
Abstract
Abstract
Introduction:
Intrathoracic anastomotic leaks after esophagectomy are a significant cause of morbidity and death. Early detection and timely management are crucial. This study evaluates the effectiveness of daily drain amylase levels in detecting early leaks after esophagectomy compared with C-reactive protein (CRP).
Materials and Methods:
Between June 2015 and September 2017, 126 esophagectomies were performed in our department. Amylase levels were collected in 80 of these patients, as long right-sided chest tubes were in place. Mostly, chest tubes were removed before postoperative day (POD) 5. CRP levels were measured daily. Early leaks were defined as occurring with the chest tubes in place. According to the obtained receiver operating characteristics curves, amylase levels >335 U/L, and CRP >30 mg/dL were considered positive. Sensitivity and specificity for both drain amylase and CRP were calculated.
Results:
Overall anastomotic leak rate was 7.5% (6/80). An early disruption occurred in 4 of 80 patients (5%). Three patients had a positive amylase level and none a positive CRP on POD 1. These 3 patients had on POD 2 a positive CRP. The fourth patient presented at POD 2 bilious secretion in the chest tubes. He showed normal amylase and CRP levels on POD 1. Sensitivity and specificity for amylase level and CRP within the first 3 PODs were 0.75 and 0.98 versus 0.75 and 0.85, respectively. The patients with leak were reoperated at POD 2. They were all discharged between PODs 15 and 19.
Conclusions:
Amylase level after esophagectomy is a more accurate screening tool for detection of early leaks than CRP. It could facilitate their detection up to 24 hours earlier than CRP.
Introduction
I
Several authors have already suggested the measurement of chest-drain amylase as a cheap and routinely available alternative to other diagnostic methods, but none of them considered this procedure as a screening tool for early leak detection.
Our study compares the prognostic effectiveness of daily chest-drain amylase levels and CRP for detection of early intrathoracic anastomotic leaks after Ivor Lewis esophagectomy.
Materials and Methods
In the Surgical Department of the Nuremberg Hospital (Paracelsus Medical University, Nuremberg, Germany), 126 Ivor Lewis esophagectomies for cancer were performed over a 28-month period. Eighty of these patients consented to the study protocol.
Ivor Lewis esophagectomy was performed in four different technical variations: full-open (laparotomy+thoracotomy), hybrid-laparoscopic (laparoscopy+thoracotomy), hybrid-robotic (robotic-assisted laparoscopy+thoracotomy), and full-robotic (robotic-assisted laparoscopy and thoracoscopy) (Table 1).
If the thoracic step of the operation was done through thoracotomy, the esophageal anastomosis was performed as end-to-side esophagogastrostomy with a 25 mm circular stapler. Otherwise, if done robotic-assisted, the anastomosis was hand-sewn as a side-to-side esophagogastrostomy. Before placing the chest tubes, an irrigation of the chest with at least 1 L physiologic solution was performed to wash up any contaminating fluids. The right chest was drained with two 24 Fr chest tubes, placed, respectively, in the upper and in the lower chest. The nasogastric tube was removed already at the end of the operation.
Chest-drain amylase levels were collected daily from the chest tube placed in the lower chest as long as it was in place. Chest tubes were sequentially removed by a secretion volume <300 mL a day (mL/24 hours). CRP levels were routinely measured during the stay in the intensive care unit and in the observational ward. If bilious secretion was detected in the chest tubes or during an intervention/reoperation for suspected anastomotic disruption, no further data were collected.
An early anastomotic leak was defined as a full-thickness lesion involving the anastomosis or the gastric conduit (staple line) requiring intervention or reiteration (grade III complication according to the Clavien–Dindo Classification 14 ) occurring within postoperative day (POD) 5, with the right-sided chest tubes still in place. Surgery was undertaken when a clinical sign showing a possible leakage occurred, for example: bilious secretion in the chest tubes, CT scan or endoscopy showing a contrast leakage or visual sign of a disruption, empyema, or sepsis without any other cause. Data concerning tumor's and patients' characteristics, operative technique, anastomotic leaks, amylase levels, CRP levels, and 30-day mortality were prospectively collected and retrospectively analyzed. According to the collected data and the obtained receiver operating characteristics (ROC) curves, drain amylase levels >335 U/L and CRP >30 mg/dL were considered positive. Sensitivity, specificity, and accuracy in detecting anastomotic insufficiency for both drain amylase and CRP were calculated.
Statistical analyses were performed using R 3.1.0 software. 15
Results
Eighty patients were included in the study. One 84 years old patient died on POD 6 by acute heart failure due to a central bilateral lung embolism. In most patients, chest tubes were removed within POD 5 (mean: POD 5, range: PODs 3–8). Patients' and cancer characteristics are given in Table 2.
The overall anastomotic leak rate was 7.5% (6/80). An early anastomotic disruption occurred in 4 of the 80 patients (5%). All early disruptions became clinically evident on POD 2 (Table 3). In our series, 3 out of 4 patients who developed a disruption had a positive amylase level and none a positive CRP on POD 1. On POD 2, these same patients had a positive CRP level or presented bilious secretion in the chest tubes. The fourth patient had neither positive amylase nor CRP level on POD 1, but had bilious secretion in the chest tubes on POD 2. A fifth patient presented (false)-positive amylase level and CRP on POD 3, but an anastomotic disruption did not become evident. On POD 3, false-positive CRP levels were detected three more times. Furthermore, false-positive CRP levels were also detected two times on POD 4 and three times on POD 5.
The 5th patient showed positive amylase and CRP but no leak.
CRP, C-reactive protein; POD, postoperative day.
Two further patients presented a late leak, both on POD 12. Both leaks were detected using a CT scan. At that point, the first patient presented a CRP level of 5.2 mg/dL, but he was circulatory and respiratory instable. He underwent rethoracotomy and the leak was oversutured. The second patient presented with acute chest pain after oral food intake. The patient underwent endoscopy and the leak was covered with a self-expandable metallic stent. At that point, he presented a CRP level of 5.8 mg/dL.
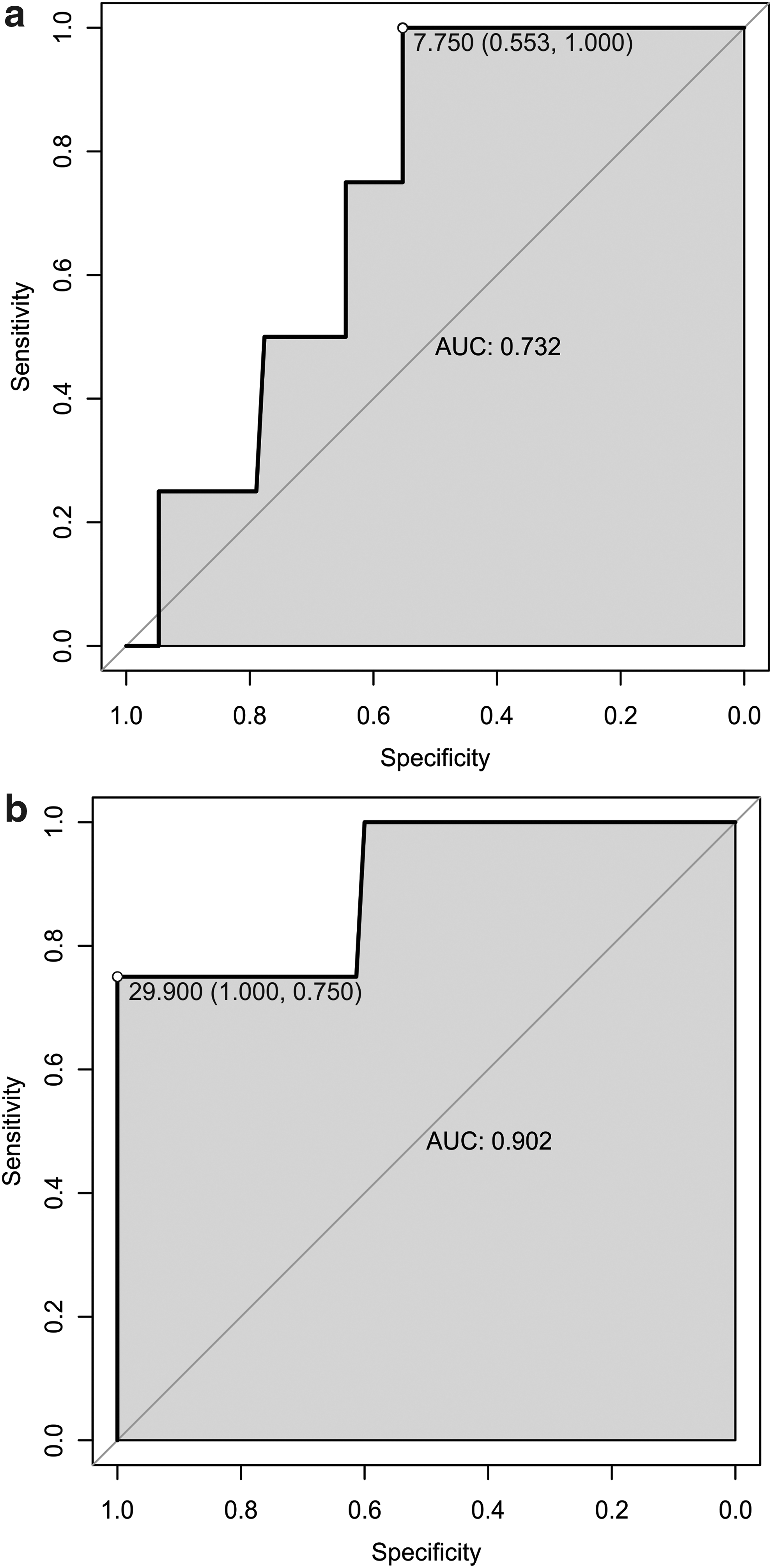
The ROC curves for amylase levels on POD 1 and for CRP levels on POD 1 and POD 2 were drawn. The area under the curves (AUC) (Figs. 1 and 2a, b) and the optimal cutoffs for both (amylase and CRP) tests were calculated. Within the first 3 PODs, an amylase cutoff of 335 U/L showed a sensitivity and a specificity of 75% and 98%, respectively. Sensitivity and specificity for a CRP cutoff of 30 mg/dL were 75% and 85%, respectively. Considering sensitivity for both variables related only to POD 1, it was 75% for amylase versus 0% for CRP. The specificity on POD 1 was 100% for both values. The accuracy for both amylase and CRP was 98% and 85%, respectively.
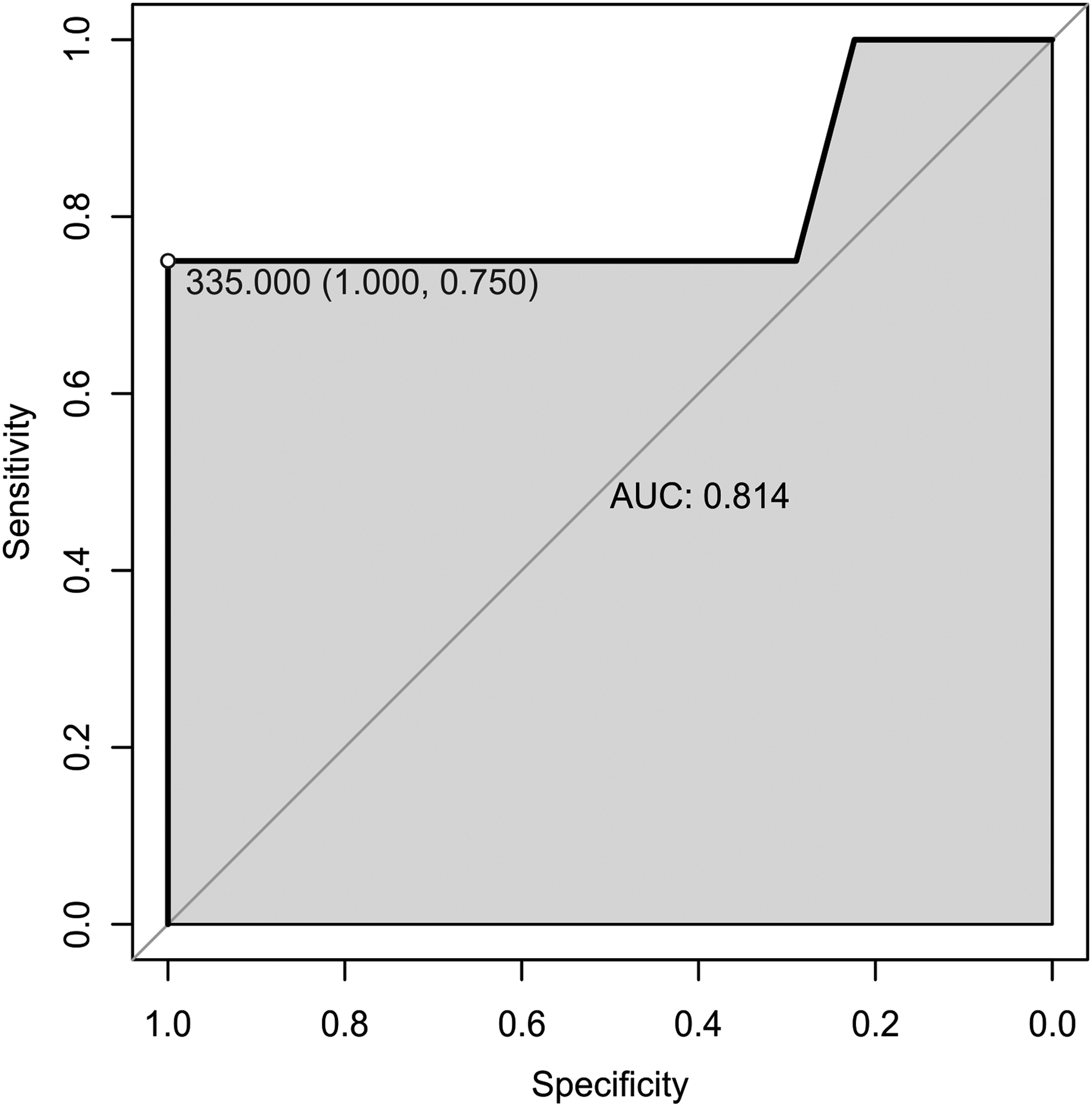
ROC curve for amylase at POD 1. POD, postoperative day; ROC, receiver operating characteristics.
The 4 patients who developed a leak underwent a rethoracotomy on POD 2. The leak was oversutured in 3 patients. The fourth patient underwent replacement of the anastomosis in the neck. After revision, further interventions or reoperations were not necessary. Food intake was regularly initiated on POD 5, according to our internal protocol. All the patients were regularly discharged between PODs 15 and 19 without any long-term consequence.
Discussion
This is the first study that compares chest-tube amylase with CRP levels as a screening tool for detection of early anastomotic leaks after esophagectomy. It demonstrates that chest-tube amylase has higher prognostic accuracy than CRP, because it can facilitate the identification of early leaks up to 24 hours earlier.
The most important factor influencing the outcome after treatment of an esophageal leakage is the time interval between the onset of the leak and its definitive therapy, which should not be >24 hours.9–11
The standard available methods for monitoring and detecting an esophageal anastomotic leak range from daily blood sampling (CRP) to endoscopy.
Contrast swallow is commonly used to detect an anastomotic leak but this procedure has severe limitations and a low sensitivity. Cools-Lartigue et al. prospectively collected data regarding the effectiveness of barium swallow in detecting anastomotic leaks after esophagectomy. 16 Between 2005 and 2011, 221 patients were examined. The authors concluded that because of its low sensitivity (45.5%) and its association with adverse events such as aspiration and mediastinitis, routine barium esophagram is not an effective screening modality for anastomotic leaks.
Another modality that is often favored is the CT scan with contrast swallow. Higher sensitivity (>54%) has been reported for this procedure,17,18 nevertheless it is also associated with a high risk of aspiration; therefore, it cannot be suggested as a routine screening examination.
Endoscopy has also been proposed by several authors as standard procedure to identify anastomotic leaks.19,20 If performed by an experienced endoscopist, it is a safe method for detecting anastomotic leaks with sensitivity and specificity rate of 100%. 21 However, daily endoscopies in every patient after an esophagectomy are not feasible; therefore, also this procedure is only to be performed in case of a suspected anastomotic breakdown rather than routinely. 22
The first trial with amylase detection after esophagectomy dates back to the year 1996 as Machens et al. prospectively investigate this method for detecting early leaks after esophagectomy with gastric pull-up and cervical anastomosis. 23 Out of 14 patients, 6 developed a leak. In this study, the analyzed number of patients is very small. The rate of anastomotic disruption is unusually high, which could be explained by the placement of a drain in the cervical anastomotic site. For this consideration, in our department we do not place any cervical drainage at all.
The first large series with amylase measurements from the chest tubes after transthoracic esophagectomy with intrathoracic anastomosis was published in 2015. Baker et al. retrospectively reviewed data of 100 patients after minimal invasive esophagectomy, collected in their surgical center between November 2009 and April 2014. 24 Ninety-eight patients received an intrathoracic anastomosis. A leakage occurred in 13% of the patients. This group has been using a routine CT esophagram at POD 7, 8, or 9 for evaluation of the conduit integrity before initiating oral food intake. Many aspects of this study are controversial. For the reasons already explained (aspiration risk and low sensitivity), CT esophagram should not be used routinely in asymptomatic patients. In addition, because of the postulated postoperative contamination of the thoracic cavity and to avoid false-positive measurements, chest tube amylase was collected starting on POD 6 only, which excludes the detection of the anastomotic complications occurring on PODs 1–5. Contamination of the thoracic drainage can be prevented with intraoperative saline irrigation at the end of the operation.
Berkelmans et al. published multicentric retrospective data of a series of 89 patients who underwent minimal invasive esophagectomy for cancer. 25 Fifteen patients (16.9%) developed a leak and all cases were confirmed with endoscopy. Chest-tube amylase levels were measured daily from POD 1 until drain removal or until POD 6. Drainage amylase levels were significantly higher in patients with anastomotic rupture (384 U/L [median] versus 37 U/L in patients with no leak, P = .003). Despite a high specificity between 94% and 95.7%, sensitivity was 21.4% to 35.7% only. Even though the methods of this group are very similar to ours, the obtained results partly discord with our outcomes, since the sensitivity of chest-tube amylase was much higher in our study. Nevertheless, a cutoff of 350 U/L at POD 1 seemed to be suitable for detection of a leak, according to our results.
One of the largest studies in this subject was published by Perry et al. 26 One hundred forty-six patients were included in this study, but only 25 (17.1%) of them underwent an Ivor Lewis esophagectomy. Amylase levels for all patients were recorded from POD 1 to POD 5 daily, unless an anastomotic complication became apparent earlier. Anastomotic rupture rate for the Ivor Lewis group was 12%. For any kind of leak, a cutoff of 234 U/L accurately classified 88.2% of patients with a sensitivity of 50% and a specificity of 97.7%. The heterogeneity of the study population that consists of a majority (82%) of cervical anastomosis makes the results obtained from Perry et al. difficult to compare with our study and to interpret at all. In a subsequent publication, the same group confirmed its observations and proposed a protocol for enhanced recovery after esophagectomy based on amylase levels. 27 The anastomotic leak rate was high (23%) and the patient with intrathoracic anastomosis represented a small part of the study population. Anyway, sampling of chest-tube amylase seemed to be suitable to identify patients who are appropriate for early food intake and discharge.
Recently, a further study was published by Miller et al. 28 Forty-five patients who underwent an Ivor Lewis esophagectomy over a period of 18 months were included. Chest-tube amylase levels were daily recorded starting on POD 3 only, to avoid possible false-positive values due to contamination. Peak values were reported (227, 630, and >4000 U/L), nevertheless it was not explicitly described at which POD they were measured. Furthermore, it was not reported what for a level was measured the day before the disruption was identified, except for 1 case. The authors did not suggest an amylase level that could be probably associated with a leak. They also did not publish their statistical methods, but they reported in a table (table 5 in Miller et al.) a 100% sensitivity and a 100% specificity for amylase levels >200 U/L.
In contrast to this experimental method, CRP is a widely used laboratory value for monitoring systemic inflammatory response 29 and it has also been suggested as a marker for early detection of postoperative complication after esophagectomy. 30 Warschkow et al. 13 assessed with their retrospective study with meta-analysis the accuracy of CRP, after surgery for gastroesophageal cancer, in predicting and diagnosing postoperative inflammatory complications. Two hundred ten patients were included. CRP was identified as a performing marker for postoperative inflammatory complication only up to POD 4. Because of the low diagnostic accuracy (AUC 0.77, 95% CI, sensitivity 0.78, specificity 0.70 by a cutoff of 14.1 mg/dL), CRP was classified as with a low-to-moderate diagnostic value. The authors suggested that in case of elevated CRP levels, further diagnostic measures should be added.
Similar results were reported by Park et al. in their retrospective single-center study. 31 One hundred seventy patients out of 201 underwent an Ivor Lewis resection. CRP was identified as a significant marker for anastomotic leak only up to POD 3.
The presented studies aimed to establish a cutoff value for CRP as a predictor for postoperative complications. The results, however, are conflicting since the complications were not accurately stratified. Several other studies aimed to define a CRP level as marker for anastomotic disruption, but they included mostly patients after colorectal surgery.32–34
Because of the conflicting data in the literature, Straatman et al. proposed in 2015 a prediction model for major complications as a function of continuous CRP levels on POD 3, which was identified as the POD with highest sensitivity. 35 After this risk assessment, a cutoff may be established at the discretion of the surgical department.
Based on previous literature and the obtained ROC curve, we decided to establish our cutoff for CRP at 30 mg/dL. In our series, increased CRP levels up to the predefined cutoff were observed in 3 of 4 patients who developed an anastomotic disruption, but only on the day in which the leak became also clinically evident. On the contrary, positive amylase levels were identified already 24 hours earlier, at a time in which clinical signs were not yet apparent. This was the most important observation of our study. It showed that, compared with CRP, chest-tube amylase is probably a better screening tool for detection of early anastomotic leaks. Despite our results, a later removal of the chest tubes for prolonged sampling of amylase is not justified.
Amylase sampling could facilitate the identification of patients with early anastomotic rupture who could benefit from early reoperation, in a time frame when oversuturing the anastomosis is still possible. In our series, rethoracotomy on POD 2 with oversuturing or even replacement of the anastomosis was feasible in all patients, with excellent outcomes.
Because of the reproducibility and the low cost of the technique, a more frequent (every 12 rather than 24 hours) sampling of chest-tube amylase could be considered to further refine the method. Furthermore, CRP should be probably still considered as a marker for late esophageal disruptions.
This study has some limitations. First, it is a single-center study with the obvious biases. Second, several very different cutoffs for chest-tube amylase have already been proposed.23–27 In our study, the cutoff of 335 U/L seemed to be the most accurate and reliable. Nevertheless, the small sample size (four early leaks only) could have influenced the statistical analyses, resulting in an overstatement of the results.
To allow the identification of a clear cutoff and to prove reliability and reproducibility of the procedure, a multicentric prospective study is needed.
Footnotes
Acknowledgment
We thank Mr. Daniel Tietze for the support in preparing the graphs.
Disclosure Statement
No competing financial interests exist.