
Abstract
Abstract
Background and Objectives:
The formation of a fistula between the gastrointestinal tract and cardiovascular system is a rare but devastating condition. Although clinical diagnosis is suspected, autopsy confirmation is rarely obtained. Advancement in the treatment of esophageal cancer could result in an increased risk of enterovascular fistula formation. We describe autopsy-proven series of enterovascular fistulas with particular focus on this complication developing as a consequence of esophageal cancer therapy.
Methods:
Cases of enterovascular fistulas were retrospectively identified in the institutional autopsy case records (1994–2017). Relevant clinical information and pathologic findings were reviewed.
Results:
Nine cases were identified. Seven out of 9 were related to malignancy, with 6/9 occurring in the setting of treated esophageal carcinoma. This esophageal cancer group was a unique set of patients (age median: 71 years) with male predominance (M:F-5:1) presenting with hematemesis as the main symptom. All patients had advanced disease at diagnosis and the complication generally occurred late after treatment (mean interval: 1.7 years). The fistula site was between the esophagus and variety of vascular structures. The most common etiology was tumor invasion (4/6). The diagnosis of enterovascular fistula was made postmortem in all cases.
Conclusions:
The development of enterovascular fistulas is a late complication of treated esophageal cancer. Tumor invasion, infection, and radiation response are the leading etiologies. Early recognition and aggressive treatment may salvage this highly morbid complication.
Introduction
T
Esophageal cancer incidence has been rapidly increasing all over the world in the past decades. 6 The increasing availability of multimodal therapy, including esophageal resection and complex reconstructive surgery, chemotherapy and radiation therapy for esophageal carcinoma, has led to better symptomatic control and improved survival. 7 However, this increased utilization of multimodal treatment could result in an increased risk of enterovascular fistula formation as a complication, with the genesis now being the gastrointestinal system. Here we describe a series of autopsy-proven enterovascular fistulas with particular focus on this complication developing as a consequence of therapy for esophageal cancer. The rarity of this complication and the lack of autopsies done in this patient population limit our knowledge on the link between treated esophageal cancer and enterovascular fistula formation. Most of the current data comes from historical series and case reports.
To our knowledge, this is the first study aimed to investigate the correlation between treated esophageal cancer and the development of enterovascular fistula.
Methods
After obtaining appropriate institutional review board approval, cases of enteric fistulas to heart and/or large vessels were retrospectively identified in the autopsy case records of the Brigham and Women's Hospital (1994–2017). Relevant premortem clinical information was collected from the electronic medical record. Gross photographs and glass slides were also independently reviewed with 2 expert autopsy pathologists to collect relevant gross/microscopic findings. Statistical analysis was performed using the GraphPad Prism statistics software package.
Results
Nine autopsy cases with anatomic evidence of an enterovascular fistula were identified (Table 1). The cause of death was related to the fistula in all cases. The initial presentation was hemoptysis and/or hematemesis in all cases, with 2 patients also presenting with signs and symptoms of sepsis. The majority of cases (7/9) were directly or indirectly related to malignancy. The remaining 2 cases were related to endovascular aortic repair and pulmonary vein isolation procedures, respectively.
Clinical and Pathologic Characteristics of All Identified Cases of Enterovascular Fistula
ICA, internal carotid artery fistula; IVC, inferior vena cava; SCC, squamous cell carcinoma; TEF, tracheo-esophageal fistula.
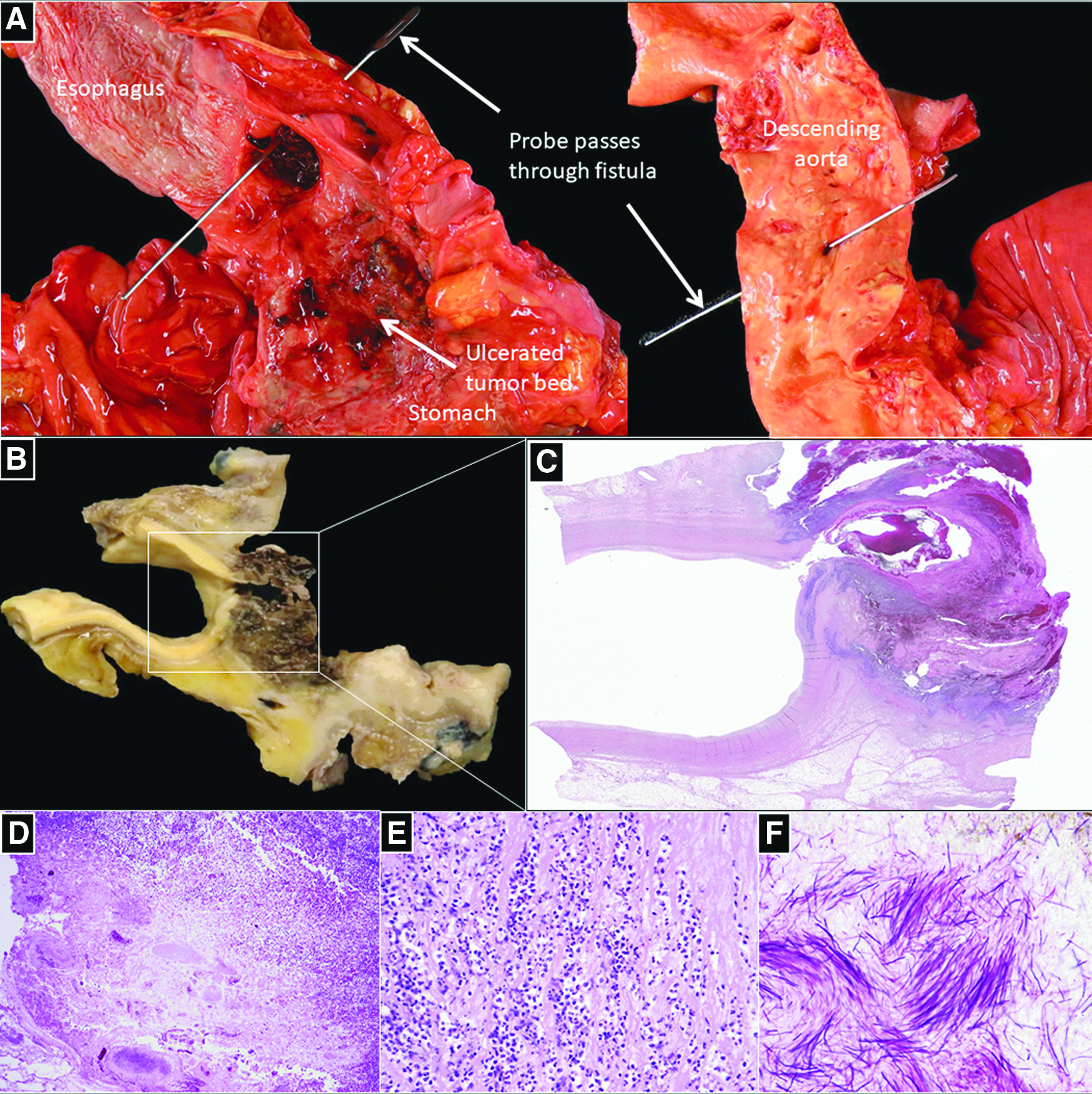
Of the 7 cases related to malignancy, most (6) occurred as a direct treatment effect of esophageal carcinoma. This was a unique group of patients (age range: 30–80 years, median: 71 years) with male predominance (M:F-5:1). The fistula site was most commonly between the esophagus and a variety of sites: aorta (2), inferior vena cava (1), aberrant right subclavian artery (1), coronary sinus (1), and left ventricle (1). The histologic subtype of the esophageal malignancy was adenocarcinoma in most patients (4/6) and squamous cell carcinoma in the rest. The terminal complication generally occurred as a late event after the diagnosis of malignancy (mean interval: 1.7 years), with all patients having locally advanced and/or metastatic disease at diagnosis. All but 1 of the patients received chemotherapy and chest radiation therapy. All patients underwent surgical and/or endoscopic intervention: minimally invasive esophagectomy (3/6) or esophageal stent placement (3/6). The etiology of fistula formation was tumor invasion in most cases (4/6), confirmed by microscopic examination of the fistula site (Fig. 1). The etiology in the other cases was pathologically shown to be fistulizing infection in 1 case and mechanical erosion of a retrograde jejuno-gastric feeding tube in the other. In the latter case, the esophagectomy was complicated by volvulus of the gastric conduit resulting in relative obstruction necessitating placement of a retrograde jejunogastric tube. Of the 3 patients who underwent esophagectomy, the fistula site was at the gastroesophageal anastomosis in 2 of them. There was no significant atherosclerosis (minimal to mild) at the fistula sites in patients with fistulas involving the aorta/carotid/subclavian artery (cases 1, 3, 4, and 7).

Case 4.
The final malignancy-related patient (case 1) had a history of papillary thyroid carcinoma treated with thyroidectomy, radical left neck dissection and radiation therapy that was complicated by tracheo-esophageal fistula (TEF) formation 2 years after initial diagnosis. He subsequently developed invasive squamous cell carcinoma at the TEF with erosion into the internal carotid artery, confirmed by microscopic examination of the fistula site.
Of the 2 patients with enterovascular fistulas not related to malignancy, 1 underwent endograft repair of an ascending aortic aneurysm and aortic root repair for type A dissection 2 years before the terminal presentation with signs and symptoms of graft infection and possible fistula between distal esophagus and aorta. After massive hematemesis he was taken to the operating room and thoracic endovascular aortic repair with salvage esophageal diversion was performed. However, the patient died 3 weeks later as a result of progressive sepsis secondary to graft infection and pneumonia. The second patient developed hematemesis 3 weeks after a pulmonary vein isolation procedure and an atrio-esophageal fistula was confirmed on imaging. This fistula was repaired with evacuation of a left atrial phlegmon. However, postoperative course was complicated by multisystem septic infarcts and septic shock leading to death.
Discussion
Much of our understanding of the etiologies of enterovascular fistulae comes from a large literature review of around 500 cases of AEF reported between 1928 and 1991 by Hollander and Quick. 8 Thoracic aortic aneurysms, foreign body ingestion, and esophageal malignancy accounted for the vast majority (87%) of cases. The most common cause was thoracic aortic aneurysm (51.2%) followed by foreign body ingestion (18.6%) and esophageal malignancy (17.0%). Other causes include surgery-/endoscopy-related reflux esophagitis and infection. In contrast, our study revealed esophageal malignancy (6/9) as the predominant cause of enterovascular fistulae.
In the same study, analysis of AEFs arising secondary to esophageal malignancies between 1963 and 1991 revealed two groups of patients—one where the development of AEF was the first manifestation of esophageal carcinoma and the other where AEF occurred in the setting of treated esophageal carcinoma. This group of patients developing AEF secondary to esophageal cancers was characterized by marked male predominance (10/11) and the classic Chiari's triad of symptoms was identified in none of the patients, similar to that observed in our study. Of the cases that occurred in the setting of treated esophageal cancer, most patients received radiation therapy and the complication occurred weeks to months after the diagnosis of esophageal cancer. In our study, we aimed to look on the treated esophageal cancer patient group.
The complication occurred as a late event (mean interval: 1.7 years) after diagnosis and therapy for esophageal cancer. This is likely due to the current improved neoadjuvant/adjuvant regimens and surgical techniques that have resulted in improved survival in patients with esophageal cancer. Oncologists and surgeons following these patients should be aware of this rare but lethal complication, and recognition of early symptoms should be worked up expeditiously as this can manifest as a late event (years after initial therapy) during routine follow-up. This also highlights the importance of the autopsy in bringing to light historically unusual but perhaps increasingly common complications related to cancer therapy.
Of the 6 patients with esophageal cancer in our study, the fistula occurred between the esophagus and aorta in only 2 cases, with 1 each between the esophagus and a variety of unusual vascular sites such as an aberrant right subclavian artery (1), left ventricle (1), coronary sinus (1), and inferior vena cava (1). The patient (case 4, Fig. 1) with the aberrant right subclavian artery was particularly illustrative with likely a multifactorial mechanism of fistula formation. This patient had advanced esophageal cancer, which was first treated with chemoradiation. He was then taken for surgery where total esophagectomy was performed with the esophagogastric anastomosis done at the left neck. The anomalous vessel's retroesophageal course put it in proximity with the staple line of the esophagogastric anastomosis. The combination of the mechanical erosive effect of the metallic staple along with tumor erosion and radiation-related vessel wall weakness likely resulted in fistula formation. This case underscores two important points. First, every aberrant thoracic vascular anatomy should be identified preoperatively and should guide surgical planning; the identification of an aberrant right subclavian artery has been described to influence the surgical planning of an esophagectomy procedure. 9 Second, the identification of the fistula site at the staple line supports the potential causative role for metallic staples in fistula formation. Moreover, we describe a case of a gastrocaval fistula (case 2) where the fistula site was also identified at the staple line in the setting of esophagogastrectomy, eroding through the more delicate thinner venous wall.
The dominant mechanism of fistula formation in most of the esophageal cancer cases (4/6) was tumor erosion with or without contribution from radiation and/or mechanical staple erosion. Preoperative chemotherapy and radiation therapy before resection of localized esophageal cancer is currently the standard of care and has resulted in significantly improved survival. 7 Of the patents with esophageal cancer in our series, all but 1 patient (5/6) received chest radiation therapy. A healthy aorta is a remarkably strong and durable structure that is resilient to extrinsic destructive processes. It is possible that radiation-induced vessel weakness 10 (in the aorta or the adjacent mediastinal or retroperitoneal vessels in the radiation field) likely plays an important etiologic role in the ultimate development of fistula in patients with esophageal cancer. However, in 1 case (case 3), fistula formation occurred primarily from tumor erosion without a history of radiation.
Of the 2 esophageal cancer cases where the fistula was not secondary to tumor erosion, 1 was an illustrative case (Fig. 2) of a fistulizing Actinomyces sp. infection in a patient who received multiple rounds of chemotherapy and radiation with no surgical intervention. The combination of multifactorial (tumor, chemotherapy, and radiation) ulceration and mucositis along with systemic immunosuppression likely played a key role in the pathogenesis. The other case was also just as instructive and unusual, resulting from mechanical erosion of a retrograde jejunogastric tube from duodenum to left ventricle occurring in the setting of a malrotated gastric conduit leading to functional obstruction.
Case 7.
The limitation of our study is the small number of cases described. This is a reflection of the rarity of this phenomenon, rapid demise from exsanguination before diagnosis or treatment and the fact that autopsy is not done in all patients presenting with this complication. Nevertheless, the cases that were captured in our series are illustrative and well describe the nature of this phenomenon and able to highlight the need for clinician awareness, early diagnosis, and rapid aggressive multimodality salvage treatment, including both endovascular and surgical modern approaches.
Conclusion
Enterovascular fistula formation is a devastating development with an extremely high mortality rate. The increased incidence of esophageal cancer in the population and the advancement of treatments brought to our awareness again this highly morbid complication. Preoperative anatomic variations such as aberrant vascular structures, chemotherapy, and radiation likely increase the risk for enterovascular fistula formation. Once suspected or diagnosed, management with multimodality treatment, which involves endovascular stenting, infection control, and surgical diversion or exclusion, should be done immediately. Despite these measures, the mortality risk stays significant.
Footnotes
Authors' Contributions
Study conception and design: V.S., R.N.M., R.F.P., O.W.; acquisition of data: V.S.; analysis and interpretation of data: V.S., R.N.M., R.F.P., O.W.; drafting of the article: V.S., R.N.M., R.F.P., O.W.; critical revision and final approval of the version to be published: V.S., R.N.M., R.F.P., O.W.
Disclosure Statement
No competing financial interests exist.