
Abstract
Background:
Videoscopic transcervical mediastinal lymphadenectomy has been attempted to reduce thoracotomy-related complications of surgical treatment for esophageal cancer. However, many surgeons would hesitate to attempt this procedure because of the difficulty in understanding the anatomical orientation. In this study, we aimed to create a three-dimensional computer graphic (3D CG) animation and compare it with the real-life operation.
Materials and Methods:
LightWave 3D® version 7 was used as a rendering software to create the 3D CG. The 3D CG images were superimposed to generate an animation using AfterEffects CC®.
Results:
The 3D CG animation for videoscopic transcervical upper mediastinal esophageal dissection was successfully created; it dynamically shows the scene, especially the separation between the esophagus and trachea, and enables surgeons to easily understand the anatomical orientation when using transcervical approach. This 3D CG animation was of high quality and similar to the real-life operation.
Conclusions:
We created a virtual 3D CG animation for the transcervical approach, which will contribute to understanding this procedure for esophageal cancer preoperatively.
Introduction
Videoscopic transcervical upper mediastinal lymph node dissection has been attempted to reduce thoracotomy-related complications of surgical treatment for esophageal cancer.1,2 This novel approach was suggested to be feasible because of its equivalence to the conventional transthoracic approach both in the number of harvested lymph nodes and in the frequency of laryngeal nerve palsy. 3 Recent publications have shown that the technical demands based on the narrow operative field were overcome by introducing single-port endoscopic surgery through a pneumomediastinum 4 or robot-assisted surgery.5,6 However, transcervical endoscopic surgery is still inaccessible for most surgeons because there are few opportunities to use this operative view and it is difficult to understand the clinical mediastinal anatomy from the viewpoint of transcervix.
The area of the upper mediastinum comprises the esophagus and its regional lymph nodes as a target, trachea and bronchus as landmarks, aorta, nerves, and other organs. These organs intersect with overhead crossing in the narrow canal space. In this transcervical approach, the longitudinal anatomy of this region is very complicated, and operators find it difficult to understand compared with the conventional transthoracic approach with a wide side view. Essentially, for advanced and detailed detection of the esophagus in this approach, landmark organs around the esophagus are winding and scattered. Therefore, it is difficult to understand positional change of mediastinal organs in the narrow space only from the surgical atlas or computed tomography images. A virtual three-dimensional (3D) animation in this mediastinal area would be useful to simulate this operation through a transcervical approach.
In this study, we introduced the completed video animation of transcervical upper mediastinal esophageal dissection, including its creation process, and compared the three-dimensional computer graphic (3D CG) animation with the real-life operation.
Materials and Methods
Software
LightWave 3D® version 7 (NewTek, Inc., San Antonio, TX) was used as a rendering software to create the 3D CG, and AfterEffects CC® (Adobe Systems, Inc., San Jose, CA) was to generate the 3D animation.
Design drawing and 3D remodeling
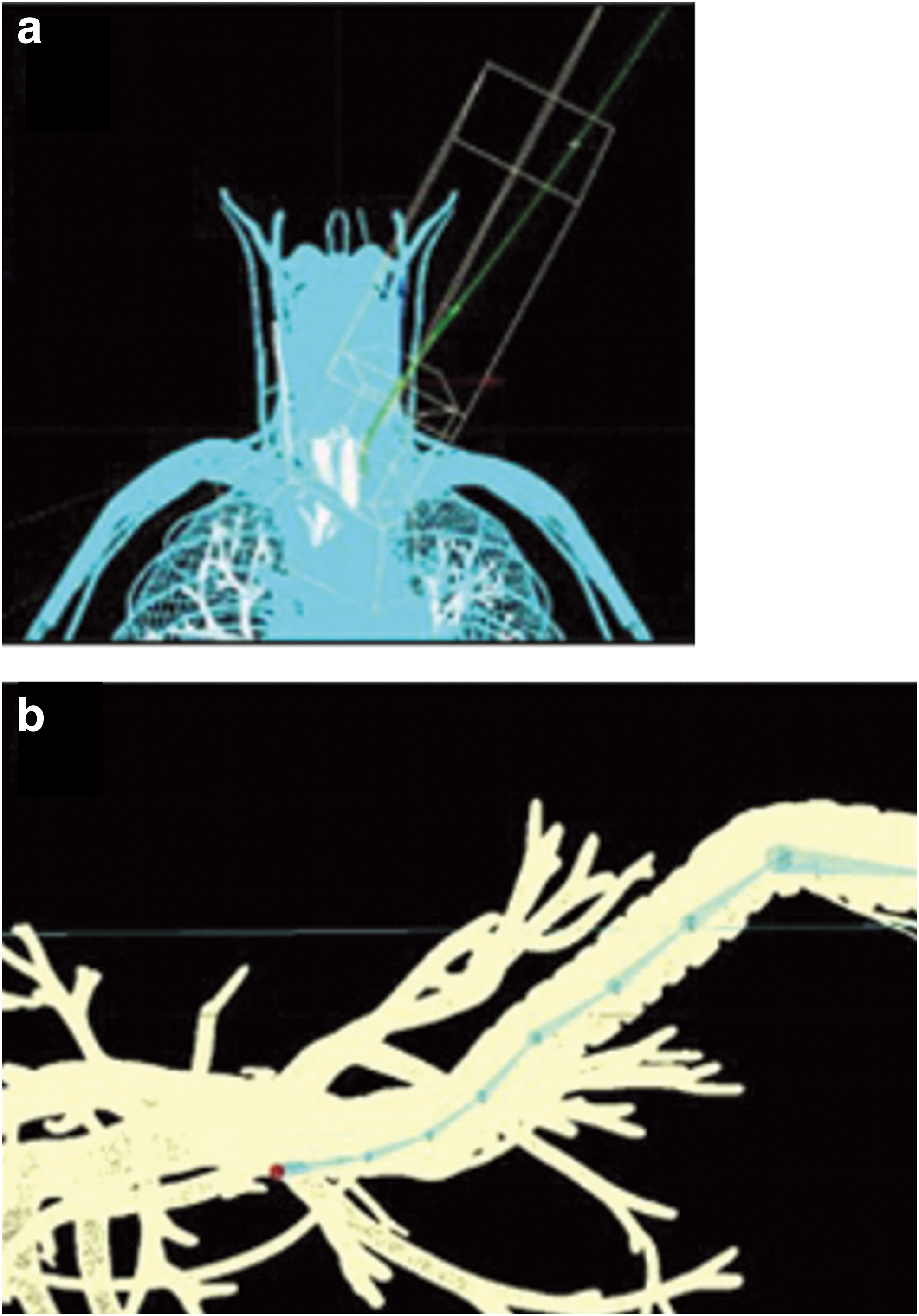
Preparation of accurate images of anatomical structures is one of the important fundamental operations. Using the conventional anatomical chart 7 and surgical atlas, 8 the 3D position of each organ, lymph node distribution, and so on in the mediastinal region were drawn out in the XYZ space. Then, 28 images of this area were made because the accuracy of this stage deeply affects the quality of subsequent 3D CG. Furthermore, 3D CG models were represented using polygon modeling by superimposing these design images9,10 (Fig. 1a, b).

3D remodeling.
Animation
Setting up the track of the endoscope
Using LightWave 3D software, an animation video to film a vertical endoscope entering into the 3D CG model was made similar to that in a real operation, and it was finely adjusted several times to move the endoscope smoothly and to prevent the scope from colliding with virtual organs, especially when it passes through narrow portions with thickset nerves and vascular systems. The final track of the virtual scope was set as shown in Figure 2a.
Setting up the track of the endoscope.
Metamorphosis of the object attendant during dissection
In the real intervention, during deep dissection of the esophagus as a target organ, landmark organs are separated from the esophagus, and the scope camera is passed through them. The manufacture process is very important, as it should naturally represent those metamorphoses, flexions, and positioning changes. Joints were used to make our animation 11 because of its facile adjustment and strict setting. In this method, bones were placed in 3D models, and joints were set between each bone. Then, to wind the models, every joint was set to each desired angle. Figure 2b shows the bones and joints set in bending the trachea. If joints were insufficient, the model did not move smoothly. Moreover, if there were excessive joints, it would be difficult to control the animation. In our model, eight joints were set up in bending the trachea in the animation video. Each angle of every joint was set to use sketches. The displacement mapping effect 12 was ultimately used to represent slight trembling of the trachea in its winding, and this technique used patchy pattern images for the trachea model in the 3D CG.
Division of the esophageal branch of the recurrent nerve
When bending the trachea to separate it from the esophagus, esophageal branches should be divided from the trunk of the recurrent nerve that runs along the trachea. The 3D CG software we used had no simple command of demonstrating the action of cutting objects. After two models, before and after cutting the nerve branch, were prepared, the morphing function, which makes the smooth transformation of the model, that is, before and after cutting the nerve branch, was used to represent the branch to be cut.
Setting of lighting and texture
Lighting and texture of the model were set to greatly control the quality of the completed 3D CG. Texture is composed of some parameters, namely, color, luminosity, diffusion level, specularity, glossiness, reflection, transparency, refraction index, translucency, bump, and so on, and is adjusted several times. Lighting was set based on the degree of illumination from one side until the gradual darkening to the depths, similar to actual images of endoscopic surgery. Then, lighting was set according to the movement of the scope camera.
Results
After operating with the aforementioned settings, all images rendered in the 3D CG were obtained. Images rendered for each model were superimposed using AfterEffects CG, an animation software for image composition, to represent the nerves running behind the left common carotid artery and the left internal jugular vein. Through this process, this software was also used to shade off the neighboring parts of each image and to make fine adjustments of the colors in the animation. All rendering images were about 3500 flames, and the process took about 40 hours, including the rendering test time.
Supplementary Video S1 shows the accomplished 3D CG animation for the endoscopic transcervical upper mediastinal esophageal dissection, which takes 72 seconds. It presents each scene through the track of the scope camera: approach from the left neck (4 seconds from the start), passing on the left side of the trachea (12 seconds), advancing between the esophagus and the posterior wall of the trachea with dissected esophageal branches of the recurrence nerve (61 seconds), and finally to the lymph nodes around the bifurcation of the trachea. The video shows a pause option at each scene when the lymph nodes must be dissected. At 46 seconds from the start of the video, the lymph nodes around the aorta and ligamentum arteriosum, shifting the aortic arch, are shown. By using a synthesizing software input of the 3D positional data in the LightWave 3D software, the annotations are shown to synchronize the movement of the annotational texts to the position of the moving models in the 3D CG.
This 3D CG animation created to perform endoscopic transcervical upper mediastinal esophageal dissection clearly showed high quality of the clinical mediastinal anatomy and was similar to the real-life operation (See Supplementary Video S2).
Discussion
In this study, we created a 3D CG animation, which might be useful to understand the transcervical approach for radical esophagectomy.
Although the endoscopic transcervical approach with radical mediastinal lymph node dissection is one of the promising rational and minimally invasive interventions,1,2 many surgeons would hesitate to attempt this procedure because of the difficulty in understanding the anatomical orientation in this approach through a small left neck incision. The esophagus, trachea, and bronchus; major arteries and veins; nerves; and other organs are located in the upper mediastinum, which is a narrow canal space, and they intersect complicatedly with overhead crossing. In the actual operation, these neighboring organs should be separated without causing any organ injury. Especially, the nearby recurrent nerves, membranous trachea, esophagus, and regional lymph nodes must be dissected at the exact layer. 13 However, the view of this region in the vertical axis from the neck is unfamiliar to many surgeons. Therefore, they find it difficult to imagine operative scenes and how the angles and positions of these objects will be shown on the monitor screen. This factor might be a limitation of the human's ability for space recognition, which varies individually. Using CG, animation images of regions not frequently observed can be created. Seeing images of such regions help enhance space recognition.
With advancement in medical interventions, organs are constantly divaricated in various directions, and the operative field varies. However, it is difficult to predict these unique operative views of the narrow upper mediastinum in the longitudinal direction. Therefore, there is a need to create a more natural and real 3D CG animation video that will be a useful simulation tool for intervention, detailing how each organ will be remolded after dissection or showing which way on the monitor screen the landmark organs are passed through when the scope camera advances more deeply. This operation needs not only graphic engineers but also surgeons who have enough experience with esophageal interventions. The 3D CG video created in this study dynamically shows the scene when the trachea and recurrence nerve are detached and spread toward the farthest part of the screen, by separating the esophagus and the trachea. Furthermore, the color, luster, and reflection of organs are naturally expressed without uncomfortable sensation because of different adjustments for texture and lighting.
With the development of medical technology, many interventions have been changing from open surgeries to endoscopic surgeries, and more rational approaches have been proposed. The next-generation surgeons who received the benefit of endoscopic surgery will be required to have space recognition ability on every operative view, which is difficult to understand when using a conventional anatomical atlas. The 3D CG animation is, of course, different from actual operative video in camera working, tension of tissue, and so on, and in the narrow operative field such as the upper mediastinum, interference of forceps may happen. However, 3D CG animation would help surgeons easily recognize operative anatomy. The presented 3D CG animation video is expected to help surgeons who are planning to perform a new approach because it showed high-quality images of the surgical anatomy and was similar to the real-life operation.
The major limitation of this study is that it did not confirm whether using this 3D CG animation will improve the surgical outcomes. This video only helps with a very small part of this surgery in regard to safety because the safety of the surgery will be dependent on the surgeon's clinical judgment, surgical skill, experience, medical and anatomical knowledge, and ability to manage intraoperative complications. We will investigate the effect of this video clinically.
We succeeded in creating a 3D CG animation of transcervical upper mediastinal esophageal dissection for esophageal cancer, and it showed high quality of the clinical anatomy. This 3D CG animation will contribute to understanding this procedure preoperatively, and it might ensure further intraoperative safety.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.