
Abstract
Abstract
Background:
Bariatric surgery is superior to medical treatment for type 2 diabetes mellitus (T2DM) control in obese patients. Reports in the literature have been mainly based on Roux-en-Y gastric bypass (RYGB) or adjustable gastric band. The aim of this study was to analyze mid- and long-term metabolic results after laparoscopic sleeve gastrectomy (LSG).
Methods:
Obese patients with T2DM undergoing LSG were included in this study. Selection criteria for T2DM remission were: post-operatory fasting glucose (FG) level <100 mg/dL, and hemoglobin A1c (HbA1c) <6% without medication.
Results:
Between January 2009 and July 2016, 166 T2DM obese patients underwent LSG and completed ≥1 year follow-up. There were 101 women (60.8%; mean age 49.07 ± 12.8 years). Initial body mass index (BMI) was 46.44 ± 7.68 kg/m2. Mean time since T2DM diagnosis was 5.95 years (1–28). Preoperative HbA1c was 7.53% ± 0.97%. Before LSG, 75.3% (n = 125) were receiving oral hypoglycemic agents, and 13.25% (n = 22) insulin. Mean follow-up was 65 ± 10 months. Complete T2DM remission was achieved in 78.3%, 76.2%, and 71.4% at 1, 3, and ≥5 years respectively; in the long term, 7.2% attained partial remission, 10% improved, and 11.4% experienced recurrence of the disease. Remission rate was significantly lower in patients under insulin therapy preoperatively, and in patients with T2DM diagnosed ≥5 years before consultation (P = .0004 and .0001, respectively).
Conclusions:
At mid- and long-term follow-up, T2DM control was satisfactory after LSG. Preoperative insulin therapy and T2DM duration ≥5 years were predictors of less favorable outcomes.
Introduction
O
Health care costs devoted to the treatment of this disease have exponentially increased during the last decade. 3 Pharmacological treatment associated with lifestyle modification only changes discreetly glycemic control, but it does not achieve long-term treatment goals.4–7
Since the last publications from Pories, bariatric surgery has been gaining field in the treatment of this disease. 8 So far, the majority of publications addressing this issue reported encouraging results after Roux-en-Y gastric bypass (RYGB).9–15
Laparoscopic sleeve gastrectomy (LSG) is a relatively novel surgery that has shown up now to good results in terms of weight loss and resolution/improvement of comorbidities with low postoperative complication rate.16,17 Specifically, short- and mid-term results in regard to T2DM are promising, and they can be compared with those coming from other current techniques.17–21
The goal of this study was to analyze the effect of LSG at 1, 3, and 5 years on obese patients with T2DM.
Materials and Methods
Obese patients with T2DM undergoing LSG at our institution were included in this study. Data were analyzed retrospectively from a prospectively collected database. Statistical analysis was performed using the SPSS 19.0 Statistics 2011 program.
The following parameters were evaluated: demographics, pre- and postoperative body mass index (BMI), percentage excess weight loss (%EWL), time since T2DM diagnosis, type of treatment received before surgery, outcomes after surgery (complete remission, partial remission, improvement, no change, and eventual recurrence of the disease), pre- and postoperative glycemia, and HbA1C.
For complete remission, the ASMBS, SOARD, and outcome reporting standards criteria were used. 22
Fasting glucose (FG) <100 mg/dL
HbA1c <6%
No pharmacologic treatment
Partial remission was considered when values of HbA1c were between 6% and 6.4% and FG between 100 and 125 mg/dL for at least 1 year, in the absence of pharmacologic treatment. 22
Improvement was defined as HbA1c and FG significantly reduced, although remission criteria were not reached or when medication requirements were reduced (discontinuation of insulin therapy or oral hypoglycemic drugs [OHD] or reduction to half dosage). 22
Recurrence was defined as HBA1c or glycemia within T2DM range (HbA1c ≥ 6.5% and FG ≥126 mg%) or need for medications after having reached complete or partial remission at any point after surgery. 22
Long-standing T2DM was considered when diagnosis had been done at least 5 years before consultation. 22
To homogenize follow-up length, short-term was defined as 1 year, mid-term as 3 years, and long term as ≥5 years.
Surgical technique
A 12-mm optical trocar was inserted (EXCEL® Endopath, Ethicon Endosurgery, Cincinnati, OH) for the camera in the midline supraumbilical position under direct vision. Then, two 5-mm trocars were inserted, one on the left upper quadrant, and the other one on the right upper quadrant; a 10-mm trocar was introduced on the left flank. The Nathanson liver retractor was placed in the epigastrium. The short gastric vessels were all divided using the harmonic scalpel (Harmonic Ace®, Ethicon Endosurgery). Dissection of the greater curvature of the stomach continued toward the left pillar of the crus. The gastric sleeve was calibrated with a 42 Fr bougie. Then, using between four and five linear staplers (Echelon 60, Ethicon Endosurgery) the stomach was divided vertically starting on the greater curvature about 4–6 cm above the pylorus parallel to the lesser curvature and from this position toward the angle of His. Black (4.2 mm), green (4.1 mm), gold (3.8 mm), or blue (3.5 mm) cartridges were chosen depending on the thickness of the stomach wall. Staple line was reinforced with running stitches of absorbable suture. The specimen was retrieved in a plastic bag. A multi-lumen drain was left along the staple line.
Results
Demographics and perioperative data
Between January 2009 and July 2016, 166 obese patients with T2DM underwent LSG at our institution. There were 101 women (61%; mean age 49 ± 12.8 years; range 26–69). Initial BMI was 46 ± 7.6 kg/m 2 (range 33–69). At 1, 3, and 5 years BMI was 31, 33, and 34 kg/m 2 , while %EWL was 68%, 65%, and 53%. Changes in BMI and %EWL are shown in Figures 1 and 2.
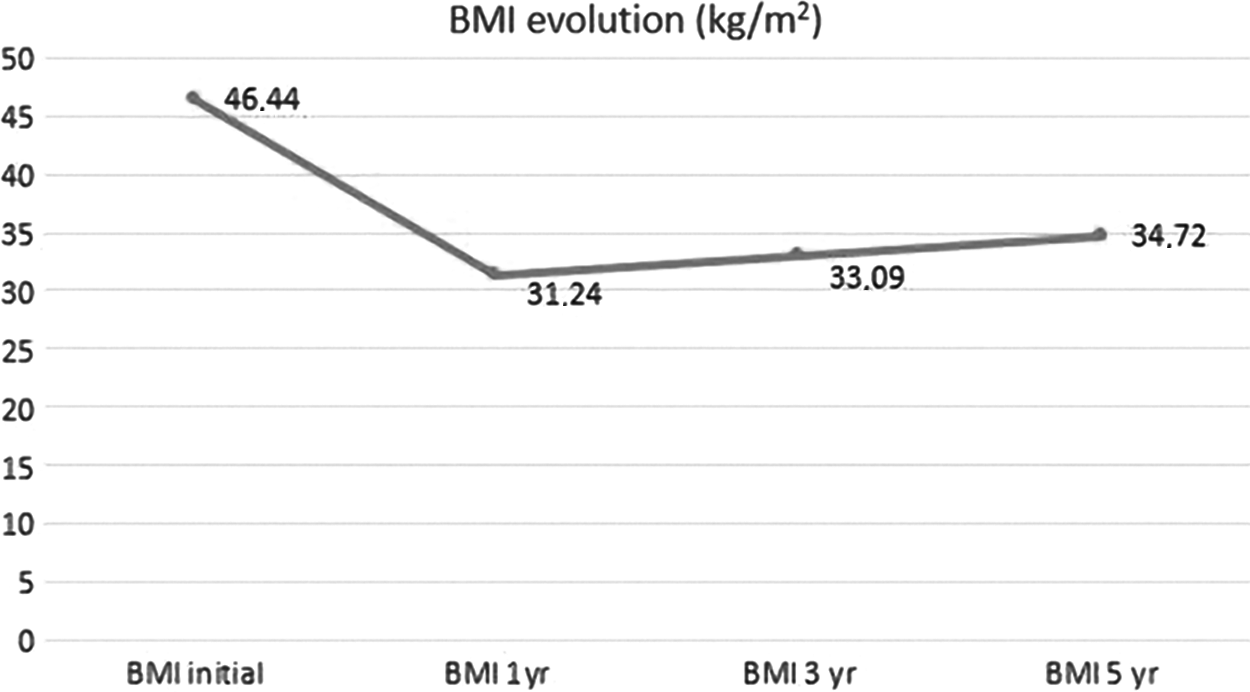
BMI evolution at 1, 3, and 5 years. BMI, body mass index.

%EWL evolution at 1, 3, and 5 years. %EWL, percentage excess weight loss.
Time since T2DM diagnosis was 5.9 years (range 1–28). Operative time was 59 ± 11.5 minutes (range 38–130). Hospital stay was 2.1 days (range 2–5). Follow-up was 65 ± 10 months (range 12–84).
Medication usage
Before the operation, 75.3% (n = 125) of patients were only taking OHD; among them, 52.8% (n = 66) were receiving just one drug, 30.4% (n = 38) two drugs, 15.2% (n = 19) three drugs, and 1.6% (n = 2) four drugs. Of the remaining patients, 13.25% (n = 22) were on insulin therapy; within this last group, 31.8% (n = 7) were on insulin alone, and 68.2% (n = 15) on insulin and OHD. The remaining 11.45% (n = 19) did not receive any medication (Fig. 3).
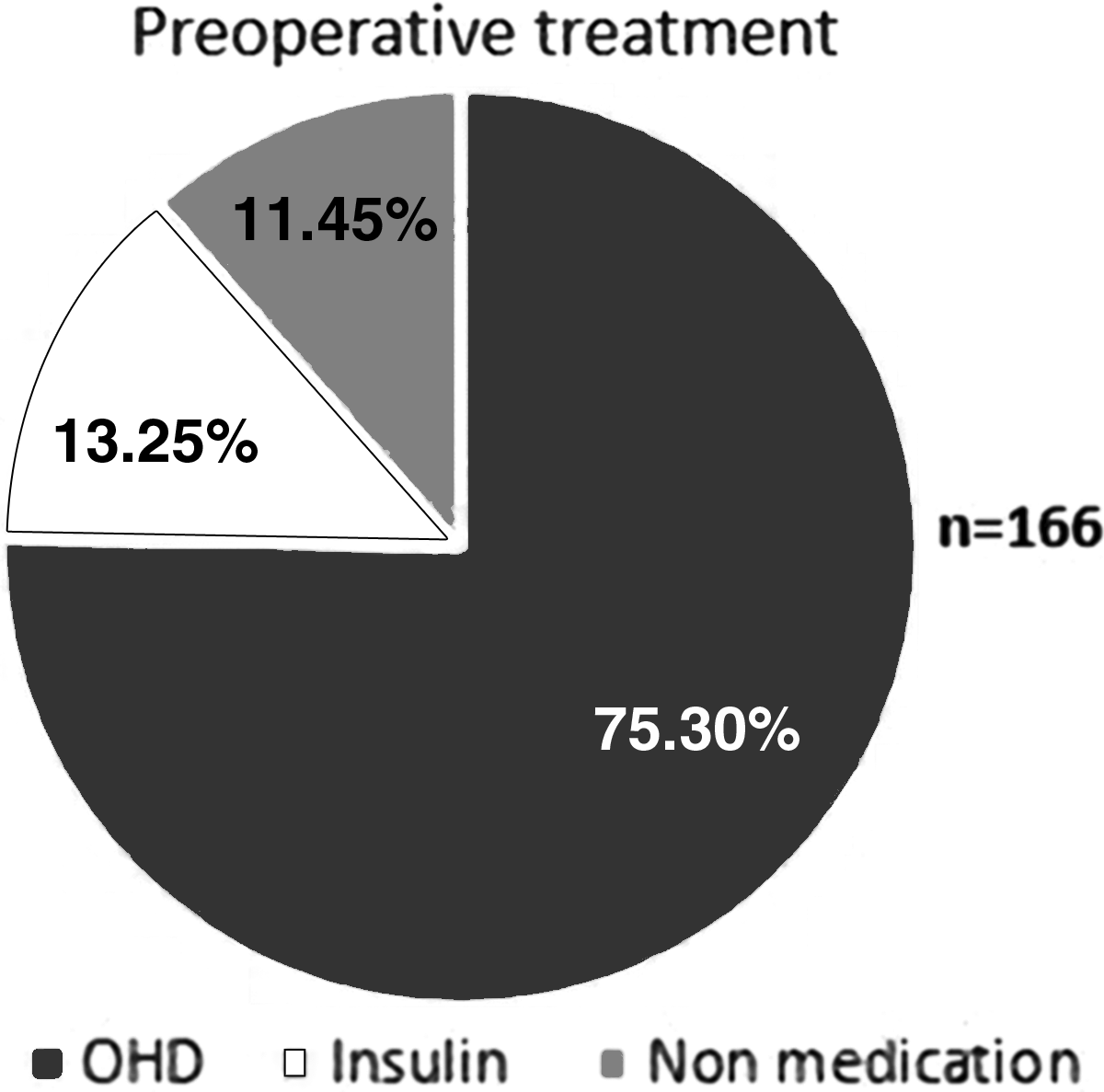
Preoperative treatment. OHD, oral hypoglycemic agents.
Complications
Postoperative morbidity was 2.4% (n = 4). Three patients presented abdominal bleeding; they were managed conservatively, and they did not require blood transfusion. The remaining patient had an intra-abdominal collection, which was managed with percutaneous drainage and antibiotics. There were no conversions to open surgery, no reoperations, and no mortality in this series.
Postsurgical evolution of FG and HbA1c after LSG
Preoperative FG was 140.3 ± 29.3, and HbA1c 7.5% ± 0.9%. FG decreased significantly at 1, 3, and 5 years to 98, 108, and 108.5 mg/dL, respectively (P = .001). Similarly, HbA1c values dropped to 5.8%, 6.3%, and 6.3% at same periods of time (P = .001) (Figs. 4 and 5).
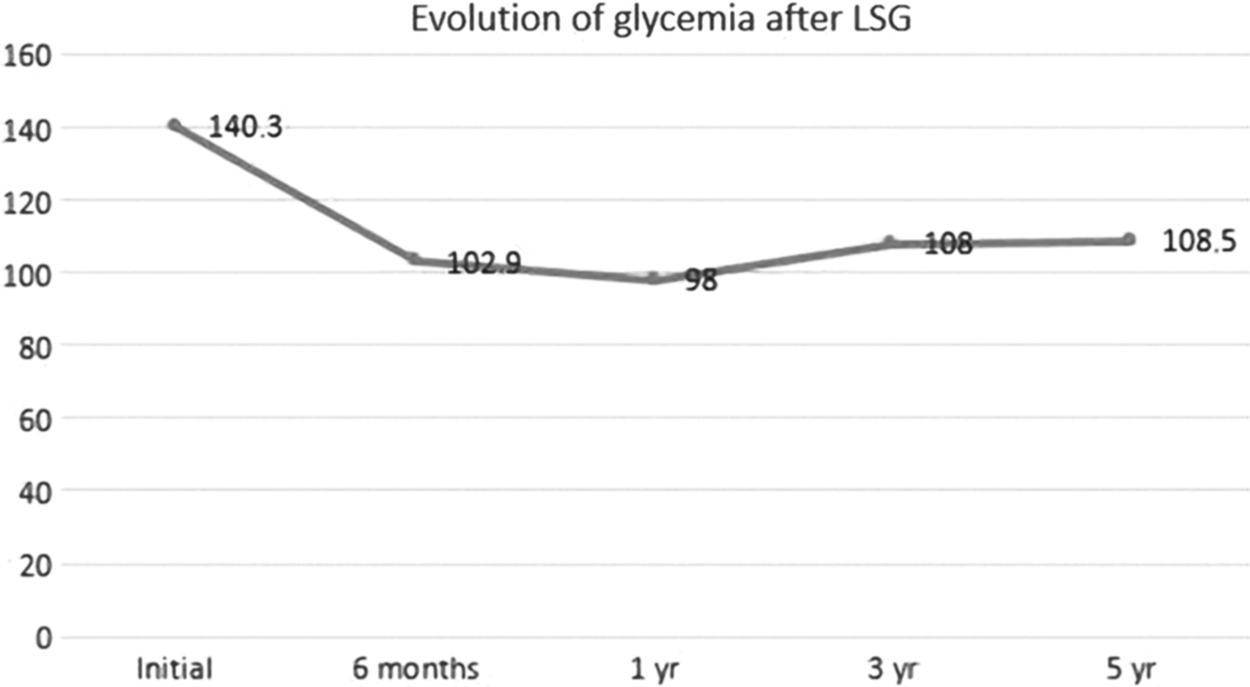
Evolution of glycemia after LSG. LSG, laparoscopic sleeve gastrectomy.

Evolution of HbA1c after LSG. HbA1C, glycated hemoglobin.
Short-term T2DM remission after LSG
Follow-up was achieved in all patients at 1 year. T2DM complete remission was observed in 78.3% (n = 130) of patients (Fig. 6). Then, the results were analyzed according to their preoperative treatment. Before the operation, 75.3% (n = 125) were on OHD. Complete remission was attained in 78.4% (n = 98) of these patients. In contrast, 13% (n = 22) were receiving insulin. Among those, 50% (n = 11) showed complete remission.

T2DM complete remission. T2DM, type 2 diabetes mellitus.
Outcomes were also compared according to time since T2DM diagnosis. At 1- year follow-up, all 166 patients were analyzed; 76 of them were diagnosed ≥5 years before consultation. Remission in this group was observed in 59% (n = 45) of them. The remaining 90 patients had shorter evolution (<5 years) of the disease. Remission was achieved in 81% (n = 73) of patients in the last group (P = .001).
Mid-term T2DM remission after LSG
Follow-up was completed in 59% (n = 98) of patients at 3 years; 75.5% (n = 74) showed complete remission (Fig. 6). Within this group, 86.7% (n = 85) were receiving OHD before the surgery. Remission was observed in 75% (n = 64) of them. We were able to contact all 13 patients who were under insulin therapy before LSG; 30.7% (n = 4) of them continued in complete remission, while 60.3% (n = 9) showed improvement.
T2DM remission at ≥5 years
Five-year follow-up was accomplished in 42% (n = 70) patients. Complete remission was attained in 71.4% (n = 50) of them. Partial remission was observed in 7.1% (n = 5), improvement in 10% (n = 7), while 11.4% (n = 8) experienced recurrence of the disease (Fig. 7).

T2DM status at 5-year follow-up after LSG. T2DM, type 2 diabetes mellitus.
Again, results were analyzed according to their preoperative treatment. Before the operation, 88.5% (n = 62) were on OHD. Complete remission was attained in 72.5% (n = 45) of these patients. In contrast, 11.5% (n = 8) were receiving insulin. Among those, only 37.5% (n = 3) showed complete remission (P = .004)
Also, outcomes were compared according to time since T2DM diagnosis at 5-year follow-up. Among the 70 patients available, 22 were diagnosed ≥5 years before consultation. Remission was seen in 40.9% (n = 9) of them. In the remaining 48 patients who had shorter evolution (<5 years) of the disease, a remission was observed in 70.8% (n = 34) (P = .001).
Recurrence
At ≥5 years, 11.4% (n = 8) of patients showed recurrence of the disease. Age was 49.7 ± 15.2 years (range 28–64), and disease duration was 8.1 ± 4.1 years (range 1–13). Preoperative BMI was 39.6 ± 5.82 kg/m 2 , decreasing to 34.32 ± 4.17 kg/m 2 at 5-year follow-up; %EWL was 54.83 ± 15.2. Preoperative FG and HbA1c were 170 ± 56.9 mg/dL and 8.5% ± 2.1%, respectively. At 1 and 5 years, glycemia was 111 ± 18.2 and 129.4 ± 34 mg/dL, respectively. HbA1c at the same periods was 6.3% ± 0.6% and 6.7% ± 0.9%. Outcomes at 1, 3, and 5 years are shown in Table 1.
BMI, body mass index; %EWL, percentage excess weight loss; HbA1c, glycated hemoglobin; LSG, laparoscopic sleeve gastrectomy.
At the time of recurrence, 87.5% (n = 7) were prescribed OHD, and only 1 patient (12.5%) went back on insulin therapy.
Outcomes on patients receiving insulin preoperatively
Out of all patients, 22 were on insulin therapy before LSG. Age was 53.5 ± 9.5 years (range 36–66), and T2DM duration was 10.68 ± 5.7 years (range 1–28). Pre- and postoperative BMI was 41.3 ± 5.12 kg/m2 (range 38–54) and 34 ± 2.2 (range 28–40), respectively, and %EWL was 58.01% ± 3.5%. Preoperative glycemia and HbA1c were 124 ± 33.5 mg/dL and 7.1% ± 1.3%, respectively. At 1 and 5 years, glycemia was 114 ± 20.9 and 123 ± 30 mg/dL, respectively. HbA1c at the same periods was 6.3% ± 0.6% and 6.7% ± 0.9%. Outcomes of these patients at 1, 3, and 5 years are shown in Table 2.
Discussion
Obesity and T2DM have shown a dramatic growth in prevalence. This problem demands immediate action from the governments, the health system, and the medical community.
Medical treatment including diet and lifestyle changes, plus pharmacologic treatment in some cases, could result in partial improvement in insulin resistance, T2DM, hypertension, and dyslipidemia, decreasing risk factors in this population.4–6
In 2011, the IDF proposed surgery as an adequate treatment option for obese patients with T2DM who had poor metabolic control. They stated that surgical treatment would be a good option not only for obese patients with BMI ≥35 kg/m2 and T2DM but also for those with BMI between 30 and 35 kg/m2 when T2DM could not be controlled by medical treatment, especially in patients with a high risk of cardiovascular disease. 9
The majority of publications that address long-term outcomes on obese patients and T2DM include mainly results after RYGB. So far, short- and mid-term T2DM remission reported was around 67–86%, while long-term remission was between 46% and 80%, RYGB being the standard of care for this group of patients.10–15
In 2012, the American Society for Metabolic and Bariatric Surgery (ASMBS) accepted LSG as a primary surgery for the treatment of obesity. This technique has demonstrated several advantages over other current procedures. Lower morbidity and mortality rates, less invasiveness, lack of malabsorption, possibility of conversion to another procedure in case of failure, coupled with satisfactory mid-term results in terms of weight loss and resolution of comorbidities, represent contributing factors for choosing this technique over others.16–21
Short-term T2DM remission after LSG
Regardless of the different definitions used for T2DM remission, short-term diabetes remission rates after LSG are high, being between 37% and 91%.20,21,23,24 For instance, Gill et al. reported their results on 673 patients at 13.1 months, with an improvement/resolution rate of 93.1%. 23 In contrast, Schauer et al. reported 37% remission in 49 T2DM patients at 12 months. Preoperative HbA1C was 9.2 ± 1.5, duration of the disease 8.5 years, and 44% of them were on insulin therapy preoperatively. 24 The long-time standing of the disease, elevated HbA1C, and high percentage of patients on insulin therapy before the operation might explain the “relative” low remission rate if compared with other publications. In our series, 78.3% of patients achieved remission at 1-year follow-up.
Mid-term T2DM remission after LSG
According to literature, percentages vary from 24% to 94%.25–28 Abbatini et al. observed a remission rate of 87.6% at 3 months, which was stable at around 84.6% at 36-month follow-up. The authors remarked that all 4 patients with no remission were either on high doses of insulin or had poor metabolic control before the operation or had been diabetic for ≥10 years. 25 Schauer et al. reported remission in 24% of patients at 3-year follow-up according to their primary goal, which was HbA1c ≤ 6. 28 In our group, complete remission at 3 years was observed in 76.2%.
Long-term T2DM remission after LSG
Long-term results were less frequently reported. The vast majority of publications exhibited decrease in LSG efficacy with time, although others showed remission rates above 50%, with variations between 11% and 85%.25,29,30 Likewise, Schauer et al. found remission in 7 out of 47 patients (14.9%). 29 Duration of the disease (8.5 ± 4.8 years), high percentage of patients on insulin therapy before LSG (44%), and elevated preoperative HbA1c (9.5 ± 1.7) might serve as interpretation for the low remission rate at 5 years in this set of patients. Aminian et al. demonstrated a significant decrease in HbA1c, FG, and the usage of antidiabetic medication after LSG (P = <.001). Although long-term complete remission was seen in only 11%, partial remission in 15%, and improvement in 47%, this gave a number of 63% of patients with adequate diabetes control after LSG (HbA1c < 7%) versus 31% before the surgery. They concluded that LSG significantly improved glycemic control in T2DM although long-term remission and its maintenance for ≥5 years occurred infrequently. 30 Sieber et al. found 85% remission (normal FG, without antidiabetic medication for 1 year, and HbA1c < 6%) in 62 patients at 5-year follow-up. 31 Other authors reported dissimilar results regarding complete remission.32,33 Our results showed that complete remission was accomplished in 71.4% of patients, partial remission in 7.14%, and improvement in 10% at 5-year follow-up. Patients receiving insulin preoperatively, and with duration of disease ≥5 years, presented lower remission rates (P = .0004 and .0001, respectively).
Outcomes on patients receiving insulin preoperatively
Despite some interesting results coming from some publications, it is clear that remission rates in diabetic patients receiving insulin are lower than in patients treated only with OHD.30,31,33–38 In our study, 13% of patients were receiving insulin. At short-term follow-up, remission was observed in half of them, while the other half showed improvement. Efficacy started to drop at 3-year follow-up, shifting remission rate to 30% and improvement to 70%. At 5 years, 8 patients were available for evaluation; remission was 37.5% (n = 3), improvement 50% (n = 4), whereas 12.5% (n = 1) showed recurrence of the disease. While percentages were lower, >85% of patients were able to obtain either remission or improvement, decreasing the dosage of insulin or eventually receiving only OHD, with adequate metabolic control maintaining glucose values of 123 ± 30.02 mg/dL and HbA1c 6.75% ± 0.9% at ≥5-year follow-up. Golomb et al. demonstrated similar results at 3 years. In their series, 54.5% of patients were able to drop insulin therapy or were able to attain metabolic control just with OHD. 35 At 5-year follow-up, Sieber et al. found remission in 25% of patients who were under insulin therapy before LSG, versus 85% of those who were either on OHD or were not receiving any medication. 31 Aminian et al. found a significant drop in insulin use after LSG, going from 42% to 25% at long-term follow-up (P = .004). 30
T2DM recurrence and associated risk factors after LSG
In our series, 11.4% (n = 8) of patients experienced recurrence of disease at ≥5 years. These patients had longer history of T2DM (P = .0001), FG, and HbA1c significantly higher than of patients who remained with their disease under control (P = .003 and .06, respectively). Only 25% of them were receiving insulin before LSG. It is worth mentioning that during the first year, 100% of them showed either complete remission or improvement. The evolution in this group was as follows: at 3 years, 75% showed complete/partial remission or improvement, and 25% already had recurrence; at 5 years, the total group presented recurrence of disease. Only few publications addressed T2DM recurrence after LSG, with rates between 0% and 44%.25,30,33,37,38 Aminian et al. reported 44% (n = 24) recurrence at long-term follow-up. All of these patients had shown remission initially. The only related factor they could identify was the need for two or more OHD for T2DM control before the surgery (P = .02). Despite the high recurrence rate, 67% of patients who belonged to this subgroup were able to achieve adequate control of their glycemia in the long run, decreasing their dosage of medications, even in patients who were on insulin. 30 Jimenez et al. described 16.2% recurrence after LSG, clearly related to patient's age, preoperative insulin therapy, and weight regain. Disease recurrence was observed approximately 25.2 ± 11.0 months after remission was achieved. 37
Summary
Our long-term results confirmed the benefit of LSG in the treatment of T2DM, showing remission rates of 78.3%, 75.5%, and 71.4% at 1, 3, and ≥5 years, respectively. A significant drop in HbA1c and FG was also observed. Although remission rate in patients under insulin therapy was inferior (37.5%), all of them were able to attain control with lower doses of insulin or even with OHD only. Our recurrence rate is similar to the one reported by others, and undoubtedly related to poor glycemic control before LSG. According to what have been previously discussed, we believe that LSG has a significant role in the treatment of obesity and T2DM, demonstrated by satisfactory long-term weight loss, low morbidity and reoperation rate, becoming a suitable alternative as a first step in the treatment of this disease. The tendency has shown a gradual decrease in efficacy with time; however, we believe that patients were still able to accomplish better metabolic control, even those who were on insulin and those who experienced recurrence of the disease.
Conclusion
Our results showed that at short, mid, and long term, T2DM control was satisfactory after LSG. Patients receiving insulin preoperatively and those with T2DM for ≥5 years revealed significantly lower remission rates.
Footnotes
Disclosure Statement
No competing financial interests exist.