
Abstract
Abstract
Background:
Sliding indirect inguinal hernias containing ovary are not uncommon in girls. We reported our experience with laparoscopic treatment of inguinal ovarian hernias in female infants and children with the aim to standardize the surgical technique.
Methods:
The medical records of all girls who underwent laparoscopic inguinal hernia repair in our unit over the past 5 years were retrospectively reviewed. Only patients with an ovary found intraoperatively in the hernia sac were included in the study. All patients younger than 1 year received preoperatively a bowel preparation with simethicone and enemas.
Results:
A total of 289 girls (median age 3.2 ± 0.5 years) underwent laparoscopic inguinal hernia repair during the study period. Thirty-seven patients (12.8%) had an ovarian hernia and were included in the study. Of these 37 girls, 9 (28.1%) were younger than 1 month, 20 (62.5%) ranged in age from 2 months to 1 year, and 3 (9.4%) were from 1 to 7 years. The average operative time was 23.7 minutes (range 18–43 minutes). No necrotic ovary was found intraoperatively, and all the procedures were accomplished laparoscopically. Neither intraoperative nor postoperative complications were reported. A patency of the contralateral canal of Nuck was found in 16 of the 37 patients (43.2%) and repaired during the same procedure. The average length of hospitalization was 21.8 hours (range 18–36 hours). No hernia recurrence or ovarian atrophy was recorded at a mean follow-up of 36 months (range 1–60 months).
Conclusions:
On the basis of our experience, laparoscopy should be considered the gold standard for the treatment of inguinal ovarian hernias in girls. Key points for standardization of the technique are as follows: bowel preparation in children younger than 1 year, use of 5-mm umbilical balloon trocar, correct positioning of 3-mm working screw trocars, section of the abnormal attachment of ovarian suspensory ligament, section of the periorificial peritoneum, and use of nonresorbable sutures.
Introduction
The incidence of inguinal hernia in pediatric patients varies between 0.8% and 4% and increases to about 30% in preterm infants 1 More than 96% of pediatric inguinal hernias are indirect, originating from a patent processus vaginalis. 2 The incidence of inguinal hernia is higher in male infants than in female infants, with documented ratios ranging between 3:1 and 10:1. 3 The incidence of incarceration in untreated hernias ranges between 6% and 18% in children, but it increases to ∼30% in infants.1,4
Inguinal hernias containing ovary and fallopian tube are not uncommon in female infants.5,6 A prolapsed ovary is almost exclusively the cause of an irreducible hernia in girls.7–9 The ovaries trapped within the inguinal hernia sac have a higher risk of complications than those in the normal pelvic position. 3 In these cases, ovarian torsions have been described in 2%–33% of cases, justifying an early surgical repair in irreducible hernias, even in asymptomatic patients.3,5,10
Open inguinal herniorrhaphy is a well-established technique for inguinal hernia repair, but it is sometimes not easy to perform in case of ovarian incarceration. 5 The advent of minimal access techniques has revolutionized the traditional management of pediatric pathologies, including inguinal hernia. The laparoscopic technique has been recently standardized 2 , and the key points of the procedure include the section of the periorificial peritoneum using monopolar coagulation and the closure of the defect by a purse-string or an N-shaped suture using a nonresorbable stitch. The proposed advantages of the laparoscopic technique over conventional open repair are visualization of contralateral patency, identification of rare hernias, reduced postoperative pain, improved cosmetic results, a faster return to full daily activities, and lower complications rate, especially in infants and in complicated cases.1,2 In our daily practice, we noted that the laparoscopic repair of inguinal ovarian hernias in girls required some technical modifications compared with the technique routinely adopted for common inguinal hernias. For this reason, we reported our experience with laparoscopic treatment of inguinal ovarian hernias in female infants and children with the aim to standardize the surgical technique for this pediatric pathology.
Materials and Methods
The medical records of all female patients who underwent laparoscopic inguinal hernia repair in our unit over the past 5 years were retrospectively reviewed. Only girls with an ovary found intraoperatively in the hernia sac were included in the study.
All patients younger than 1 year, candidate for elective laparoscopic repair, received preoperatively our standardized bowel preparation protocol. This protocol includes simethicone (10 drops 3 times/day after the meal) for at least 2–4 days before surgery; enemas with probe for 2 days before surgery; fasting at least 5 hours before surgery. All these measures were easily performed by parents at home, without increasing the length of hospital stay. The bowel preparation allowed to deflate the intestinal loops from gas and stools; in this way, a larger working space was obtained and the entire laparoscopic procedure was performed keeping a low intra-abdominal pressure (IAP).
This study received the appropriate institute review board approval.
Surgical technique
All the procedures were performed under general anesthesia with orotracheal intubation, the bladder was emptied with a Nelaton catheter before surgery, and the table was positioned in a 15° Trendelenburg position.
Three trocars were positioned in all cases: one 5-mm umbilical balloon trocar for the 0° 5-mm optic and two 3-mm working screw trocars in triangulation with the optic port (Figs. 1 and 2). In infants younger than 1 year, especially in newborns, the working ports were placed on the same line with the optic port, to obtain a larger working space and avoid the clashing between the optic and the instruments. In cases with a very limited intra-abdominal working space due to bowel distention, the working ports were safely introduced within the cannula of the umbilical port (“trocar in trocar”) (Fig. 3). The IAP varied between 7 and 8 mmHg.
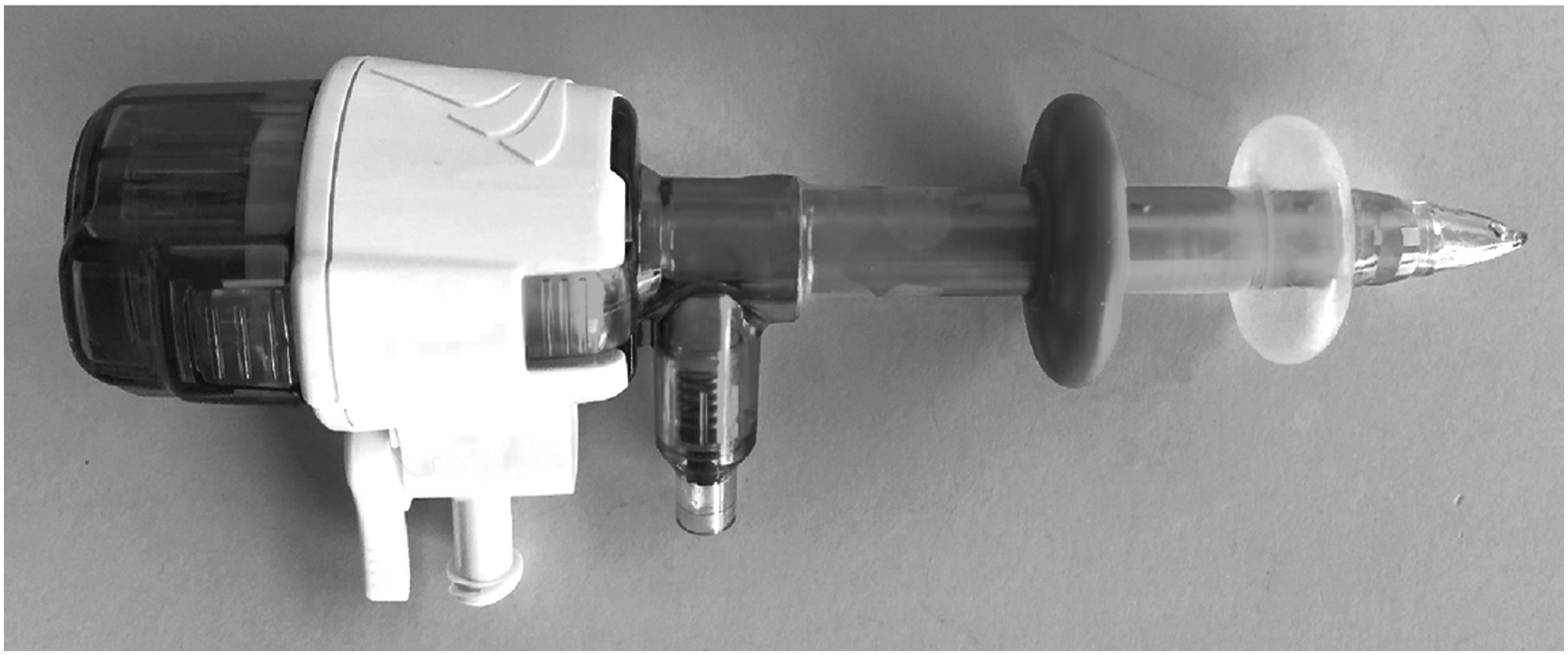
The 5-mm balloon trocar used for the 5-mm 0° optic.

The 3-mm screw working trocar used for laparoscopic instruments.
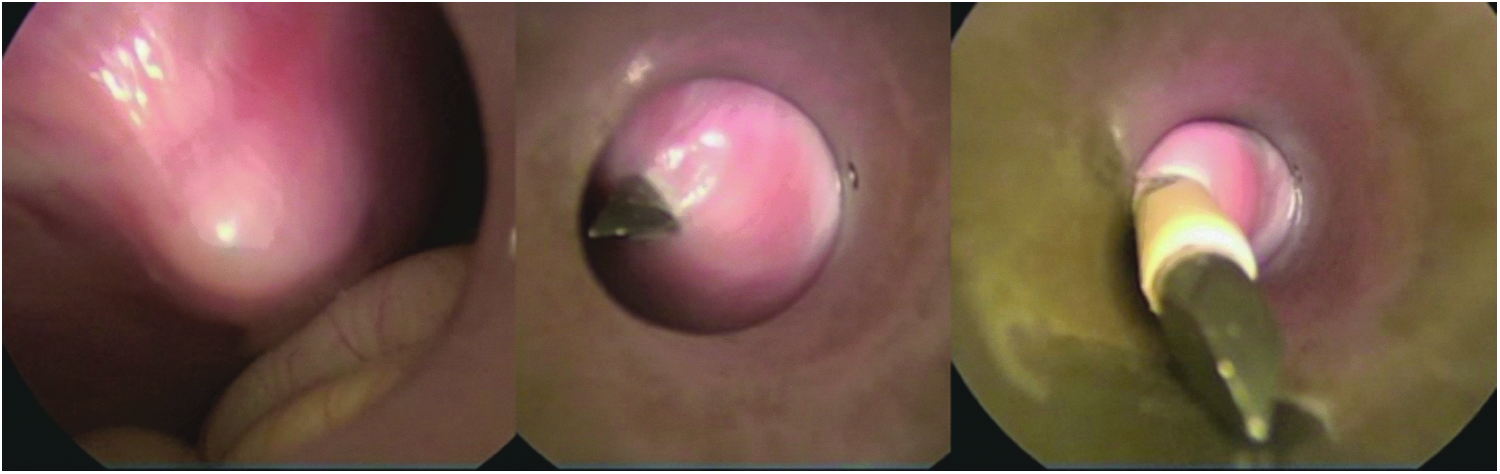
In cases with a very limited working space, the working ports can be safely introduced into the abdomen within the cannula of the umbilical trocar (“trocar in trocar”).
In regard to operative technique, after reduction of the hernia content with both extracorporeal manipulation and intracorporeal maneuver using atraumatic graspers, ovary and fallopian tube were visually inspected for any vascular damage. The abnormal attachment of the ovarian suspensory ligament over the internal inguinal ring, found in all patients of our series, was divided with monopolar hook and the herniated adnexa recovered the normal pelvic position. The periorificial peritoneum was sectioned with the monopolar hook.
A 3/8 of circle needle with a length of 20 mm was introduced transabdominally. The hernia orifice was closed with either a purse-string suture according to Montupet's technique or an N-shaped suture according to Schier's technique, 11 using a 2/0 nonresorbable stitch. The entire procedure was performed using a single suture. The optimal length of suture was about 15 cm for unilateral repairs and about 20 cm for bilateral pathology. The patency of contralateral canal of Nuck was always checked, and if present, it was repaired during the same procedure (Fig. 4).
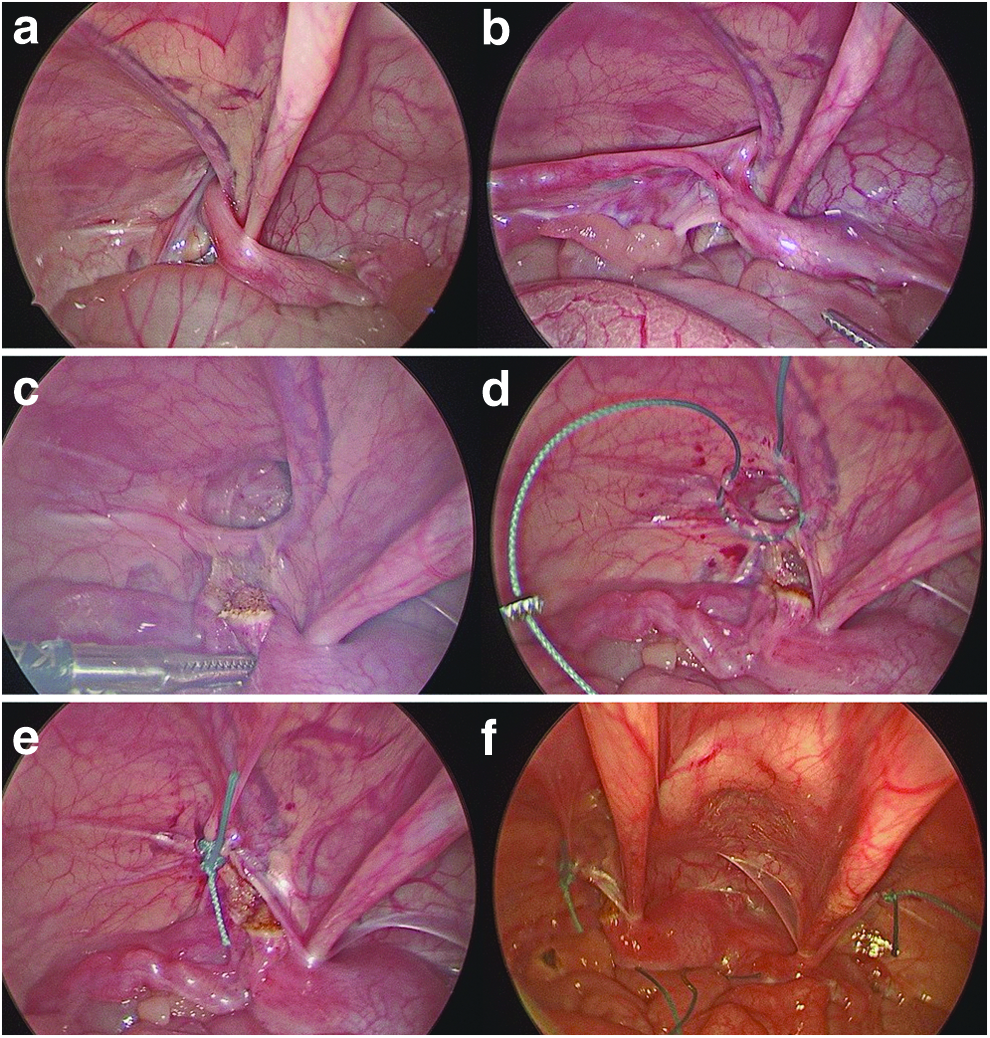
Surgical steps:
Results
A total of 289 girls, with a median age of 3.2 ± 0.5 years, underwent laparoscopic inguinal hernia repair in our unit over the past 5 years. An ovary was found intraoperatively in the hernia sac in 37 of the 289 girls (12.8%), who were included in the study, whereas the patients with adnexa in normal position were excluded. Of the girls with ovarian hernias, 9 (28.1%) were younger than 1 month, 20 (62.5%) ranged in age from 2 months to 1 year, and 3 (9.4%) were from 1 to 7 years. Sixteen of the 37 patients (43.2%) presented an asymptomatic irreducible inguinal mass and were promptly operated on within 1–4 days after diagnosis.
Three different surgeons (two senior surgeons and one trainee) performed the surgical procedures. All the procedures were successfully accomplished in laparoscopy with no need for conversions to open surgery. The average operative time was 23.7 minutes (range 18–43 minutes). All the ovaries were still prolapsed within the hernia sac wall at the time of surgery. No case of ovarian torsion was recorded in our series. After reduction in the abdominal cavity, all ovaries were visually inspected for any vascular damage and all were found in a good morphological condition with no necrotic or gangrenous aspect.
Neither intraoperative nor postoperative complications were reported. The patency of the contralateral canal of Nuck was found in 16 of the 37 patients (43.2%) and repaired during the same procedure. All the patients restarted oral feeding at a mean of 2–3 hours after the surgery, and they did not require any analgesic drug in the postoperative period except four patients (10.8%) who received a single oral administration of paracetamol (7.5 mg/kg) 8–12 hours postoperatively. The average length of hospital stay was 21.8 hours (range 18–36 hours). Only patients younger than 1 year had an overnight hospitalization following the surgery since our anesthesiologists required their observation for at least 12–24 hours postoperatively, especially if premature infants with a history of respiratory distress or bronchodysplasia. The remaining cases were performed on an outpatient basis.
No hernia recurrence or ovarian atrophy was recorded at a mean follow-up of 36 months (range 1–60 months). The parents of all operated patients were highly satisfied with the cosmetic results (Fig. 5). All patients underwent an abdominal ultrasonography 1 year postoperatively to check the ovarian status, and the prolapsed ovary appeared morphologically normal and with a good vascular supply in all operated patients.

Cosmetic results 6 months after laparoscopic repair.
Discussion
The diffusion of minimally invasive surgery (MIS) has revolutionized the traditional management of some pediatric pathologies including inguinal hernia.1,2,11 Analyzing the recent international literature, there is still an ongoing debate about the best management of inguinal hernia in children. 12 In female patients, it is not uncommon to find a prolapsed ovary within the hernia sac, which may undergo incarceration.3,5,6 The incidence of incarceration of a prolapsed ovary within the sac of an inguinal hernia is unclear, and it ranged between 6% and 15% of inguinal hernias in girls, as recently reported.3,5,13–15 The management of an inguinal ovarian hernia depends on its reducibility and the presence of clinical signs of strangulation or torsion. 3 The existence of a critical time interval between ovarian incarceration in an inguinal hernia and subsequent torsion is unknown; obviously, incarcerated ovaries have a higher risk of torsion and infarction compared with ovaries in the normal pelvic position.9,15 The torsion of the suspended ovary occurs primarily, with a frequency ranging between 2% and 33% in different series.3,13 For these reasons, even without clear signs of strangulation, the presence of a twisted ovary should be always suspected in any irreducible hernia in a female patient. 5 A prompt repair is advisable within 24–48 hours in any patients with an ovary in the hernia sac to prevent ovarian torsion and subsequent gonadal necrosis. 14
The traditional repair via inguinal approach is not easy to perform in female infants with an incarcerated ovarian hernia, also in expert hands.16,17 The high ligation of the hernia sac through conventional transinguinal approach is also technically challenging for sliding inguinal hernias in girls because of sliding of the fallopian tube and the ovarian ligament. 5
After a 25-year experience, we recently standardized the laparoscopic technique of inguinal hernia repair 2 and the key points of the procedure include the section of the periorificial peritoneum using monopolar coagulation and the closure of the defect by a purse-string or an N-shaped suture using a nonresorbable stitch. In our daily practice, we noted that the laparoscopic repair of inguinal ovarian hernias in girls required some technical modifications compared with the technique routinely adopted for common inguinal hernias.
First of all, we believe that it is very useful to perform a preoperative bowel preparation with simethicone (10 drops 3 times/day after the meal) and enemas in all patients younger than 1 year who undergo laparoscopic repair in elective conditions. 18 In such patients, the preoperative bowel preparation according to our standardized protocol represented an important additional benefit as it increased the working space by reducing bowel content and allowed to perform the entire procedure, keeping the IAP under 8 mmHg.
As for the technical point of view, it is very useful to adopt a 5-mm balloon trocar to be placed in the umbilicus for the 0° 5-mm optic; this type of trocar can be lift up with no risk of dislodgement, thanks to the intra-abdominal balloon, so as to obtain a large and panoramic view of the pelvic region and keep a low IAP (Fig. 1). In regard to trocars' position, two main rules should be considered in small infants: the first is the use of 3-mm screw trocars so as to avoid their dislodgement during the change of instruments (Fig. 2) and the second is the positioning of the working trocars on the same line with the camera port to obtain a larger working space and avoid the clashing between the optic and the instruments. 16 Regarding the surgical technique, before closing the hernia defect, it is mandatory to section the abnormal attachment of the ovarian suspensory ligament to release the herniated adnexa. Recently, laparoscopic observation showed that the attachment of the ovarian suspensory ligament to the abdominal wall is dislocated ventrally in many cases of inguinal hernia in girls younger than 2 years. 19 For these reasons, the ovary remains near the pelvic rim and the deep inguinal ring in newborns, with higher chances of prolapse within the hernia sac. 10 Other technical recommendations are: to always section the periorificial peritoneum to release the distal part of the canal of Nuck and avoid tension during the defect's closure and to use nonresorbable sutures. In regard to the type of suture to be adopted for defect's closure, the purse string suture, the N-, or double N-shaped closure seem to give similar results in expert hands.20–22
The main advantages of laparoscopy over open technique in treating incarcerated ovarian hernias are: the easier reduction of the adnexa under visual control bypassing edematous structures and the possibility to inspect the reduced adnexa for viability. Another great advantage of the laparoscopic approach is the chance to check and eventually treat a patency of the contralateral canal of Nuck, which was found in >40% of patients in our series.
The main criticism moved to laparoscopic inguinal hernia repair, especially in premature infants, is the need for general anesthesia with orotracheal intubation and myorelaxation.23–25 However, we believe that this is not a true problem because, as we have already reported in a recent article, laparoscopic repair resulted faster than open inguinal repair, especially for bilateral pathology; the length of hospitalization of infants who underwent laparoscopic repair was exactly the same as open repair, but the laparoscopic repair reported a lower postoperative complications rate compared with open surgery, especially in infants. 12 For this reason, we believe that a strict collaboration with anesthesiologists' team is extremely important.
In conclusion, on the basis of our experience, we believe that laparoscopy should be considered the gold standard for the treatment of inguinal ovarian hernias in girls. The laparoscopic approach allows to perform an easy and safe reduction of the herniated adnexa, to visually inspect them for any vascular damage and finally to check the contralateral canal of Nuck for patency and to repair it during the same procedure. In the present study, we reported the fundamental rules to standardize the surgical technique; in this way, every surgeon can reproduce the different steps of the procedure to avoid complications and reduce recurrence rates.
Footnotes
Disclosure Statement
No competing financial interests exist.