
Abstract
Abstract
Background:
Minimally invasive liver surgery has gained increasing popularity over the past decade. Nevertheless, laparoscopic treatment of lesions located in the posterior–superior locations remains challenging because of the difficulty to reach a safe exposition of those regions of the liver. We present a new retroperitoneoscopic approach for the minimally invasive treatment of posterior tumors.
Materials and Methods:
Between May and July 2018, 2 patients with solitary liver metastasis of colorectal origin underwent retroperitoneoscopic liver resection in the prone position. The operation was conducted with three to four trocars, the CO2 insufflation pressure was set at 20 mmHg. Liver transection was carried out by alternating bipolar coagulation and clips, without clamping of the hepatic inflow.
Results:
There were no intra- or postoperative complications. The procedure was completed in both cases without conversion after 120 to 180 minutes, respectively. Complete resection was achieved in both cases. Hospital stay was 3 and 5 days.
Conclusions:
Retroperitoneoscopic liver resection is feasible and safe. This approach could be suggested as an additional therapeutic option, especially in cases of redo resection at the posterior segments.
Introduction
The first laparoscopic wedge resections for a benign liver tumor was described in 19911 followed in 1993 from the first metastasectomy. 2 Few years later, anatomical resections3,4 and even major hepatectomy have been described. 5 After the initial skepticism related mostly to fear for bleeding complications, minimally invasive liver surgery gained increased popularity and developed progressively along the past 15 years.6–8 Many studies have been performed and confirmed feasibility and safety of the laparoscopic approach. 9 Laparoscopic liver resections are divided according to the complexity of the procedure in different categories. 8 Small wedge resection, resections of the anterior segments (4b, 5, 6), and left lateral resection are classified as “minor resections,” whereas hemihepatectomies and resections of the posterosuperior segments are allocated in the group of “major hepatectomy.”
Resection of right anterolateral segments and left lateral sectionectomy are actually considered domain of minimally invasive surgery, at least in specialized hepatobiliary centers. 10 Differently, resection of the posterolateral segments as well as major hepatectomies, which are technically demanding, are still performed in few specialized units with extensive experience in hepatobiliary surgery. The advantages of minimally invasive techniques compared with conventional surgery justify the increasing extension of the indications also for liver resection.11–13 Most studies have demonstrated a reduced hospital stay, lesser requirement of analgesics and less intraoperative bleeding.14–17 A meta-analysis published by Mirnezami et al. showed a significant decrease in the incidence of complications with laparoscopic liver resection compared with open surgery. 14 Specifically, minimally invasive approaches seem to have lower rates of wound infections, incisional hernias, and cirrhotic decompensation events. 17
In an earlier study, we report our experience with laparoscopic liver surgery at the Kliniken Essen-Mitte, a referral center for minimally invasive and oncologic surgery. 18 Over a period of 13 years (2000–2013), 94 laparoscopic liver resections have been performed including 31 “major hepatectomies.” The conversion rate was 8.5% and the mortality rate 1%. Our experience increased constantly over the past 5 years (2014–2018) including >100 laparoscopic resections out of 257 operations performed during this period. Combining the extensive experience with the retroperitoneoscopic access for adrenal surgery 19 and of laparoscopic liver surgery, we developed a novel minimally invasive approach for treatment of posteriorly located liver tumors using the retroperitoneoscopic route.
Materials and Methods
After approval by the institutional ethical committee, a retrospective record review at our institution identified 2 patients who underwent retroperitoneoscopic liver resection between May and July 2018. These patients were treated with the institutional standard of care. Informed consent was obtained before any operation.
The first operation was performed in a 72-year-old male patient primarily affected by a sigmoid colon cancer with simultaneous multiple liver metastasis. The patient underwent laparoscopic left colectomy in January 2012 without liver resection due to bilaterality and number of the hepatic lesions. The postoperative course was uneventful. Final histology showed a nodal positive (1 out 13 lymph nodes) pT3 colonic cancer. One month after surgery, chemotherapy with folinic acid, fluorouracil, and oxaliplatin (FOLFOX)+bevacizumab was started. Owing to occurrence of severe polyneuropathy, oxaliplatin was stopped after the second administration, whereas bevacizumab was stopped in June 2013 due to proteinuria. A morphologic complete remission of the hepatic lesions was observed. In August 2015, a biochemical recurrence confirmed by computed tomography scan was observed. Chemotherapy with folinic acid, fluorouracil, and irinotecan (FUFIRI) was started and followed later on by the FOLFOX protocol. The last magnetic resonance imaging on December 2017 showed a solitary lesion located in the left lateral segment and chronic cholecystitis that correlated with recurrent pain in the right upper quadrant. On January 2018, a laparoscopic liver resection (segment 3) and a simultaneous cholecystectomy have been performed. The postoperative course was uneventful and a radiological follow-up was planned few months later. A new lesion at segment 6 was detected (Fig. 1). Redo surgery by the posterior approach was planned.
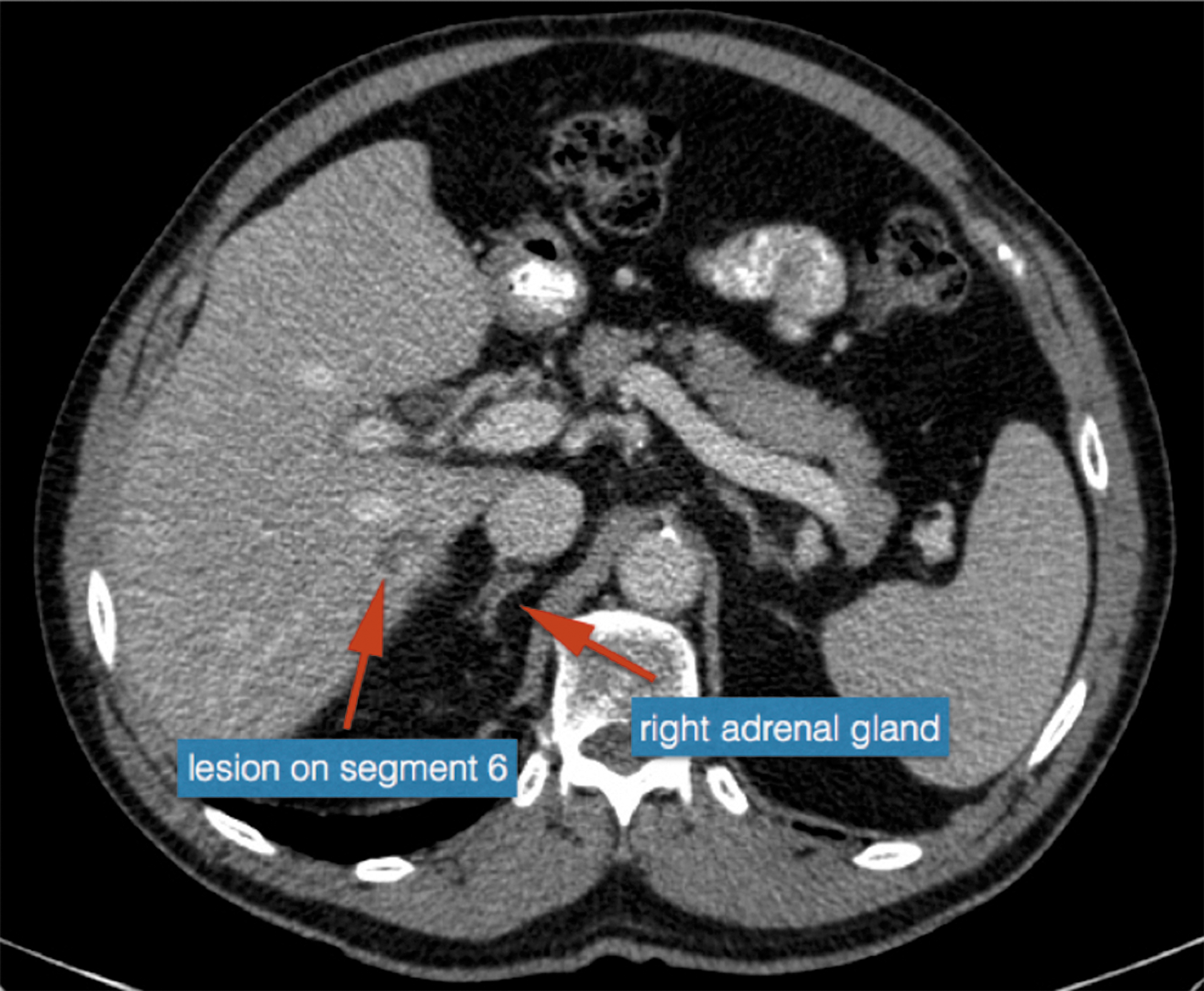
CT scan showing a solitary hepatic lesion located at segment 6 in front of the right adrenal gland and behind one branch of the portal vein.
The second case was a 63-year-old female patient affected by rectal cancer. In 2012, she underwent transanal resection of a rectal polyp at the level of the dental line that revealed a pT1 (sm2) malignant tumor at final histology. A follow-up strategy avoiding abdominoperineal rectal excision was primarily set in accordance with the patient at the tumor board review. After 3 years, she presented with a local recurrence infiltrating the vagina and simultaneous bilateral liver metastasis. After neoadjuvant chemotherapy with folinic acid, fluorouracil, and irinotecan (FUFIRI) combined with short-course radiotherapy (25 Gy delivered in five fractions), a laparoscopic-assisted abdominoperineal rectal resection with partial colpectomy as well us a simultaneous liver resection (segments 2–3 and 5) was performed. A complete resection of both primary tumor and liver metastasis could be achieved. One year later, the patient presented with two new hepatic lesions at segments 4 and 7. Induction chemotherapy (FUFIRI+cetuximab) was followed by conventional (open) left hepatectomy and wedge resection of the lesion at segment 7. Ten months later, a new metastasis at segment 8 was diagnosed and resected by the laparoscopic approach. Unfortunately, a local recurrence was diagnosed 6 months later at the resection line (Fig. 2). In August 2018, a retroperitonescopic resection was planned.

MRI scan showing a solitary hepatic lesion located at segment 8 behind the right hepatic vein and showing adhesions to the diaphragm after previous laparoscopic surgery. The red circle highlights the position of the lesion in the coronal view and its contact to the diaphragm. MRI, magnetic resonance imaging.
Operation
Patients were placed in prone position with bent hip joints as described for posterior retroperitoneoscopic adrenal surgery (Fig. 3). 20 The liver was approached from the right side with the trocar position being analogous to the retroperitonescopic adrenalectomy (Fig. 4). The first incision was placed on the tip of the 12th rib and the retroperitoneal space was reached by blunt dissection. Under finger control, the 11th rib was localized and a 12 mm single-use trocar was inserted just below the tip of the rib. Differently from adrenal surgery, we preferred at this position 12 mm trocar to permit the insertion of clips, vascular staplers, or vessel clamps that could be necessary in liver surgery. A blunt trocar with an inflatable balloon and an adjustable sleeve was introduced into the initial incision site and blocked (Fig. 5). A capnoretroperitoneum was established and maintained with a pressure of 20 to 25 mmHg. The first step of the operation was opening of the Gerota's fascia to reach the retroperitoneal space. Finally, the third 10 mm trocar was inserted under direct view between the spine and the first incision. The 10 mm −30°camera was then switched from the middle to the medial/paravertebral trocar. In 1 case, an additional trocar was necessary for retraction of the retroperitoneal fatty tissue; the position of the fourth trocar is shown in Figure 4. The adrenal gland was visualized and mobilized cranially to expose the retrohepatic vena cava and the peritoneum. In 1 case, the main adrenal vein was divided to allow better retraction of the adrenal gland and circular exposure of the vena cava. Encircle of the vena cava with a vessel loop can be performed until reaching the right hepatic vein, as necessary. Before opening the retrohepatic peritoneum, intraoperative ultrasonography was performed to precisely localize the lesion. The peritoneum was finally incised and the liver exposed. The dissection lines were fixed using intraoperative ultrasonography, the resection was performed without Pringle maneuver by bipolar forceps and Ligasure (Medtronic, Minneapolis). Clips were used for dividing vessels >3 mm. The specimen was retrieved using an endobag (Endo Catch Gold, Medtronic, Minneapolis) through the primary incision. After accurate hemostasis, an easy-flow drainage was left in place through the lateral port.

Patient's position.
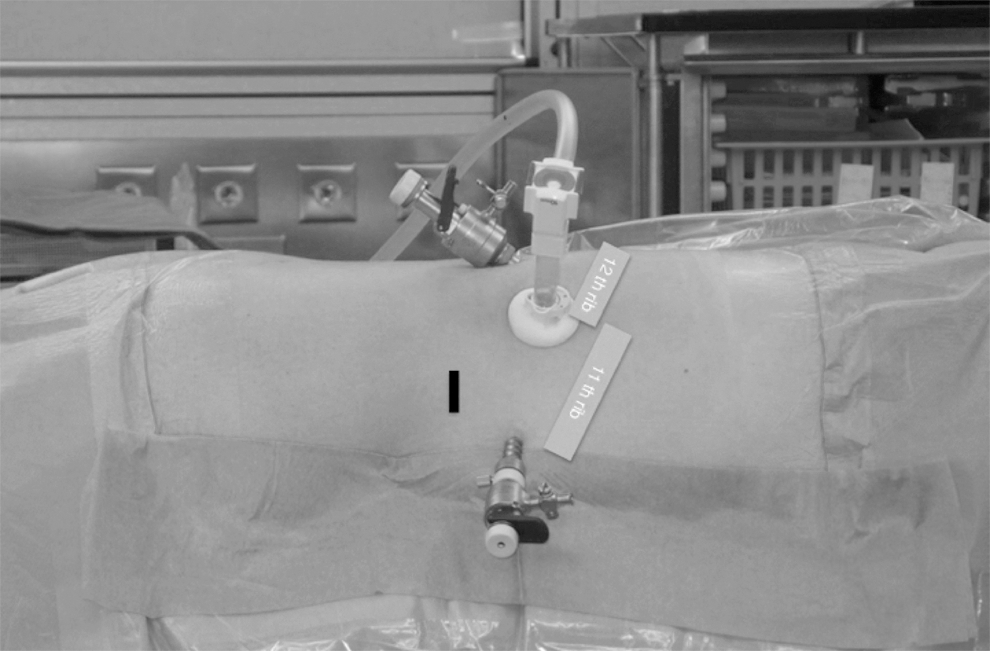
Trocar position for the retroperitoneoscopic approach. The first incision is made on the tip of the 12th rib and covered later on with the blunt trocar with an inflatable balloon and an adjustable sleeve. The lateral incision is placed on the tip of the 11th rib: differently from the adrenalectomy (as shown in this picture), a 12 mm trocar was used. The black line shows the position of a fourth, eventually needed, trocar.

Blunt trocar with inflatable balloon and adjustable sleeve to allow airtight coverage of the first incision.
Results
There were neither intra- nor postoperative complications. The operating time was 120 minutes for the first case (metastasectomy at segment 6) and increased to 180 minutes for the second operation, including liver resection (segment 8) “en-bloc” with the diaphragmatic muscle. The intraoperative blood loss was <100 mL in both cases. No intra- or postoperative blood transfusions were necessary. The abdominal drainage was removed on days 2 and 4, respectively. In the second case, an additional thoracic drain was used after diaphragmatic resection (Fig. 6). Histology confirmed the complete (R0) resection of a solitary metastasis of the colorectal adenocarcinoma in both cases. Patients were discharged on days 3 and 5 and sent back to the referral oncologist for further follow-up.

View of the three posterior incisions (the abdominal drain is still in place) after removal of the thoracic drain.
Discussion
Three different approaches for laparoscopic liver resections have been described so far 21 : pure laparoscopic (the procedure is performed through laparoscopic ports and only the extraction of the specimen requires an auxiliary incision), hand-assisted (with routine placement of an extra hand port), and hybrid hepatectomy (laparoscopic mobilization and minilaparotomy for vascular dissection and parenchymal transection). We developed a new alternative approach for laparoscopic liver surgery through the retroperitoneoscopic route. This technique is suitable for resection of lesions located at the posterior right segments. The access to this area of the liver is difficult, generally requiring extensive mobilization of the right lobe to ameliorate the exposition of the operating field. Because of the objective technical difficulty, confirmed by higher conversion rate, higher blood loss, prolonged operative time, and narrow surgical margins, these posterior resections ere included into the “major operations.”22–24
The main advantage of the retroperitoneoscopic access is the direct view to the posterior segments and to the vena cava without mobilization of the liver. Moreover, this route avoids the previous operative field in case of reoperations as in both of our patients. We routinely use a pressure of 20 mmHg or more for retroperitonescopic adrenalectomy. That results surprisingly in significant increases of cardiac output (+72%), stroke volume (+42%), mean arterial pressure (+39%), and mean pulmonary arterial pressure (+36%) as well as central venous pressure (+37%) without being associated with adverse effects. 25 High gas pressures widen the operative space and are responsible for compression of the small veins avoiding intraoperative bleeding during the transection of the parenchyma. As CO2 is a diffusible gas, the occurrence of relevant intraoperative gas embolism was not observed as well during the procedures.
Different techniques have been described to approach the posterolateral segments 24 : (1) abdominal approach, (2) transthoracic approach, and (3) semiprone position. For the abdominal approach, the patient was set in the supine dorsally elevated position. In addition, the operation table was tilted leftward by 15–45° according to the position of the lesion. The right liver was fully mobilized by transection of the perihepatic ligament and division of the short hepatic veins. The liver was then rotated toward the anterosuperior direction using retractors and the ultrasound-guided transection was started. For tumors located in the subdiaphragmatic area, a transthoracic approach can be preferred. For resection of segment 6, the classical “French position” was used. The liver was mobilized from the diaphragm and the right adrenal gland dividing the short hepatic veins. During laparoscopic resection of segment 7, the patient was placed in the left lateral decubitus position with the right arm suspended. In addition to three trocars placed in the right upper quadrant of the abdomen, two balloon-tipped trocars to isolate the chest from the abdominal cavity were inserted through the diaphragm in the same intercostal space. Deflation of the right lung was unnecessary. Recently a laparoscopic approach in a semiprone position has been described. 26 The first port was placed in the right pararectal line, 10 cm below the costal margin, and was used to introduce a 30° laparoscope. Three trocars were placed below the costal margin in the right pararectal line, anterior axillary line, and posterior axillary line. After hilar dissection and mobilization of the liver, an intercostal port was inserted at about the seventh intercostal space in the anterior axillary line. Differential lung ventilation was used when intercostal ports were planned. In their study, the authors affirm that after the introduction of the semiprone position, the percentage of laparoscopic resections of tumors in the anterosuperior and posterior segments could be increased from 17.5% (7 out of 40 patients) to 57%. (69 of 120 patients) (P < .001). Nevertheless, they stated that partial resection of a posterosuperior or anterosuperior tumor was more difficult in this position than in hemihepatectomy or sectionectomy position even if less blood loss was reported in the semiprone group. Postoperative complications included 2 cases of intra-abdominal abscess (3.6%).
To the best of our knowledge, this is the first report of minimally invasive liver surgery in prone position through the retroperitoneal route. We believe this approach could become a new option for laparoscopic resection of tumors at the posterior segments and hopefully increase the indications for limited resection (metastasectomy), allowing parenchymal preservation. This argument is particularly important for the increasingly aggressive surgical approach to liver metastasis. Moreover, limited resections are related with significantly less complication when compared with right hepatectomy. In a study comparing laparoscopic resection of the posterior segments with formal laparoscopic right hepatectomy, Portigliotti et al. 27 demonstrated that liver failure (17.1% versus 0%; P = .001), biliary leakage (6.0% versus 1.2%; P = .01), intra-abdominal collection (19.1% versus 2.5%; P = .001), and pulmonary complication (16.1% versus 1.2%; P = .001) were significantly increased in the hepatectomy group. Moreover, the transfusion requirement was significantly higher in the right hepatectomy group (1.2% versus 13.1%; P = .003).
This study has several limitations. First, it is a retrospective study that included a very limited number of patients. The selection criteria for the retroperitoneoscopic liver resection should, therefore, be evaluated on a larger number of cases. The second concern is about the reproducibility of the results as the operations were performed in a center with extensive experience in both minimally invasive liver surgery and retroperitoneoscopic adrenal surgery. The authors have acquired over the past 20 years extensive skill with the retroperitonescopic route by performing >2000 adrenal procedures and are, therefore, familiar with this approach and its possible complications. The position and relationships of the structures could be unfamiliar. Moreover, a major concern could be related to intraoperative bleeding and theoretical necessity of conversion that requires the change to a supine position. This was up to now never the case in our adrenalectomy cases, as even a major lesion of the vena cava was controlled by the retroperitoneal route. The last point is that the resections were performed without clamping of the hepatic inflow, as we did not explore the possibility to perform a Pringle maneuver. We can actually only suppose that, according to our experience in complex adrenalectomies, the occlusion of the hepatic pedicle could be safely performed from the back.
Retroperitonescopic liver resection for tumors of the posterior segments seems to be feasible. This new approach can represent in the future a new option and hopefully increase the indication for minimally invasive liver surgery. Nevertheless, the results of this report should be confirmed by further studies including a larger number of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.