
Abstract
Abstract
Background:
Re-radical surgery is the only curative therapy for unsuspected gallbladder carcinoma (UGC). The aim of this study was to compare prognosis of pT3 UGC patients receiving anatomic hepatectomy (AH) or wedge hepatectomy (WH) combined with en bloc local-regional lymphadenectomy of the hepatoduodenal ligament using propensity score-matching (PSM) analysis.
Materials and Methods:
A retrospective study was carried out on 81 consecutive pT3 UGC patients who underwent radical re-resection at Eastern Hepatobiliary Surgery Hospital from 2006 to 2015. Overall survival (OS) was estimated using Kaplan–Meier method. The difference in OS between the AH and WH groups was analyzed using the log-rank test and the PSM method.
Result:
The AH and WH groups showed no significant difference in OS (P > .05) by either log-rank test or PSM analysis.
Conclusions:
Both AH and WH radical re-resections are effective treatments for UCG patients with pT3 tumors.
Introduction
Despite common use of ultrasonography and computed tomography (CT), only 30% of gallbladder cancer (GBC) patients are diagnosed preoperatively. The remaining 70% cases are diagnosed by pathological examination of biopsy specimens from patients who undergo cholecystectomy for the treatment of benign gallbladder diseases and, therefore, are called unsuspected or incidental GBC (unsuspected gallbladder carcinoma [UGC] or IGBC).1,2 UGC is diagnosed in 0.3%–2% of all cholecystectomies, often at late stage.3,4 Chemo- and/or radiation therapy do not significantly improve GBC patient survival,5,6 and complete re-resection seems to be the only curative therapy. 7 However, even for patients diagnosed at an early stage and undergo R0 resection, the 5-year survival is merely 17%. 8
Because of high residual tumor rate for UGC patients receiving cholecystectomy, multidetector CT (MDCT) and magnetic resonance imaging (MRI) are often used for postoperative restaging.9,10 R0 re-resection is considered the gold standard treatment for UGC patients with up to pT2 tumors. There are two common operative procedures for R0 re-resection: hepatectomy of the gallbladder fossa with a 3–4 cm margin in the liver (wedge hepatectomy [WH]) or hepatectomy of liver segments 4b and 5 (anatomic hepatectomy [AH]) combined with en bloc local-regional lymphadenectomy of the hepatoduodenal ligament (LRLHL). 11 Current literature reports suggest that WH combined with LRLHL is the preferred procedure for GBC up to pT2.2,10–14
Extended resection is recommended for advanced GBC with liver presence. On one hand, the incomplete resection or the tumor plane with occult seeding during the initial cholecystectomy may be related to the gallbladder commonly heavy inflammation and the depth of invasion through the dissection plane. On the other hand, the initial pathological tumor staging can be inaccurate due to the lack of information about the invasion the cystic duct margin and the cystic artery lymph node. However, for tumors that do not invade the liver, the benefits of extended hepatectomy remain controversial.2,12–14 In this study, we evaluated the prognosis of 81 pT3 UGC patients who underwent radical WH or AH combined with LRLHL at our hospital for a period of 10 years.
Materials and Methods
This study was approved by the Research Ethics Committee at Eastern Hepatobiliary Surgery Hospital (EHBH). A total of 81 consecutive UGC patients with pT3 tumors who underwent radical re-resection surgery at EHBH between February 2006 and September 2015 were included in the study. The diagnosis was made after the initial cholecystectomy at another hospital. The medical records of patients were obtained by contacting the initial attending surgeons. All patients were restaged at EHBH based on results from physical examination and diagnostic imaging with MDCT, MRI, and/or 18F-fluorodeoxyglucose positron emission tomography. The original pathological slides were re-evaluated at pathology department of EHBH to confirm the diagnosis before restaging. The clinicopathological data of patients included the depth of tumor invasion (T stage), the grade of tumor differentiation, the presence of perineural and/or lymphovascular invasion, inflammation, and the presence of benign gallbladder diseases associated with cancer (gallstones and/or polyps). A positive resection of cystic duct was defined as its margin <1 mm. Lymph node metastasis (N1 disease) was defined as tumor presence in at least one lymph node resected. Depth of tumor invasion and lymph node metastases were categorized based on the AJCC staging manual (the 7th edition). Histological differentiation was categorized as full, moderate, poorly differentiated, or unclear.
Radical surgery was recommended for all patients. The protocol of radical surgery included the type of hepatectomy with a WH or an AH, and en bloc LRLHL was carried out, and the lymphadenectomy around the pancreatic head, duodenum and celiac artery, and port site resection was also performed by surgeon's preference; common bile duct resection (CBDR) was performed selectively to achieve clear margins when there was definite or suspected presence.
The postoperative complications were graded retrospectively according to Clavien-Dindo classification. 15 No patients died of postoperative complications. Outpatient follow-up was conducted every 3–6 months by telephone interviews with surgeons, patients, and family members of the patients. Physical examination was performed at least once every 3 years, and measurements of CEA and CA 19–9, abdominal ultrasonography, MDCT scanning or MRI were carried out when necessary. Because the efficacy of adjuvant therapy for GBC has not yet been clearly established,5,6 neither adjuvant chemotherapy nor radiation is routinely performed in our institution. Follow-up data up to August 31, 2016 were included in this study.
Statistical analysis
Baseline parameters are presented as numbers and percentages (%), means ± standard deviation or medians and interquartile ranges. Between-group differences were interpreted using the Fisher's exact test, chi-square test, Mann–Whitney U-test, or Student's t-test. Overall survival (OS), defined as the time from initial surgery to death, was estimated using the Kaplan–Meier method, and survival curves were compared using the log-rank test. Multivariate analysis of significant variables (enter: P < .10, and the significance was P < .05) was performed using Cox regression. Propensity score-matched (PSM) comparisons of WH versus AH were performed using Fisher's exact test or chi-square test. The PSM technique (with nearest neighbor 1–3 ratio) was employed to minimize possible selection bias and confounder effects. All analyses were performed using SAS 9.4 software (SAS Institute, Cary, NC). Differences with a two-tailed P value of <.05 were considered statistically significant.
Results
Patient characteristics
Patients' baseline demographic and clinical characteristics are summarized in Table 1. Of the 81 pT3 UCG patients, 25 (31%) were men and 56 (69%) were women. Seventy patients (86%) presented with cholecystolithiasis and cholecystitis, and 14 (17%) presented with polyposis lesions and cholecystitis. The majority of patients (n = 53; 65%) had undergone laparoscopic cholecystectomy (LC). The numbers of liver metastasis, positive cystic duct node metastasis, and positive margin of cystic duct were 10 (12%), 6 (7%), and 15 (19%), respectively. After restaging, the numbers of AJCC stage 3A and 3B tumors were 75 (93%) and 6 (7%), respectively; the numbers of patients receiving AH, WH, LRLHL without CBDR, extended lymph node dissections, CBDR, and resection of laparoscopic trocar sites were 12 (15%), 69 (85%), 49 (93%), 28 (35%), 6 (7%) and 9 (11%), respectively. Trocar sites metastasis was not detected in any patient. The median survivals of the AH and WH groups estimated by Kaplan–Meier method were 54 and 49 months, respectively, with no significant difference detected between the two survival curves (F = 0.0001, P = .992). The OS of the patients with liver metastasis, positive margin of cystic duct, lymph node metastasis, and residual tumor are shown in Supplementary Figure S1.
Baseline Characteristics of 81 Patients with pT3 Unsuspected Gallbladder Cancer
Continuous variables are expressed as mean ± SD or median with IQR; categorical variables are expressed as number and percentage.
AH, anatomical hepatectomy; AJCC, American Joint Committee on Cancer; CBDR, common bile duct resection; IQR, interquartile range; LC, laparoscopic cholecystectomy; OC, open cholecystectomy; SD, standard deviation; WH, wedge hepatectomy.
By univariate analysis, the hepatectomy type had no significant impact on OS in pT3 UCG patients receiving re-radical resection (F = 0.909, P = .340). By multivariate analysis, the residual tumors had a significant impact on OS (F = 17.756, P < .0001).
Seven pairs of AH and WH patients receiving re-radical resection were created (7 AH and 21 WH, 1:3) by PSM. A homogeneity test revealed that no significant difference was found in between the two matched groups. And analysis of two types of hepatectomy were compared by the PSM method in pT3 UGC, which showed that there was no significant difference in OS between any matched pairs (Fig. 1).
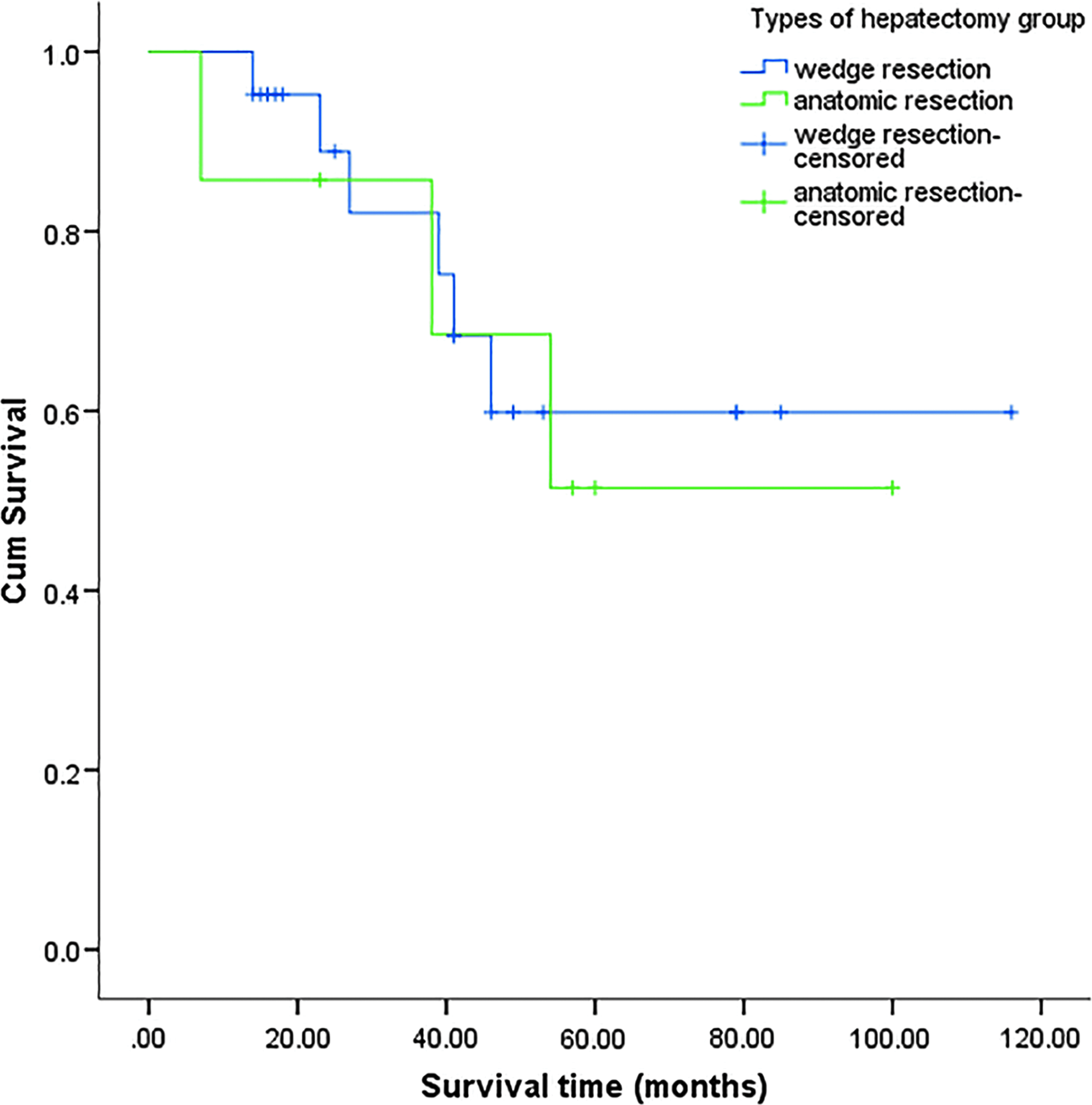
The overall survival of two types of hepatectomy of 7 pairs (1:3) patients with pT3 unsuspected gallbladder carcinoma were compared by the propensity score-matching method (.813, log-rank test).
Discussion
For many years, laparoscopic surgery as a curative treatment for UGC has been contraindicated. Nowadays, the rising number of LCs has led to increased diagnosis of UGC at an early stage and thus improved prognosis of patients. Early postcholecystectomy restaging, now a policy in GBC management, has found a high rate of remnant disease.9–11,16 In addition, minimally invasive techniques have been widely used in GBC staging and surgery. In 23%–62% of GBC patients, staging can be completed using laparoscopy instead of the more invasive laparotomy. 17 GBC patients receiving radical laparoscopic surgery have enjoyed the same long-term survival as those receiving open radical re-resection.18–21 Nonetheless, the criteria for UGC patient selection for surgery and the preferred operative procedure are still under debate.5,6,22
Hepatectomy is necessary for UGC treatment if the tumor has spread through the gallbladder wall into the liver and/or micrometastases have been found in an area of 15–27 mm. 23 Many studies have recommended WH of the gallbladder fossa with margins ranging from 1 to 5 cm or a major AH.1,3,4,11,24,25 Goetze et al. 3 have reported that WH of the gallbladder fossa with a 3 cm margin combined with LRLHL is associated with better prognosis in pT1b tumors, whereas AH is linked to better survival of pT2 tumors. However, controversy still exists regarding the preferred operative procedure for pT3 tumours.2,13,14,26 Considering that the goal of hepatectomy is to achieve an R0 resection,5,11 AH seems to be the method of choice for late-stage tumors because it tends to produce better tumor clearance.14,27,28 However, Fuks et al. 2 compared the clinical outcome in pT3 UGC patients receiving WH, AH, or hemihepatectomy, and found that more radical liver resection failed to improve survival. Similarly, a few other studies have showed that, compared with WH or AH, major hepatectomy has not been associated with improved survival, but has been linked to increased postoperative complications.2,9,29
In this study, we found that pT3 UGC patients receiving WH of the gallbladder fossa with a 3–4 cm margin had similar OS to those receiving AH. Furthermore, data comparison using the PSM analysis showed no significant difference in OS between the WH and AH groups. Since the PSM technique adjusted for differences in demographic and clinical characteristics between the two groups, the results are likely reproducible despite the small sample size in this study. Considering that WH is generally associated with a lower risk of postoperative complications than AH, we would recommend WH for pT3 UGC patients.
The reported median interval time from initial cholecystectomy to re-resection vary from 14 to 90 days.11,12,29 The decision on early or delayed re-resection often results from an interplay of technical issues and patient selection. Although reoperation within 4–8 weeks after the initial cholecystectomy is strongly recommended, 30 we did not observe a significant impact of re-resection time on outcomes. For the purpose of avoiding too much time for tumor dissemination, we would recommend the interval time of reoperation for pT3 UGC patients no later than 4 weeks after initial cholecystectomy.
This study has several limitations. It is a single-center retrospective study, the patients were referred from other hospitals, and the sample size is relatively small. In addition, the precise tumor location (the “liver” or “peritoneal” side of the gallbladder) was not specified. However, the PMS analysis used in this study may render the results more credibility than previous single institution reports.
Conclusion
In summary, pT3 UCG patients receiving radical WH combined with en bloc LRLHL showed similar OS to those receiving radical AH combined with en bloc LRLHL.
Footnotes
Acknowledgments
We thank Large-scale Data Analysis Center of Cancer Precision Medicine-LinkDoc database for their assistance in clinical and pathological data collection. This study is sponsored by Shanghai Science and Technology Committee (09411965400) and National Natural Science Foundation of China (81172303).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.