
Abstract
Abstract
Introduction:
Robot-assisted laparoscopic surgery (RALS) has been increasingly embraced in the fields of adult and pediatric urology, especially in North America and Europe. The advantages of a stable magnified three-dimensional view, tremor filtering, and motion scaling allow for precise intracorporeal exposure and suturing.
Methods:
With this review, we aim to provide the most recent evidence on RALS applied to pediatric urology. We systematically searched the following databases: PubMed and EMBASE. We critically reviewed the available literature on the use of robotic technology in pediatric patients.
Results:
We extrapolated and summarized the most recent evidence on RALS as applied to pyeloplasty, radical and partial nephrectomy, ureteral reimplantation, kidney stones treatment, bladder augmentation, bladder neck reconstruction, Mitrofanoff appendicovesicostomy, and Malone antegrade continence enema.
Conclusion:
RALS is technically feasible for selected pediatric patients and may achieve comparable surgical outcomes compared to the standard of care, but large case series and randomized controlled trials are still needed. We strongly believe that the evolution of robotic platforms will offer an alternative in the treatment of pediatric patients, along with improved care and quality of life.
Introduction
M
With this review, we aim to illustrate the current state of the art of robotic surgery in pediatric urology and to provide an in-depth analysis of the up-to-date available literature.
Pyeloplasty
Ureteropelvic junction obstruction (UPJO) is a common congenital anomaly that is present in ∼1:2000 live births. The majority of cases in the modern era are detected on routine antenatal ultrasound, however, UPJO can less commonly present in older children and adults experiencing abdominal pain, nausea, and emesis. 16 The gold standard intervention for UPJO is the Anderson-Hynes dismembered pyeloplasty, traditionally performed with an open flank approach. Endoscopic options, including endopyelotomy and retrograde balloon dilation, are less invasive, but not routinely used due to suboptimal outcomes relative to pyeloplasty. 17 Laparoscopic pyeloplasty (LP) was first described in 1995 18 and subsequently shown to be a safe and effective minimally invasive treatment option for UPJO. 19 However, conventional laparoscopy has a steep learning curve, which makes it technically challenging for many surgeons. 20 Conversely, the robotic platform enhances the laparoscopic approach by providing several advantages, including high-resolution 3D view and enhanced dexterity. This technology has facilitated a shorter learning curve and acts as a bridge between the open and endoscopic approach. 21 As such, utilization of robot-assisted LP (RALP) has increased steadily since the initial case reports published in 2005.22–24 Since then, RALP has been shown to have very good outcomes. A 2011 article from Minnillo et al. showed a 96% success rate at a median follow-up of 31.7 months. 25 This is the largest single-institution study so far, in which the authors assessed 155 pediatric patients undergoing RALP. A meta-analysis performed by Cundy et al. found no difference in success rate between RALP, LP, and open pyeloplasty (OP). 26 This meta-analysis included 12 observational studies with a total of 384 RALPs, 131 LPs, and 164 OPs. The cumulative success rate among studies was 99.3% for RALP and 96.9% for LP, with no significant difference detected between the two groups. A more recent multicenter study included 407 pediatric patients treated with RALP and found an overall complication rate of 13.8%. The majority of these compilations were low grade Clavien–Dindo (CDG) I or II (8.8%). The remaining complications were grade III, (4.9%) and there were no grade IV or V (high-grade) complications. 27 Given the success of robotic pyeloplasty in the general pediatric population, we started to perform robotic pyeloplasty in infants. Kutikov et al. described a series of 9 infants with a mean age of 5.6 months who were safely and successfully treated with RALP. 28 Subsequent series comparing RALP to OP in infants have demonstrated comparable outcomes with respect to improvement or resolution of hydronephrosis, with either an equivalent 29 or shorter length of hospital stay (LOS) in the RALP cohort. 30 In addition, these studies found no difference between RALP and OP in terms of postoperative complication rates. The largest series to report on RALP in infants is a multicenter retrospective review of 60 infants undergoing RALP, with a mean age of 7.3 months, which reported positive outcomes in 91% of patients. The authors reported postoperative complications in 7 patients (11%), of which 1 CDG I, 2 CDG II, and 4 CDG III. 31
These preliminary data suggest that RALP is safe and effective in children. However, RALP for infants still remains in its early stages and further studies are needed to validate the use of this approach for smaller patients.
Partial Nephrectomy and Nephroureterectomy
Renal benign diseases, such as atrophic kidney, multicystic dysplastic kidney, and renovascular hypertension, often require a nephrectomy which can be easily accomplished with conventional laparoscopy. Robot-assisted nephrectomy or nephro-ureterectomy has been described and reported by some study groups. 32 The robotic approach is clearly feasible, but whether the robot offers a real advantage is still questionable. Nephrectomy and nephroureterectomy do not have any reconstructive part, and there is no high risk of harm to adjacent structures such as in the heminephrectomy. Therefore, the use of the robot for these indications mostly depends on local financial settings and the availability of the robotic system. However, some of these patients may present with multiple malformations of the urinary system, requiring bilateral procedures. The robot has been shown to be extremely helpful when performing multiple surgeries at the same time, such as nephrectomy with contralateral ureteral reimplantation, without the need to redock the system or place additional ports. 33 Bansal et al. reported a series of 24 robotic nephroureterectomies, with an 8.3% complication rate (urinary retention and a urine leak at the ureteral stump, both managed conservatively). The port placement for these combined retroperitoneal and pelvic procedures was similar to pyeloplasty, except for the assistant port, which was placed between the camera and inferior working port. 32
Compared with pyeloplasty, partial nephrectomy does not have a reconstructive phase. However, given the wide degrees of freedom of the instruments, motions scaling, and 3D view, the robot provides greater advantages than laparoscopy. 34 With an estimated 4%–5% of vascular accidents of the healthy moiety during the procedure, the enhanced dexterity provided by the robot helps reducing this number. 35 Herz et al. reported preliminary data confirming the lower rates of vascular accidents. In addition, the authors described selective arterial mapping with indocyanine green in an effort to avoid harm to the healthy moiety. 36 Lee et al. showed the safety and feasibility of robotic partial nephrectomy in 9 patients, 1 of which required percutaneous drainage of an asymptomatic urinoma. All patients had a normal vascularization of the remaining renal moiety confirmed on postoperative Doppler ultrasound. 37 Similar results have been shown by Mason et al., who reviewed 21 patients undergoing robotic partial nephrectomy. The authors found a higher rate (29%) of asymptomatic postoperative fluid collection, which were managed conservatively. Of note, fluid collection rate was higher (42%) when the renal defect was not closed, compared with the 11% rate when the defect was closed, suggesting that reconstruction, in which the robot can play a critical role, might be considered. 38
Ureteral Reimplantation
The ideal management of vesicoureteral reflux (VUR) is to protect the upper urinary tract in patients who fail conservative measures. In an effort to reduce morbidity, treatment options, which are less invasive than the standard open ureteral reimplantation, have been developed. As a consequence, the total number of surgical procedures has dropped during the last decade. Recently, with the advent of robot-assisted laparoscopic ureteral reimplantation (RALUR), the surgical approach has been revisited, leading to a latest increase in utilization. RALUR is usually performed through a transperitoneal, extravesical approach, mimicking the Lich-Grégoire procedure. This technique offers several advantages, such as decreased postoperative narcotic pain requirements and shorter length of stay. Since RALUR was first described by Peters in 2004, 39 an increasing number of extravesical cases have been reported. To optimize the outcomes, Gundeti et al. described RALUR technique modifications, 40 named by the acronym LUAA, which represents the length of the detrusor tunnel (L), the use of a U stitch (U), the placement of permanent ureteral alignment suture (A), and the inclusion of ureteral adventitia (A) in detrusorraphy. Other techniques have also been introduced to maximize surgical outcomes. Silay et al. described a modified “top-down” suturing technique using interrupted sutures without the need for ureteral elevation or stent placement. 41
A review by Savio and Nguyen showed that the overall surgical success rate of open ureteral reimplantation exceeded 95%. 42 Therefore, as a surgical treatment option for VUR, the open approach remains the gold standard. Conversely, a review by Baek and Koh showed VUR resolution rates after RALUR ranging between 77% and 100%. 43 This variability in success rates may be attributed to case selection and surgeon's learning curve. The major complications after RALUR were found to be urinary retention and ureteral injury due to obstruction or leakage—urinary retention being the most common one. Although some authors reported that the incidence of urinary retention varied between 0% and 12%,40,44 a more recent multi-institutional study showed a 3.9% rate of transient urinary retention after bilateral reimplantation. 45 Some authors believed that a pelvic neural plexus injury could be the cause of this event. A multi-institutional study of complications after pediatric RALS revealed that RALUR procedures had a relatively high complications rate (30.6%). 27 However, a recent study from Srinivasan et al. found no difference in complication rates between unilateral and bilateral RALURs. 46 In addition, a recent multicenter study found low complication rates, comparable to those after open surgery. 47 Although it remains unclear whether the robotic approach reduces the morbidity associated with a ureteral reimplantation, there is evidence that RALUR is associated with a shorter hospital stay and reduced need for narcotic pain medications.47–50 Further studies are needed to identify specific patient populations that experience the greatest benefit of RALUR over alternative approaches.
Kidney Stone Surgery
The wide availability and efficacy of endourological techniques have largely replaced open surgery for the treatment of renal stones. Recently, with the widespread of robotic surgery in urology, the principle of open renal surgery is being revisited. In selected cases, robot-assisted pyelolithomy may be an excellent alternative to percutaneous nephrolithomy. This minimally invasive approach is ideally suited for concomitant renal reconstructive procedures as well as primary treatment of various renal and ureteral stones in patients with complex anatomy. This is best suited for large renal pelvic stones, partial staghorn stones, or complete staghorn stones. 51 Unfortunately, strong evidence on the utility of robotic surgery for the treatment of renal stones is only available for the adult patient. Data on pediatric population are still scarce. The treatment of large stones in children is difficult and often requires multiple procedures using a combination of therapies. As in adults, children and adolescents with large stone burdens may be treated with extracorporeal shock wave lithotripsy (ESWL) or percutaneous nephrolithotomy (PCNL). Both these methods have high rates of success. However, multiple ESWL and PCNL sessions may be required to achieve stone clearance. In addition, the management of cystine stones is complex, ESWL clearance rates are poor, and its use is not recommended in children with stones greater than 25 mm. 52 Cystinuria, a rare autosomal recessive disease, can often determine complex cystine renal calculi, leading to important complications such as urinary obstruction, urinary infections, and impaired kidney function. The management of these patients usually requires PCNL followed by ESWL. However, Meggiato et al. showed that the combination of robot-assisted laparoscopic pyelolithotomy and intraoperative renoscopy was successful in the achievement of immediate stone clearance, also for complex renal stones. 53 This combined technique could be indicated to minimize intraoperative bleeding. Furthermore, it can be useful in pediatric cases with low ureteral compliance. A multi-institutional study by Swearingen et al. reported results on 27 patients undergoing robotic pyelolithotomy and nephrolithotomy, describing these two techniques as safe and reasonable options for selected patients, potentially allowing for reduced bleeding and parenchymal damage. 54
The small evidence available in literature demonstrates that the robot-assisted kidney stone surgery can be beneficial for the treatment of selected children with large stone burdens. However, further studies comparing the robot with other minimally invasive procedures are needed to validate its role in stone management.
Mitrofanoff Appendicovesicostomy
Mitrofanoff was the first to describe the principle of using the appendix as a continent cathetarizable channel in patients with neurogenic bladder. 55 Traditionally, Mitrofanoff appendicovesicostomy (APV) was accomplished with an open surgical approach, and to date it remains the most performed technique on these patients.
As discussed above, RALS has shown to be safe and effective in infants and toddlers.26,29 Therefore, many pediatric surgeons and urologists are following the trend with increasing comfort and are now performing more complex procedures, including reconstructive surgery of the upper and lower urinary tracts. 56 Pedraza et al. were among the first to describe their successful experience with robot-assisted laparoscopic Mitrofanoff appendicovesicostomy (RALMA) in a 7-year-old boy, born with posterior urethral valves. 57 The authors performed the procedure in 6 hours, with an estimated blood loss (EBL) of 10 mL and no intraoperative complications. Subsequently, Storm et al. published the first case series of RALMA reporting successful outcomes. 58 The mean operative time (OT), EBL, and LOS were 301 minutes, 50 mL, and 3 days, respectively. Nguyen et al. 56 published another case series of successful RALMA reporting similar peri- and postoperative outcomes. At 6 months follow-up, only 1 patient out of 10 (10%) developed a stomal leak and required surgical revision. Accordingly, Famakinwa et al. reported good outcomes in 18 patients undergoing RALMA. 59 At a median follow-up of 24 months, 17 patients (94%) were continent. The overall rate of complications was 17%, with 2 stomal stenosis and 1 parastomal hernia. A more recent study by Gundeti et al., 60 including multiple institutions, evaluated perioperative and functional outcomes of 88 patients undergoing RALMA. Perioperative data were comparable to the previously described studies. In addition, the authors calculated the morphine equivalent usage as a surrogate of postoperative pain, showing low use of this narcotic (0.7 mg/kg/day). Postoperative complications occurred in 26 patients (29.5%), of which 11 (12.5%) required surgical revision. Overall, 75 patients (85%) were continent at a median follow-up of 29.5 months.
In contemporary open series on Mitrofanoff, functional outcomes appeared comparable to RALMA, with revision rates ranging from 9% to 32%, 61 and long-term stomal continence, stomal stenosis, and stomal revision rates being 91%–98%, 8%–10%, and 16%–24%, respectively.62–64 McNamara et al. queried the 2012 and 2013 American College of Surgeons National Surgical Quality Improvement Program Pediatric database (ACS-NSQIPP) for all patients undergoing augmentation enterocystoplasty and/or appendicovesicostomy. In the open series, mean OT and LOS were 240 minutes and 6 days, respectively. 65 Grimsby et al., in a retrospective comparative study between open and robot-assisted Mitrofanoff, found no difference in postoperative complications, at a follow-up of 31 months. A subset analysis of the reoperated patients revealed an interesting difference between the two cohorts: surgical revisions in the robotic group were mostly required for stomal incontinence, while the open group had higher incidence of stomal prolapse and stenosis. 66
The results provided by the above-mentioned studies showed that RALMA is a safe and effective approach. In addition, it offers the intrinsic advantages of MIS (decreased postoperative pain, LOS, and better cosmesis) with comparable perioperative and functional outcomes. However, the benefits of RALMA have to be weighed against longer OT and higher costs.
Bladder Augmentation
Bladder augmentation is indicated in the management of patients with impaired bladder function secondary to neurogenic bladder or, less frequently, to non-neurogenic voiding dysfunctions, posterior urethral valves, Prune-Belly syndrome, and bladder exstrophy complex. Traditionally, this procedure was accomplished with an open approach, which is still considered the gold standard. As every major procedure, open augmentation ileocystoplasty (OAI) is characterized by long LOS and high rates of postoperative complications. In the available literature on OAI, LOS ranges between 9 and 14 days, and almost 15% of patients had a prolonged postoperative course due to ileus or urinary leak.67,68 Flood at al. 67 and Schlomer et al. 68 performed two of the biggest dataset analyses on long-term follow-up of patients undergoing OAI. In these two studies, the 3-year cumulative risk of bladder rupture, bladder stone, pyelonephritis, and small bowel obstruction ranged between 3.5% and 4%, 10.9% and 21%, 11% and 26%, and 4% and 6%, respectively.
As discussed in the previous paragraphs, pediatric surgeons and urologists have started to push the envelope by using the assistance of the robot, even for more complex and technically challenging procedures, such as reconstructive surgery of the bladder. Early in 2008, Gundeti et al. reported their first successful robot-assisted laparoscopic augmentation ileocystoplasty (RALI) and APV. 69 Murthy et al., in a large series published in 2015, compared RALI to the conventional OAI. The authors reported significantly longer OT and shorter LOS for the RALI cohort. The mean EBL, bladder capacity increase ratio, and narcotic use did not differ between the two groups. With a similar median follow-up, bladder stone formation and complication rates between RALI and OAI were similar. 70
Despite the high complications rate, OAI has proved to be a safe approach and remains the gold standard in these patients. However, RALI not only offers cosmetic advantages but also results in shorter LOS and decreased postoperative pain. Nonetheless, the complexity of this technique has limited the widespread adoption of the robotic approach.
Bladder Neck Reconstruction
Bladder neck reconstruction (BNR) is usually performed in patients with urodynamically defined incompetent urethral sphincter. The most common subset of patients requiring these complex and technically challenging procedure are those with neurogenic bladder secondary to congenital neural tube defects or spinal cord injury, epispadias-exstrophy complex, and cloacal abnormality. BNR is often accomplished along with an APV and, traditionally, an open surgical approach was considered the gold standard.
In 2011, Gargollo published their first experience with robot-assisted BNR. In their article, the authors described the management of neurogenic bladder with persistent urinary incontinence, unresponsive to clean intermittent self-catheterization, and anticholinergic medications. The technique adopted by the authors included creation of a Mitrofanoff APV and a Leadbetter/Michell (LM) BNR along with bladder neck sling (BNS). 71 Four years later, the same study group reported outcomes of 38 patients with a mean follow-up of 21 months. The authors found an overall continence rate of 82%. Two patients developed reflux (one grade 2 and one grade 3), and two developed bladder stones. 72 A direct comparison of these results with previously published open reports was not feasible due to data inconsistency: patient selection and characteristics, definition of success/failure, and associated procedures (BNS, enterocystoplasty, etc.).
Recently, Grimsby et al. published a retrospective study comparing perioperative and postoperative short-term outcomes between robotic and open BNR. The authors reported longer OT in the robotic cohort. However, they also found that with increasing experience the mean OT declined significantly. Overall, there was no difference in LOS, 30-day complications rate, and need for further surgery aimed at treating incontinence between the two groups. 73
BNR is a technically challenging procedure, and very few reports are available in literature. From the few available data, we can speculate that the robotic approach appears to be safe, offers unique advantages, and has comparable outcomes as compared to the open approach. However, there is still the need for further studies to establish a role for robotic surgery in the treatment of these patients.
Malone Antegrade Continence Enema
Malone antegrade continence enema (MACE) or appendicocecostomy (APC) is often performed in patients with congenital neural tube defects or acquired spinal cord injury for intractable constipation and/or fecal incontinence. An open approach is the gold standard and this procedure is often associated with a Mitrofanoff APV. There have only been a few reports in the literature, in which laparoscopic-assisted technique has been described for such reconstruction. However, intracorporeal suturing is a technically demanding task that requires a significant amount of experience and skills. The robotic system has the potential to overcome these limitations, allowing to perform such complex procedures in a minimally invasive manner. Thakre et al. and Lendvay et al. published their initial experiences with robotic combined Mitrofanoff and MACE.74,75 Lendvay et al. reported the use of a pure laparoscopic technique for the initial colonic and appendiceal mobilization, with an overall OT of 8 hours. 74 Thakre et al., instead, performed the entire procedure robotically, with an OT of 3 hours and 20 minutes. 75 Both studies reported no stomal incontinence or channel revision within the first year of follow-up. Zee et al. reported their successful experience of robot-assisted laparoscopic MACE with imbrication of the cecum over the channel, thereby improving continence and decreasing the risk of perforation. 76
Based on the available data, we can only conclude that robotic surgery for MACE is a safe approach if performed by experienced surgeons and has good short-term outcomes. However, evidence in literature is scarce and there is no long-term follow-up data.
Conclusion
In this review, we discussed the current status of robotic surgery applied to pediatric urology. The widespread of minimally invasive techniques has provided patients with faster recovery and reduced postoperative pain. However, conventional MIS, such as laparoscopy, has several limitations (steep learning curve, fulcrum effect, limited range of motion, etc.). The robotic platform, with its motion scaling, magnified 3D view, increased dexterity, and degree of freedom has enabled these limitations to be overcome. Robotic procedures are becoming increasingly common, as there is growing evidence that functional outcomes are comparable to the open approach. However, a few challenges have still to be solved before robotic surgery can be considered the gold standard: lack of haptic feedback; need for smaller instruments to facilitate the approach of infants and newborns; need for randomized controlled trials to validate the outcomes; need for standardized training to gain and maintain competency; and excessive costs of the current available platforms (Fig. 1). Shortly, new players (Cambridge medical robotic, Medtronic, Alphabet, and more) will come into the market offering further developments at a relatively lower price. 77 They will likely focus on specific features of robotic arms, instruments, console, and 3D video technology. The evolution of robotic technology will never stop, and we believe that the development of new platforms will offer alternative managements in treating pediatric patients, achieving improved care and quality of life.
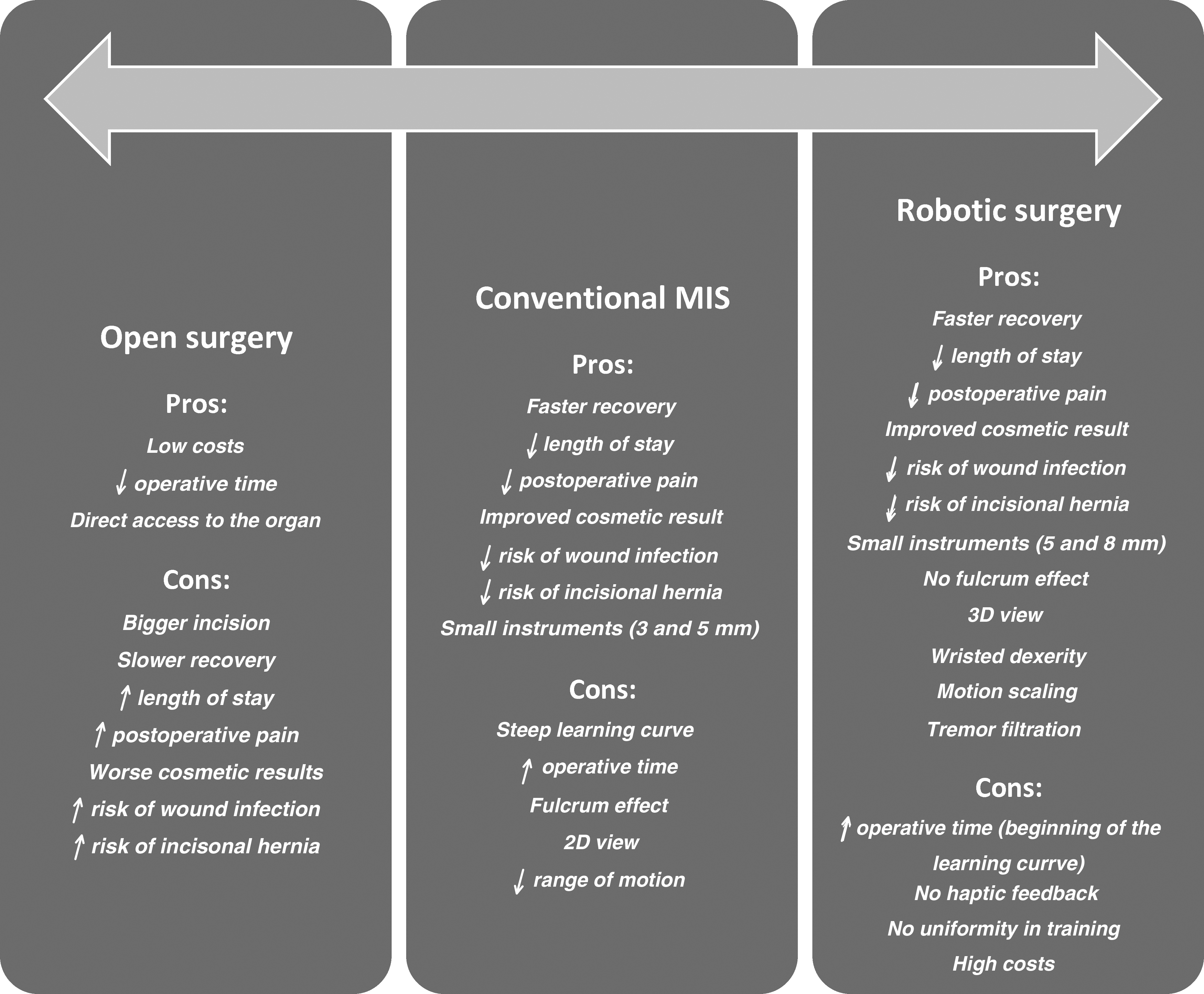
Diagram showing the evolution of advantages and disadvantages in surgery from an open to a robotic approach.
Footnotes
Authors' Contributions
Design of the work: C.A. and M.S.G.; Drafting the work and revising it critically: C.A., R.K., W.R.B., and M.S.G.; Final approval: C.A., R.K., W.R.B., and M.S.G. All authors agree to all aspects of the work.
Disclosure Statement
Dr. M.S.G. is codirector for the NARUS course. The other authors have no conflicts of interest to declare.