045). The mean hospital stay of 11 cases with type II perforation treated actively by endoscopy (26.5 ± 3.3 days) was lower compared to 33 cases receiving passive conservative treatment (34.6 ± 3.9 days) (P = .021). There was no significant difference in mortality (P = 1.000) between patients with type II perforation treated by endoscopy (n = 11, no deaths) and patients of passive conservative treatment (n = 33, 1 death).
Discussion
Over 10 years, there have been many reports about ERCP-related duodenal perforation.1,2,4,7,8,17,23–26 However, there is no uniform standard for the treatment of ERCP-related duodenal perforation. Some literature reported that certain patients with duodenal perforations could be treated with conservative medical therapy giving good results,17,25,27 while other authors have proposed that post-ERCP perforation requires surgical treatment.3,8,13,14,23,28,29
In recent years, many scholars advocated that the choice of treatment should be based on the type of perforation.1,11 It is generally accepted that type I perforation requires prompt surgical interventions.3,9 However, recent studies recommended endoscopic treatment by clipping, endoloop, and over-the-scope clip for type I perforations.20,30–32
In the present study, 7 of 8 patients with type I perforation were successfully managed by endoscopic closure using hemoclips and discharged uneventfully, while another patient was discharged 3 weeks after surgery. The 8 patients were treated differently as 7 cases of perforations were located in the proximal duodenal (duodenal bulb, proximal duodenal flexure, and duodenal descending segment), where the endoscope could easily reach and had ideal vision and thus the perforations were treated using endoscopic closure devices, while another perforation was located in horizontal segment of duodenum, where the endoscope was too short for ideal vision to be treated by endoscopy.
In the present study, endoscopic treatment has certain advantages for proximal duodenal perforation. The mean hospital stay of 7 cases with type I perforation treated by endoscopy was lower compared to 1 case by surgery. For cases of type II and III, perforations may be managed conservatively on the basis of endoscopic biliary drainage or pancreatic duct drainage. More clinical practice supports the above views.5,29,33–36 Similar results were also found in this study.
Of 44 cases with type II perforation, 33 underwent endoscopic nose-biliary drainage, and 11 underwent covered metallic stent drainage, and 43 had successful outcome with conservative management except for 1 death. However, the mean hospital stay of active endoscopic treatment (metallic stents) is significantly lower than those receiving passive conservative treatment (i.e., only nasobiliary drainage). We speculated that fully covered SEMS not only plays a role in biliary drainage but also plays a role in sealing the perforation. As fully covered SEMS can occlude the perforation site by radial force, and the perforation site can heal quickly, nose-biliary duct may not prevent bile flow into the perforation site completely. 37
In the case of type III perforation in this study, the pancreatic parenchyma was pierced by the guidewire and catheter, and surgical drainage was performed first, but the result was not ideal. Thirty-nine days after the operation, the retroperitoneal drainage tube still had pancreatic juice with a high concentration of amylase. However, the patient was discharged uneventfully 7 days after the endoscopic pancreatic duct stent implantation. This result suggested that the endoscopic pancreatic juice drainage should be performed before surgical drainage. A reasonable explanation is that the pancreatic duct stent is able to seal the pancreatic duct perforation to a certain extent. Therefore, while endoscopy can show the precise location of type I perforation, or type II perforation can be found in time, endoscopic intervention is the preferred treatment.
The patients with type IV perforation in this study only underwent endoscopic nose-biliary drainage and were discharged uneventfully.
The main limitation of this study is that our conclusion is empirical because of the low number of cases. Thus the scientific value of endoscopic treatment in ERCP-related duodenal perforation still needs to be confirmed by further clinical practice and a bigger series.
In conclusion, ERCP-related duodenal perforations include different categories. Many (especially type I and II) ERCP-related duodenal perforations can be successfully treated with endoscopic management. Active endoscopic therapy may be better than passive conservative treatment for treating type II perforation.
Footnotes
Authors' Contributions
D.S. made substantial contributions to the conception of the study and clinical work; J.f.Y. and Y.p.L. contributed to the study design, acquisition and analysis of data, and article revision.
Disclosure Statement
All authors declare no conflict of interest relevant to this article.