
Abstract
Abstract
Background:
Modifications to conventional laparoscopic cholecystectomy (LC) aim to reduce trauma to the abdominal wall and improve cosmetic outcomes. Although single-incision laparoscopic surgery (SILS) provides excellent cosmetic results, the procedure is technically demanding. Herein, we describe the LIFT technique (“Less Incisions but Four Trocars”), with four trocars but only one 3-mm visible incision, using conventional instruments.
Methods:
Retrospective study with the LIFT technique for cholecystectomy during 2017. Access to the abdomen is obtained with two trocars (11 and 5 mm) through the same intraumbilical skin incision, and two extraumbilical 3-mm trocars for a correct triangulation (one of them concealed below the bikini line). The results are compared with a series of patients operated on with LC by the same surgical team during 2016.
Results:
During the study period, 90 procedures were performed. Both techniques showed similar results in terms of surgical time, conversion rate, complications, and hospital length of stay. The patients operated on with the LIFT technique reported better cosmetic evaluation and less postoperative pain at 3 months compared with LC.
Conclusion:
The LIFT technique is a safe and feasible alternative for cholecystectomy that can provide a significant improvement from the cosmetical point of view, mostly for those patients who are especially concerned with their body image.
Introduction
Halfway between laparoscopic cholecystectomy (LC) and single incision laparoscopic cholecystectomy (SILC), Nguyen et al. 1 defined the concept of “strategic laparoscopic surgery” as an alternative to improve the cosmetic results of classical laparoscopic surgery, maintaining its same level of security. In the field of biliary pathology, numerous studies on strategic laparoscopic cholecystectomy (SLC) have recently been published that try to solve some technical problems of SILC, such as traction on the gallbladder fundus, triangulation, or collision between instruments, by the use of additional trocars, extracorporeal sutures, and specifically designed devices.2–8
Herein, we present the description and preliminary results of the “LIFT” technique (Less Incisions but Four Trocars) for LC, a proposal for SLC to optimize the cosmesis (two 3-mm incisions, one visible and one concealed with the underwear) but preserving the fundamental LC principles of triangulation, visualization, and ergonomics. Unlike other SLC techniques, the LIFT procedure is performed with four trocars and conventional instruments, which in our opinion make it a safe, feasible, and efficient option. In addition, we show a comparative analysis with a historical series of patients following a standard four-trocars LC by the same surgical team.
Materials and Methods
Patients
After approval by the Al-Takhassusi Hospital Institutional Review Board, we have retrospectively analyzed a series of 45 patients operated on for cholecystectomy using the LIFT technique at Al-Takhassusi General Hospital, Sulaiman Al Habib Medical Group (Riyadh, Saudi Arabia) during 2017. Also, the series has been compared with 45 patients operated on using LC technique by the same surgical team during 2016. Patients with a history of midline laparotomy, morbid obesity (BMI >40), anesthetic risk with ASA≥IV, acute cholecystitis, acute pancreatitis, and/or recent lithiasic obstructive jaundice (less than 6 weeks) were excluded from the study.
Surgical technique
All the patients of both groups were operated under general anesthesia. A nasogastric tube was inserted when necessary for reducing gastric distention, and single-dose of broad spectrum antibiotic was administered at induction in all. Patients were placed in a split-leg position, with 30° head-up and 20° right side-up position. The monitor was placed above the right shoulder of the patient. The surgeon stood between the patient's legs and the assistant was located on the patient's left.
LIFT technique
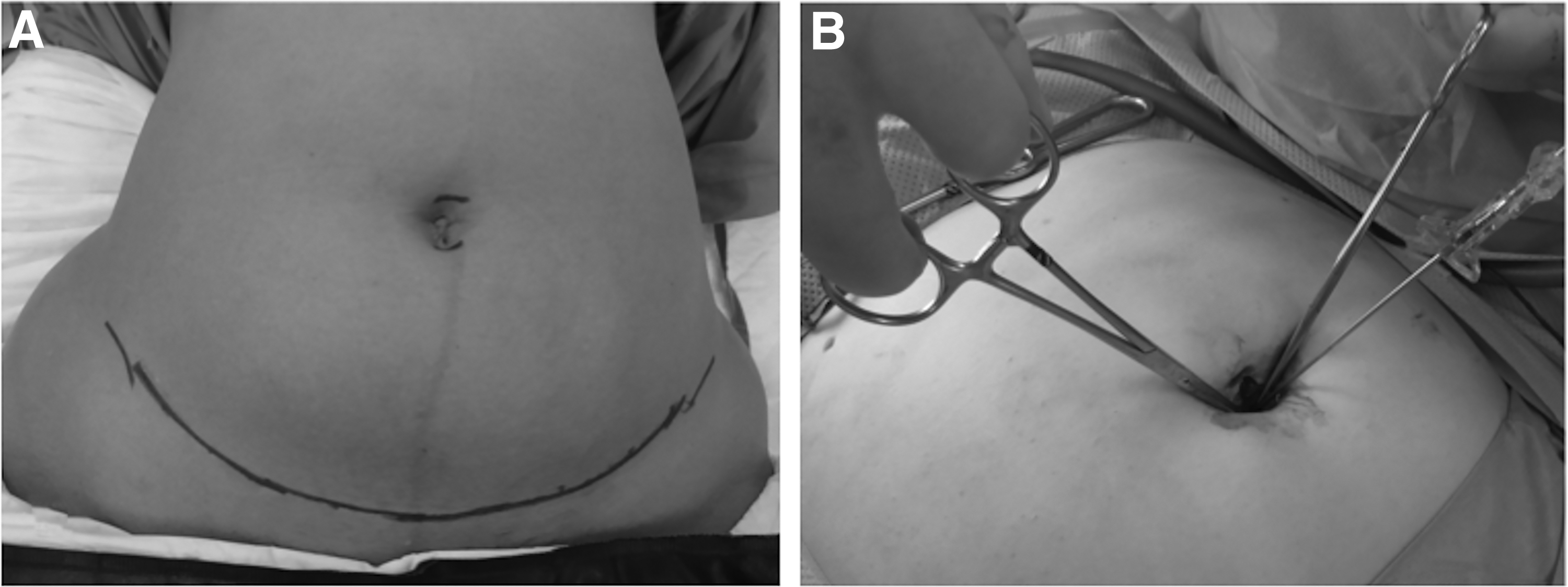
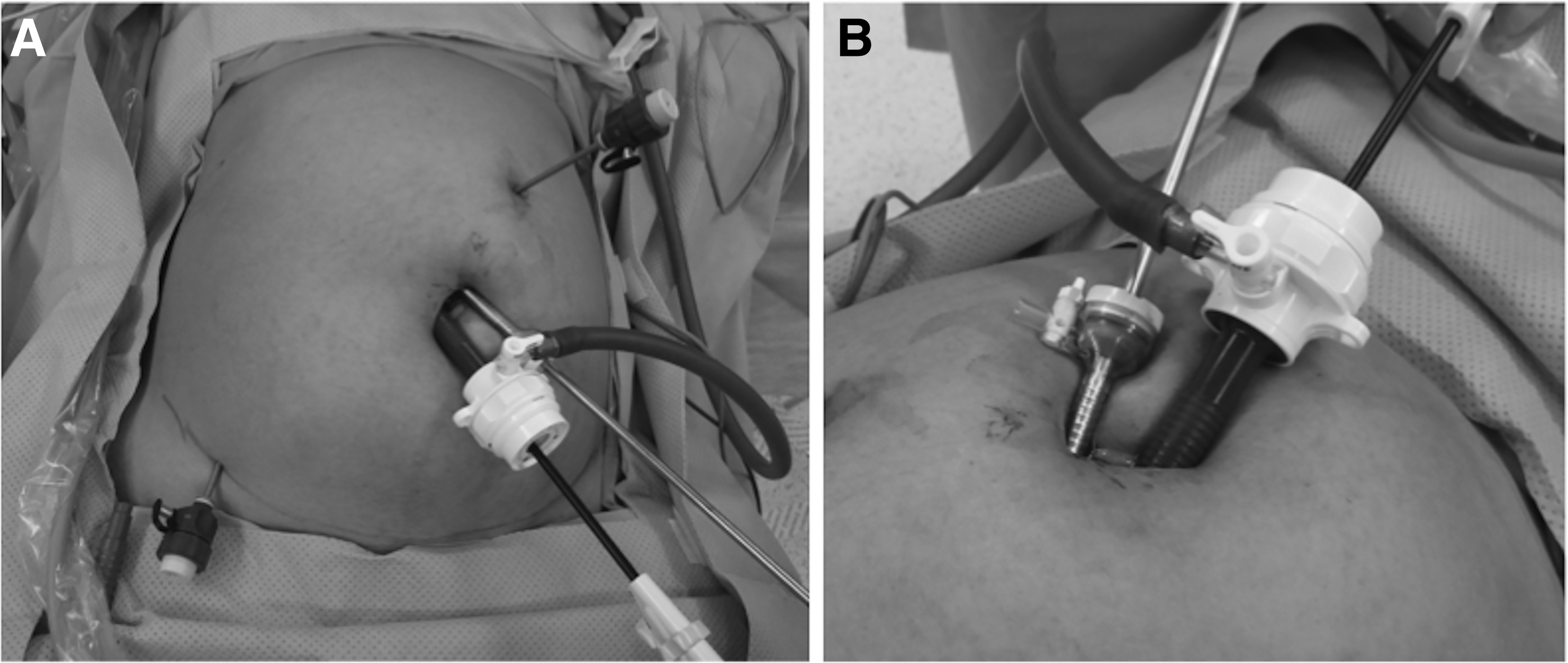
First, the superior and inferior margins of the umbilical flange are marked to delimitate a completely intraumbilical skin incision, aimed to achieve the best possible cosmetic result. Also, the “bikini” line is delineated, usually connecting both anterosuperior iliac crests.Then, two Kocher forceps are placed on both sides of the midline to evert the umbilicus, the skin and subcutaneous tissue are incised vertically with cold scalpel, deepening until reaching the fascia at the level of the umbilical stalk, and a Veress needle is inserted for the pneumoperitoneum (Fig. 1). A first 11-mm trocar is placed in the midline, and then a 5-mm optical trocar (VersaOne™; Covidien™, Mansfield, MA) is inserted about 2 cm to the right of the previous one (patient's left), by the same skin incision but through the left anterior rectus muscle. The fascial trajectory for this trocar is slightly angled laterally from the respective cutaneous entry, to reduce the intracorporeal “swordfighting” of the instruments. Now, two 3-mm trocars for the surgeon's hands are placed with a proper triangulation in both flanks of the patient. According to the patient's anatomy, the 3-mm trocar for the surgeon's left hand is placed as low as posible toward de “bikini line,” close to the patient's right anterosuperior iliac crest, so that the future scar will remain concealed by the underwear, or at least as far as possible from the most visible part of the abdomen (Fig. 2).
In the LIFT technique, conventional instruments are used. A 5 mm-30° laparoscope is inserted through the optical trocar, and a grasping forceps (EndoClinch™ II, Auto Suture™, Mansfield, MA) passed through the 11-mm trocar is used for grabbing the fundus of the gallbladder. After dissecting the cystic elements, the assistant pulls the gallbladder fundus with a clamp inserted through the left 3-mm trocar, freeing the 11-mm one to introduce the 10-mm clip applier. Once the cystic elements are sectioned, a standard cholecystectomy is performed, and a bag is used to extract the specimen (EndoCatch™ Gold, Covidien™, Mansfield, MA). We only closed the 11-mm fascial hole, with several interrupted stitches of reabsorbable material. The skin in all wounds is closed with subcuticular reabsorbable stitches (monocryl 4/0).
LC technique
We perform a conventional four-trocars LC. First, a 11-mm trocar is placed just below the inferior rim of the umbilicus, another 5-mm trocar in the epigastrium and the other two 5-mm trocars are placed in both flanks. A 5 mm-30° laparoscope, inserted through the subumbilical trocar, is temporarily shifted to the left trocar to free the umbilical one so that a 10-mm clip applier can be introduced for the clipping of cystic structures. The closure of the fascia in the umbilicus and the skin is similar to the LIFT technique.
Variables and statistical analysis
The following variables have been included for each patient: age, gender, body mass index (BMI), indication for cholecystectomy, anesthetic risk (ASA), previous surgeries, operative time, intraoperative events (perforation of the gallbladder, bleeding of the cystic artery, bleeding at the trocar site, and conversion), extension of umbilical incision, level of immediate postoperative pain at 1 week and 3 months (VAS scale), hospital stay, complications at the umbilical wound (seroma, infection), and level of satisfaction regarding the cosmesis of abdominal scars at 3 months (1 = very unsatisfied, 2 = not concerned, 3 = acceptable, 4 = very satisfied).
The data were analyzed using SPSS v20.0 (IBM Co. Armonk, NY). Descriptive statistics is presented as number (percentage) for qualitative variables, and median (interquartile range) for quantitative variables. Differences between the groups were analyzed by means of the χ 2 square test (or the Fisher test when appropriate) for qualitative variables, and with the Mann–Whitney test for the quantitative variables. A value of P < .05 was considered significant.
Results
The indication for surgery was symptomatic cholelithiasis (biliary colic or dyspepsia) in about 90% of the cases, and the rest were operated on for various reasons (previous lithiasic pancreatitis, intravesicular polyps, vesicular adenomyomatosis, and beta-thalassemia). The most frequent previous surgery was vertical gastrectomy (six cases in the LC group and five in the LIFT group), and the remaining consisted of three laparoscopic appendectomies, two caesarean sections (Pfannennstiel), one open appendectomy, one laparoscopic tubal ligation, one umbilical hernioplasty, and one laparoscopic splenectomy. Demographic characteristics of both groups were similar (Table 1).
Demographic Characteristics of Patients
The data are expressed as number (percentage), except * median (interquartile range).
BMI, body mass index; ASA, American Society of Anesthesiologists; LC, laparoscopic cholecystectomy.
There was no conversion or modification of the technique. In patients with a history of vertical gastrectomy, the working trocars were placed in the old scars as long as the triangulation was not affected. In most cases it was necessary to extend the 11-mm umbilical trocar incision in the fascia for the extraction of the gallbladder. There was no mortality or serious complications, and all patients were discharged within 24 hours after surgery.
The only case of umbilical infection was treated with oral antibiotics, partial reopening of the wound, and removal of two loose fascial closure stitches that acted as a foreign body, maintaining the suppuration 2 months after the intervention. With the LIFT technique, patients reported less pain at 3 months and a better assessment from the cosmetic point of view, compared to LC. The rest of the variables analyzed were similar in both groups (Table 2).
Operative Details, Complications, and Follow-Up
Bold values indicate comparisons with statistical significant differences at p < .05.
The data are expressed as number (percentage), except * median (interquartile range).
LIFT, “Less Incisions but Four Trocars”; VAS, visual analogic scale.
Discussion
Since its first description in 1985 by Mühe, 9 LC has gained wide acceptance compared to open cholecystectomy. The transition from open surgery to LC has resulted in significant physiological and clinical benefits, however, there has been much less progress from LC to SILC, only to include improved cosmesis and perhaps less postoperative pain. SILC has been considered as the connection between conventional multi-port laparoscopic surgery and surgery through natural orifices (NOTES), becoming prevalent over the latter by not transgressing any viscera. 10 In recent years, numerous SILC modifications have proliferated, but for various reasons this has not been widely accepted. 3 First, SILC requires a large umbilical incision that can cause seroma, infections, skin necrosis, and hernias.11,12 In a recent meta-analysis with 3051 patients, Haueter et al. 13 found that SILC was associated with better cosmetic results but with a risk of incisional hernia four times greater than LC. Second, the SILC involves an inherent difficulty for retraction and triangulation, which hinders the visualization of Calot's triangle and questions its safety. 14 In 2017, Evers et al. 15 published a meta-analysis that showed more adverse events with SILC compared to LC. These technical difficulties make it a difficult procedure to standardize and with a long learning curve, which would explain a conversion rate of up to 24% in some series. 16 Another criticism of SILC is its higher cost, which decreases its efficiency compared to LC.3,17
In 2008, Nguyen et al. 18 defined the concept of “strategic laparoscopic surgery” as a way to obtain the benefits of SILC in a safe and reproducible way, and that may constitute a new stage in the evolution of minimally invasive surgery (Fig. 3). The previous experience of our group at SILC19,20 facilitated the development of an SLC procedure as cosmetic as possible, largely conditioned by a unique work environment (Saudi Arabia) in which several factors converge, such as the demand for better cosmetic results by a very demanding population, a not entirely predictable medicolegal liability and a comprehensive cost evaluation within a private health care system. Thus, the search for a procedure that did not admit the least criticism from the standpoint of safety led us to develop the LIFT technique, in which we use four trocars and conventional instruments in a systematic way to make it safe, 21 feasible, and efficient, which in our opinion lacks the limitations of other SLC,1–8,22 as discussed below (Table 3).
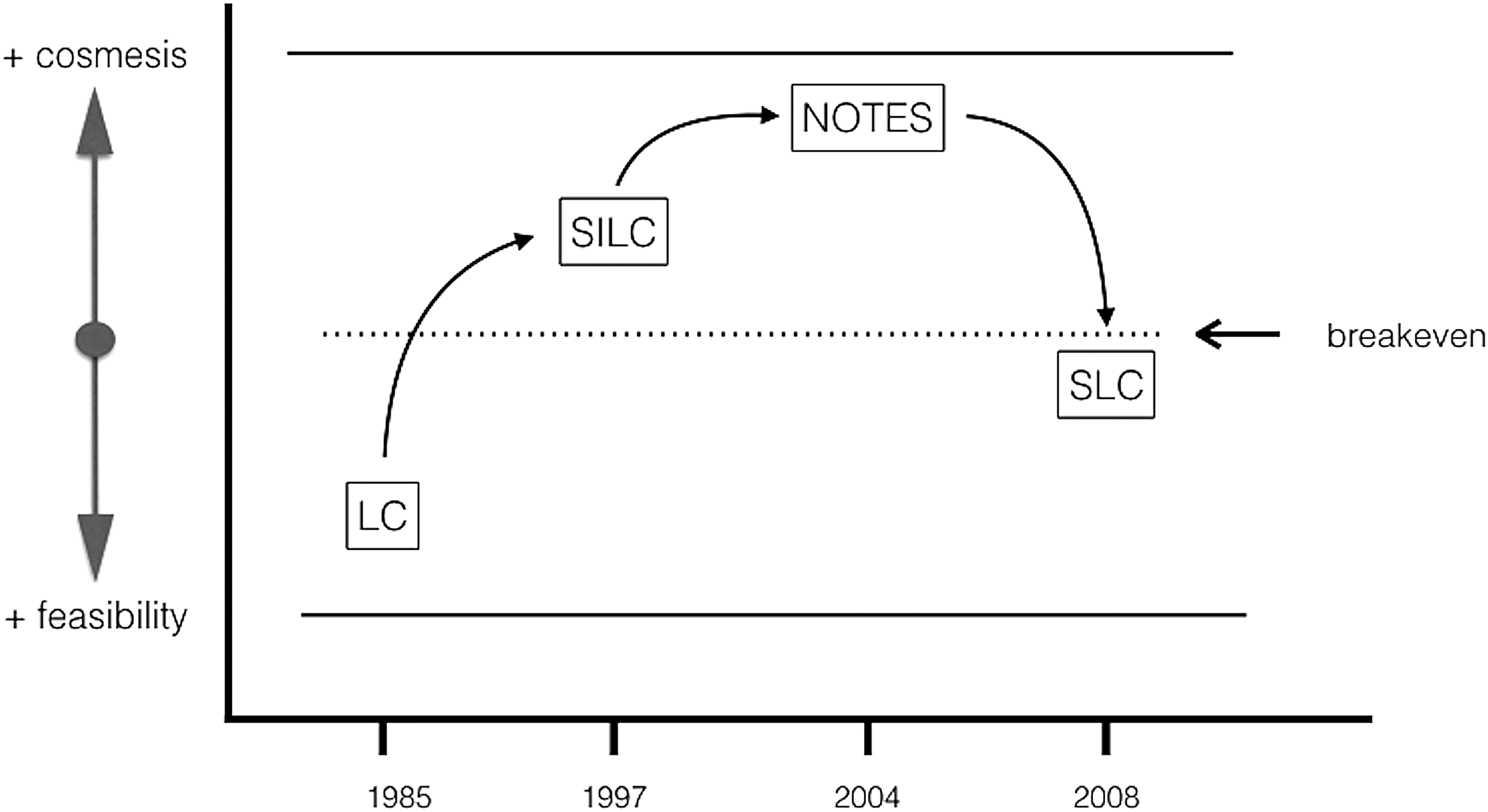
Evolution of minimally invasive surgery from LC to SLC, with its feasibility and cosmetic components, over time. SLC prioritizes feasibility over cosmesis. LC, laparoscopic cholecystectomy (conventional); NOTES, natural orifice translumenal endoscopic surgery; SILC, single-incision laparoscopic cholecystectomy; SLC, strategic laparoscopic cholecystectomy..
Technical Requirements and Limitations in Various Strategic Laparoscopic Cholecystectomy Series, Compared to the LIFT Technique
For each row, the feature described in each column is represented as present (X) or absent (-). (*) In parenthesis, the total number of trocars used. (**) Traction of the gallbladder fundus by means of percutaneous and/or intracorporeal elements (sutures, forceps, needles, or magnets) other than trocars.
LIFT, “Less Incisions but Four Trocars” SLC, strategic laparoscopic cholecystectomy.
First, almost all authors propose a reduction in the number of trocars,1–6,8,22 This forces to use some mechanism of suspension of the gallbladder fundus for a correct triangulation, for example with percutaneous sutures,5,6,22 intracorporeal ligatures 8 (Endoloop™, Medline, Covidien), endocavitary retractors 3 (Endograb™, Virtual Ports Ltd., Israel) or percutaneous forceps without trocar1,2,5 (MiniLap Grasper™, Stryker, California; Mini-Lap™ Tech, NY). In addition, it is very common for trocar reduction techniques to use flexible telescopes1,2,4,6,8 and articulated graspers1–5,7,22 to minimize the collision of instruments in the umbilical zone. The increase in the cost of these instruments is difficult to justify, as pointed out by Gurusamy et al. 23 in a recent Cochrane review. In the LIFT technique, the traction of the gallbladder is performed with a resistant grasper that allows a secure grip for the hepatic suspension and dissection from multiple angles, 6 and the dissection maneuvers are identical to the standard LC, avoiding the need for a learning curve. This differs from other SLC whose average operative times exceed two hours in the first cases.4,7 Regarding the conversion rate, we did not have to modify the LIFT technique in any patient, which compares favorably to other series that show conversion rates between 3.3% and 16%.1,3,7
Some surgeons do not use any trocar greater than 5 mm,2,3,5,6 which imposes several limitations. The most important drawback is that it forces to use 5-mm clips, perhaps unsuitable for thick or inflamed cystic ducts, which may reduce the safety of the cystic stump closure. In fact, the risk of bile leakage remains a concern related to SILC, with reported biliary leaks between 1% and 3.7% of cases.24,25 In the LIFT technique we always use 10 mm clips, and it is possible to use other tools such as gauzes, swabs, sutures, and right angle dissectors, if necessary. All this may justify that there has not been any case of biliary leakage in our series. Another limitation derived from the use of small trocars is the difficulty in extracting large stones. Thus, Cui et al. 6 limit the size of the stones to 35 mm, Jategaonkar and Yadav 8 have to fragment those stones greater than 10 mm before extracting the gallbladder, and Dan et al. 5 surprisingly exclude patients with stones larger than 5 mm. In the LIFT technique, the vertical incision in the midline can be extended without interfering with the second intraumbilical trocar, allowing the extraction of calculi of any size or bulky gallbladders.
Finally, several SLC studies exclude patients with BMI >35, possibly due to the greater technical difficulties.1,3,5 In our clinical practice it is very difficult to exclude patients with BMI >35, considering that Saudi Arabia has one of the highest obesity rates in the world. Moreover, we have perceived that in obese patients the pure intraumbilical access is advantageous compared to the clasical subumbilical one, since the navel stalk is the area of the abdominal wall in which the skin is closest to the aponeurotic plane.
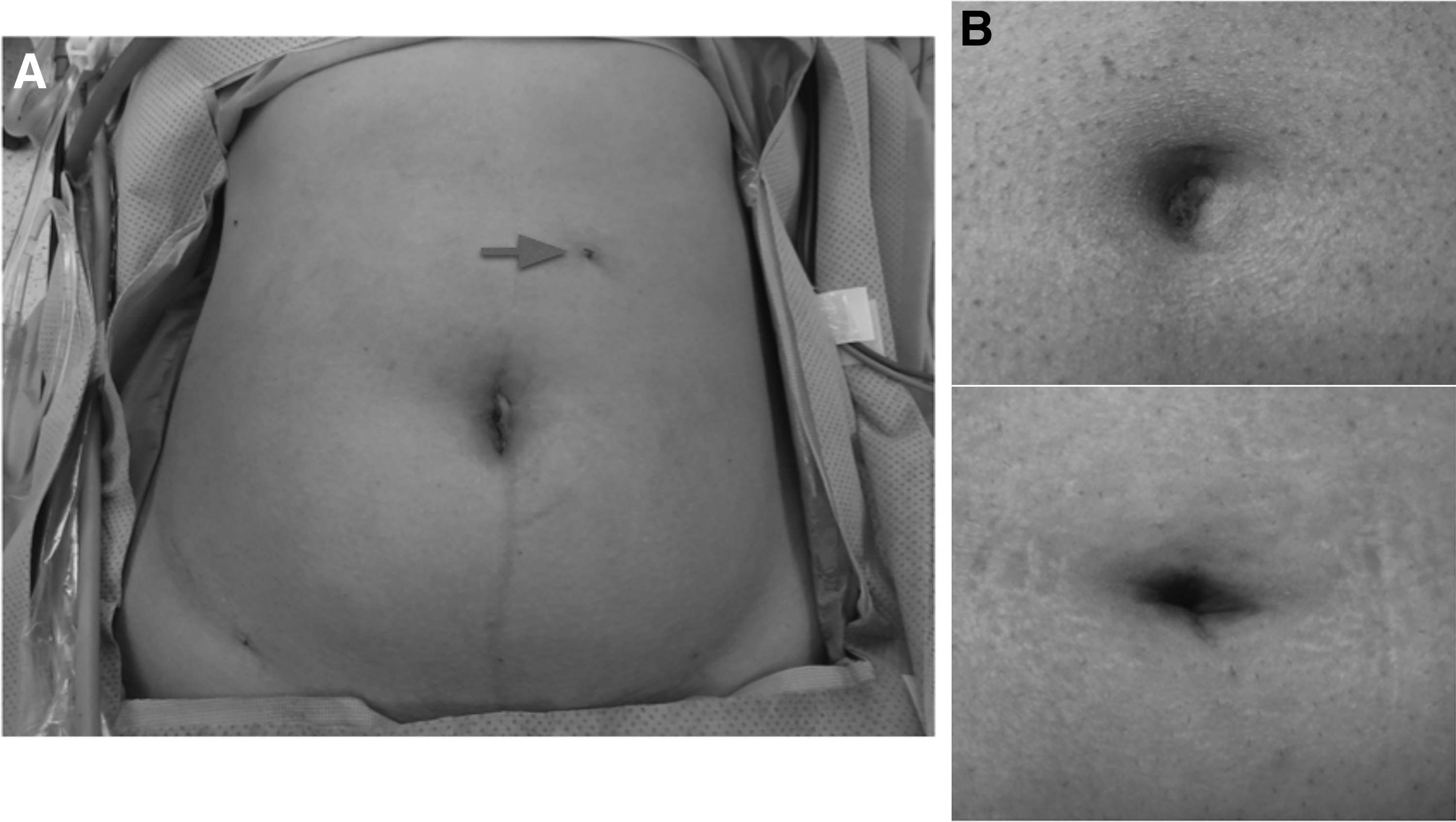
The clinical evaluation of minimally invasive surgery has focused on safety, while assessment from the cosmetical point of view is practically nonexistent. 26 However, although cosmesis is a preeminent factor in patients concerned with body image, for the majority it is less important than the reputation of the surgeon or the complications of surgery. 27 There is very little information about the long-term cosmetic satisfaction of patients, and also the studies published to date show remarkable disparities. Lurje et al. 26 published the first randomized study that showed a higher score in body image and in cosmetics with SILC compared to LC after 1 year. In contrast, Evers et al. 15 found that the lowest postoperative pain and the best aesthetic assessment in favor of SILC had no impact on quality of life, questioning whether these advantages outweighed the higher incidence of adverse events and lower feasibility of SILC. Finally, in the most recent meta-analysis available, Haueter et al. 13 point out that despite the cosmetic superiority of SILC over LC, this finding is not reflected in the common practice, where LC remains the routine technique for the benign diseases of the gallbladder. These disparities also affect evaluation methods, and while some studies use generic tools (SF-8, SF-12, SF-36, EQ-5D, QoL),11,13,28 others add specific and more complex scales to evaluate the cosmesis, such as BIQ (Body Image Quality), PSAQ (the scar evaluation questionnaire), or the Hollander scale.11,26,29 For the LIFT technique, we opted for an easy and quick-to-use cosmetic scale with four values, similar to that used in other studies.3,8 We believe that this scale allows us to obtain an evaluation focused solely on the scar, ignoring other aspects such as quality of life or body image that in most studies are not modified with the use of SILC. Similar to other SLC series,3,8 our patients have positively assessed LIFT, in a statistically significant way compared to LC (Fig. 4).
The limited number of cases has prevented the stratification of the analysis, but we agree with Marks et al. 11 that patients who demand a better aesthetic result during the preoperative visit are usually younger, female, and with a lower BMI. It is possible that these patients may be predisposed to select the most “novel” procedure because of the instinct to believe that “the new must be better” and respond more favorably to the postoperative satisfaction survey. In the opposite direction, we have also perceived that patients with little interest in the cosmetic aspect tend to give lower scores on the satisfaction scale, in line with what Bencsath et al. reported, 30 who found that less than half of the patients remembered correctly the number of incisions that had been made in a retrospective evaluation of patients undergoing SILC for a period of 2 years.
When evaluating the postoperative pain, Lurje et al. 26 did not find any significant difference between LC and SILC, which could be attributed to the absence of unified criteria for pain assessment in addition to the differences in the procedure itself. In this regard, it is interesting the metaanalysis performed by Milas et al., 12 which included 30 randomized studies with a total of 2411 patients comparing LC and SILC. The main finding was that in the trials in which the patients were blinded, the difference in favor of the SILC was not statistically significant, however, in a subset of trials without blinding the difference in favor of the SILC was four times higher and statistically significant. Unlike other SLC series,2,5 we did not find significant differences in postoperative pain between LIFT and LC, except in the 3-month review, something that does not have an explanation for us. Downsizing the port incision and the number of port incisions have been suggested to reduce the magnitude of postoperative pain, but it is well known that other factors apart from the technique are responsible for these variations, like the duration of surgery, pressure of pneumoperitoneum, bile leakage, and individual differences in pain perception among patients. We agree with Bencsath et al. 30 in pointing out the umbilicus as the most painful area for most patients undergoing LC, so it seems difficult to achieve a significant reduction of pain by eliminating some extra-umbilical trocars while maintaining the primordial access through the umbilicus.
There are several limitations to this study. First, as a retrospective study, these results should be confirmed by prospective trials. Second, because of the small sample size, statistically significant conclusions could not be drawn among subsets of patients according to age, gender, or BMI, something that in our opinion could increase the value of the technique when offered to properly selected patients. Third, the simplicity of our cosmetic satisfaction scale can be criticized when compared to other complex tools designed for this purpose. But, considering the social and cultural background of our patients, we feel that this scale was just a handy method of judging the scar outcomes on a gross scale while not interfering with patient's intimacy.
Although we have not conducted any cost-analysis comparisons in this study, given that the routine laparoscopic instruments were used without any major complications, we feel that the LIFT technique may be considered an efficient redesign of SLC, which provides improved cosmetic results by embodying some outstanding features of SILC (multiple per-umbilical instruments, reduced number of scars) into a safe and feasible procedure at no extra cost compared to conventional LC.
Conclusions
In this study, we describe a technical variant for LC in selected patients. The LIFT technique has been similar to LC in terms of safety, rate of complications, costs, and feasibility, and we believe that it can provide a significant improvement from the cosmetical standpoint, especially in those patients who are concerned about the aesthetic result and who demand it in the preoperative interview.
Footnotes
Acknowledgments
The authors would like to thank Dr Antonio Morandeira-Rivas, MD, PhD, for performing the statistical analysis, and Dr Mark William Halliday, MD, FRCS, for his assistance in the preparation and correction of style of the article.
Disclosure Statement
Dr Joaquin Picazo-Yeste, Dr Serge El-Khoury, Dr Ali YAlansi, Dr Muhammad A Malik, Dr Ashwyn A Nelson, Dr Saidislam K Mallaev, and Dr Praveen Reddy have no conflicts of interest or financial ties to disclose.