
Abstract
Abstract
Aim:
Percutaneous nephrostomy (PN), the indispensable interventional procedure in situations such as obstructive uropathy and pyonephrosis, requires serious experience. As a result, many urologists and radiologists avoid this procedure. However, this can leave both doctor and patient in a difficult situation when it is necessary. In this study, we aimed at presenting a nephrostomy insertion technique by using a transrectal ultrasonography probe that we use in our clinic and we believe that this has made the PN procedure easier, along with our results.
Patients and Methods:
Data from patients with PN inserted by using this method at our clinic from January 2013 to December 2018 were retrospectively scanned. The nephrostomy indications, complications, and success rates for patients were assessed. All procedures were performed under local anesthesia without the help of a radiologist.
Results:
A total of 84 patients, 55 male and 29 female, had 146 nephrostomy catheters inserted. Nephrostomy was performed in 52 patients due to obstruction linked to malignancy and in 32 patients due to reasons other than malignancy. The procedure was successfully concluded in all patients independent of degree of hydronephrosis.
Conclusion:
With our technique, PN was found to be performed easily with low complication rates.
Introduction
Obstructive nephropathy is a situation that may cause pain, infection, sepsis, and loss of kidney function. Percutaneous nephrostomy (PN) lowers the internal pressure in the collecting system linked to obstruction, preventing parenchymal injury. It is a time-gaining drainage method in ureter injury or ureter anastomosis leaks until the injury heals. At the same time, it is a life-saving procedure in situations with pyonephrosis. PN insertion was described for the first time by Goodwin in 1955. 1 According to the standard Seldinger technique, entry is with a needle, a guidewire is sent through the needle into the kidney, and series dilatation is applied over the wire.
Traditionally, the PN procedure is performed accompanied by fluoroscopy using contrast material. In 1974, Pedersen 2 performed the PN procedure accompanied by ultrasonography (USG) and the use of USG for PN rapidly increased. Currently, USG is accepted as a reliable imaging method for PN. 3 USG is used in patients where contrast material cannot be administered, especially in children, pregnant women, and those with kidney failure and allergies. For this procedure, generally a 3.5 MHz convex abdominal probe is used. 3 However, this application requires serious USG experience. In patients with mild hydronephrosis, this procedure is more difficult, and even in experienced hands sometimes it may fail. As a result, generally USG is performed by radiology experts with better experience for nephrostomy insertion.4,5
Prostate biopsy accompanied by transrectal ultrasonography (TRUSG) is commonly performed by urologists. To obtain a biopsy from the targeted region of the prostate, a needle director attached to the TRUSG probe is used. On the USG device screen, guide lines indicate the line that the needle sent by the needle director will pass through. As the biopsy needle sent through this apparatus follows the guide lines on the USG device screen, it is possible to obtain tissue samples from the required region of the prostate. We used this method of prostate biopsy for entry into the kidney in the PN procedure. In this article, we share our technique and results.
Materials and Methods
From January 2013 to December 2018, a total of 146 nephrostomies were performed in 84 patients with this method at our clinic. If nephrostomy was removed in patients with obstruction linked to malignancy, PN was inserted again. The demographic data, nephrostomy indications, hydronephrosis levels, complications, success rates, and results were retrospectively screened from the clinical archive. Before the procedure, routine prophylactic antibiotic treatment was administered. All procedures were performed under sterile conditions in the urology biopsy room. Patients and relatives were given information about the reason for, benefits, and potential complications of the procedure beforehand and then signed consent forms. All procedures were performed by 2 urologists, with no help from a radiologist at any point. All procedures were performed under local anesthesia and in lateral decubitus position. This study was approved by Ordu University Local Ethics Committee (2017/108/99).
Methods
Patients were placed in lateral position with the kidney for nephrostomy insertion uppermost and a silicon pillow under the opposite side. During the procedures, a Mindray M5 model USG® (Shenzhen Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) device was used. First, the kidney was imaged by using a 3.5 MHz convex abdominal probe (Model: 3C5s, Shenzhen Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) from the posterior of the mid-axillary line. The degree of hydronephrosis and general structure of the kidney were assessed, and the calyx group with nephrostomy insertion planned was determined. The distance between the skin and calyx was measured to determine the depth of the dilatator that would be sent during dilatation. Then, a 6.5 MHz TRUSG® probe (Model: 6CV1s, Shenzhen Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) with a needle director used for prostate biopsy attached was used. The image depth of the probe was set to at least 10 cm, and the kidney and calyx with planned insertion were imaged again. To protect the colon and neighboring organs from injury, images were always obtained from the posterior of the mid-axillary line. The region where the target calyx was best observed was determined. At this point, local anesthesia was applied to the line where the needle would pass through the skin to the kidney (Fig. 1). For local anesthesia, nearly 15 cc 2% prilocaine (Citanest®; AstraZeneca, UK), with 3 cc skin and subdermal and 10–12 cc along the needle line, was used. As it is atraumatic and does not deviate, a diamond-tipped needle was chosen for entry into the kidney.
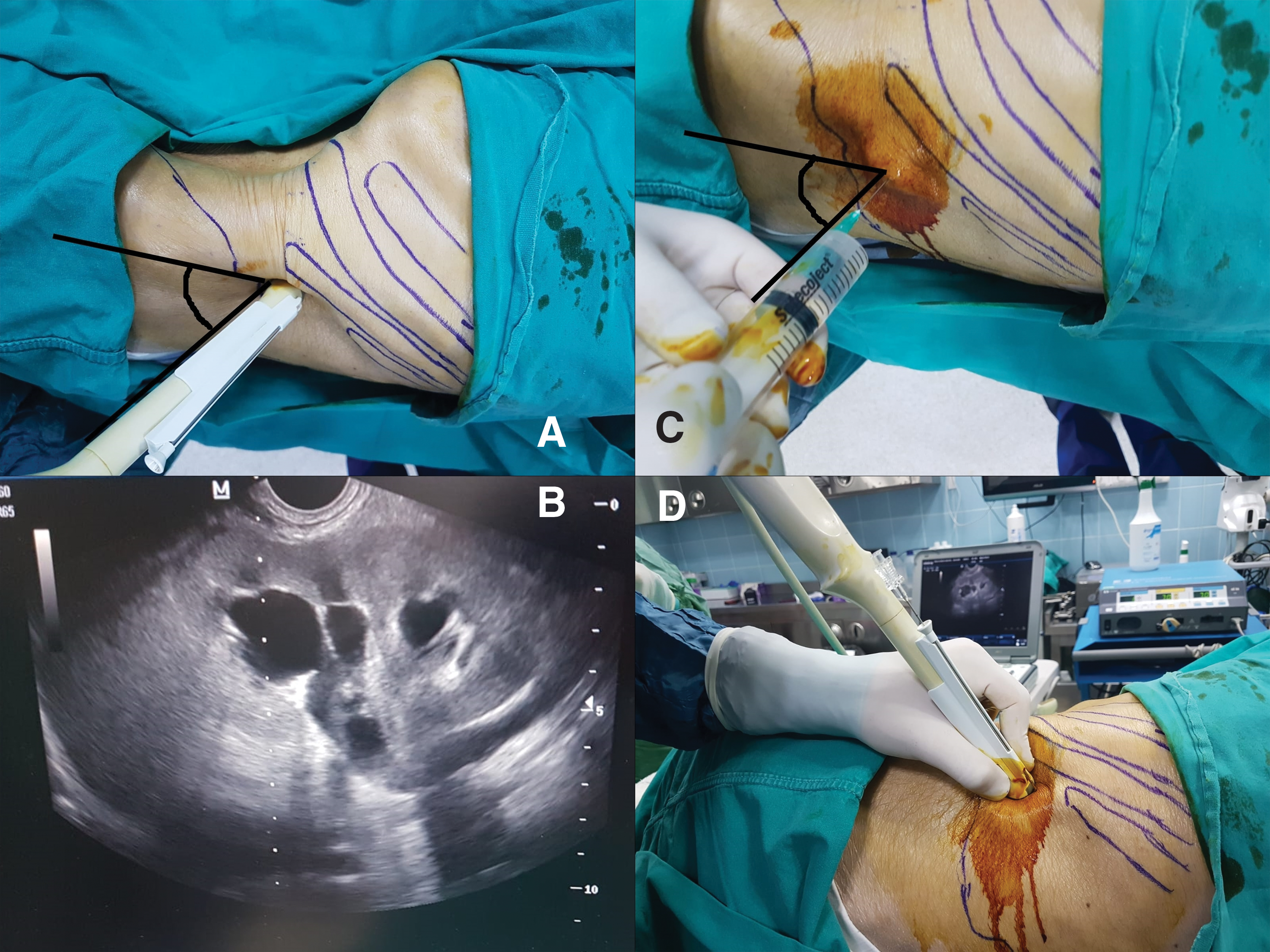
The kidney is imaged with the TRUSG probe
On the USG screen, the biopsy guide lines were activated. The guide lines were brought in line with the target calyx, and an 18-gauge 20-cm diamond-tipped needle was sent through the needle director into the kidney. After entry into the calyx, the needle sheath was inserted and the needle was removed. When the needle was removed, it was observed that urine passed through the sheath. In situations where purulent urine appeared, culture was obtained in a sterile injector. After a PTFE-coated J tip 80-cm × 0.023-inch guidewire was inserted into the kidney through the sheath, the needle was removed with a guidewire in place. After a 5-mm cut was made where the wire entered the skin, 8F, 10F and 12F dilatation was performed by using semi-rigid dilatators included in a nephrostomy set over the wire. After dilatation, a 12F nephrostomy tube was inserted into the kidney collecting system over the wire. After the wire was removed, the nephrostomy was secured to the skin.
Results
One hundred forty-six nephrostomies were inserted in a total of 84 patients, 55 male and 29 female. The median age of patients was 65.47 ± 17.28 (21–90) years. Nephrostomy was performed due to obstruction linked to malignancy in 52 patients and due to nonmalignant reasons in 32 patients. Nephrostomy indications are shown in detail in Table 1. In 26 kidneys, there was grade 1 hydronephrosis, in 62 kidneys grade 2, and in 58 kidneys grade 3. Twenty-five patients had nephrostomy inserted in the right kidney, 35 patients in the left kidney, and 24 patients had bilateral nephrostomy. All of the patients with bilateral nephrostomy inserted were identified to have obstruction linked to malignancy.
Nephrostomy Indications
Except 1 patient, all interventions were successful on the first attempt. Targeted calyx puncture and guidewire placement were successful in all patients where the calyx could be seen; however, a nephrostomy tube was not inserted on the first attempt in 3 patients. These patients were given information about the procedure again and after more careful local anesthesia, nephrostomies were successfully inserted on the next day with the same method. Nephrostomy placement was achieved with intravenous contrast administration and fluoroscopy guidance for 1 patient who had iatrogenic ureteral injury and no hydronephrosis.
Major vascular injury or injury of neighboring organs such as colon, liver, spleen, and lungs was not observed. In 8 applications due to pyonephrosis, fever above 38 degrees was observed after the procedure. These patients were already using antibiotics. Fever reduced with a single intravenous dose of paracetamol and did not recur. In 43 applications, urine appeared hematuric after the nephrostomy tube was inserted. No patient had hemorrhage requiring surgical intervention. Apart from 1 patient, the others recovered within 6 hours and the urine color cleared. One patient had 2 U transfusion due to continuing hemorrhage after the procedure. In the second week after treatment with recurring hematuria attacks, renal angiography identified arteriovenous fistula and it was treated with embolization. No patient developed septicemia.
Four patients with no urine output from the nephrostomy after the procedure had antegrade pyelography performed. In these patients, the nephrostomy tube appeared to have entered the upper section of the ureter and was retracted and insertion in the pelvis of the kidney ensued.
Discussion
With our technique, a needle director attached to a TRUSG probe was used and the collecting system was successfully entered in nearly all patients. This method makes the PN procedure much easier and we believe that it will be possible for urologists to easily insert nephrostomies with this method. In the literature, PN success according to the imaging method used is reported as 84%–99%. 6 This method could not be used in a patient where the calyx could not be observed with USG. Our success rate is 99.3%.
Urologists commonly encounter patients requiring PN; however, the number of urologists who can perform this procedure is low. A multicenter study in the United Kingdom reported that <0.5% of nephrostomies were inserted by urologists. 7 Another study by Bird et al. reported that this rate was 11%. 8 The number of urologists performing the PN procedure themselves is increasing. 9 Studies have found that the success of urologists performing nephrostomy with USG guidance is equal to that of radiologists.4,5 The study by Mahaffey found that the complication and success rates in 100 nephrostomies inserted with USG accompaniment were similar to radiologists. 4 Generally, the nephrostomy procedure is performed by radiologists with USG guidance in our country. The use of USG instead of fluoroscopy during entry allows observation of anatomic structure, and it reduces risks such as injury of neighboring organs such as spleen, liver, and colon and major vein injury 3 (Fig. 2). In addition, avoiding the use of radiation during this procedure is important, especially for patients and clinicians. Another disadvantage of fluoroscopy is that it requires contrast material to visualize the collecting system. It is not possible to use contrast in all patients due to contrast allergies, chronic kidney disease, etc. In these situations, performing the intervention with USG guidance is an advantage compared with fluoroscopy. In addition, USG is a more easily available imaging method than fluoroscopy. Currently, the majority of urology clinics have a USG device. In addition, dependence on other departments is prevented when urologists perform this procedure themselves.
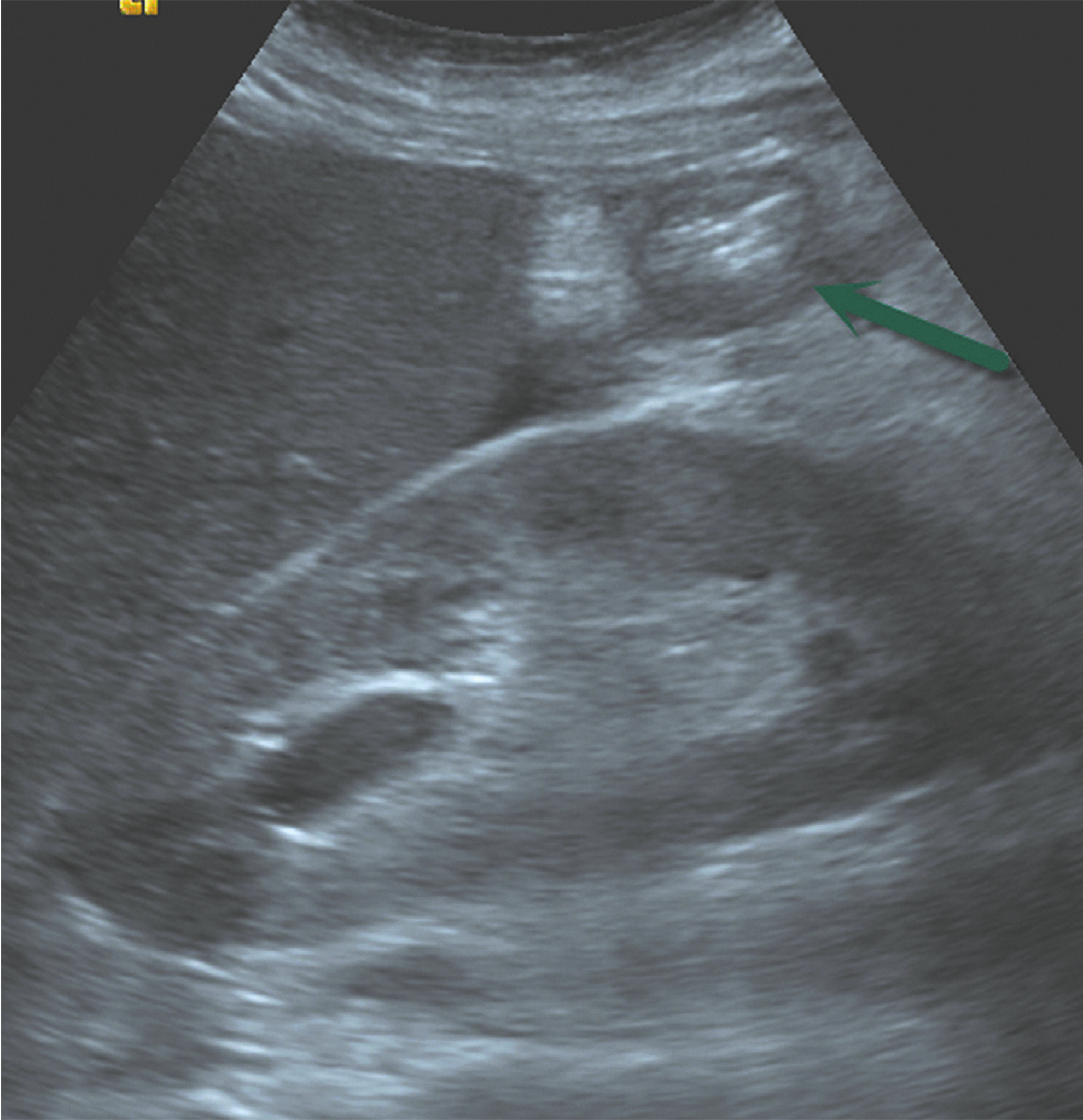
Longitudinal ultrasound image of the right kidney shows interposition of a bowel loop (arrow) filled with air between the skin and kidney. 10
In fact, urologists are accustomed to the nephrostomy procedure due to entering the kidney accompanied by fluoroscopy during percutaneous nephrolithotomy surgeries. However, USG guidance makes performing this procedure a little different. With USG guidance, a 3.5 MHz convex abdominal probe is generally used for calyx entry. The operator attempts to use the probe to visualize the needle with one hand and also directs the needle toward the target calyx with the other hand. At this point, to visualize the needle and direct the needle according to the image on the screen requires serious USG experience and hand coordination. A study by Chalmers et al. reported that the chance of success of those with low incidence of nephrostomy insertion was very low. 7 As a result, in clinics where PN is not performed very often, radiologists and urologists avoid this procedure. However, the majority of urologists perform prostate biopsy with TRUSG guidance and are accustomed to working with this device and directing the needle. As our technique benefits from the same mechanism, any urologist who performs prostate biopsy can easily insert a nephrostomy with this technique. Independent of degree of dilatation, entry into the kidney with this method is possible as long as the target calyx can be observed. We routinely use this technique in our clinic and we do not have enough experience to insert PN by using the abdominal probe, especially with grade 1 hydronephrosis. The nearest center to perform nephrostomy placement is 200 km away. As a result, we do not have the luxury of choosing patients and we perform PN procedures with ∼100% success with this technique. In our clinical experience, urologists participating in the fellowship program at our clinic and without previous experience of nephrostomy insertion were observed to comfortably succeed in performing the nephrostomy procedure after a training program lasting a few days.
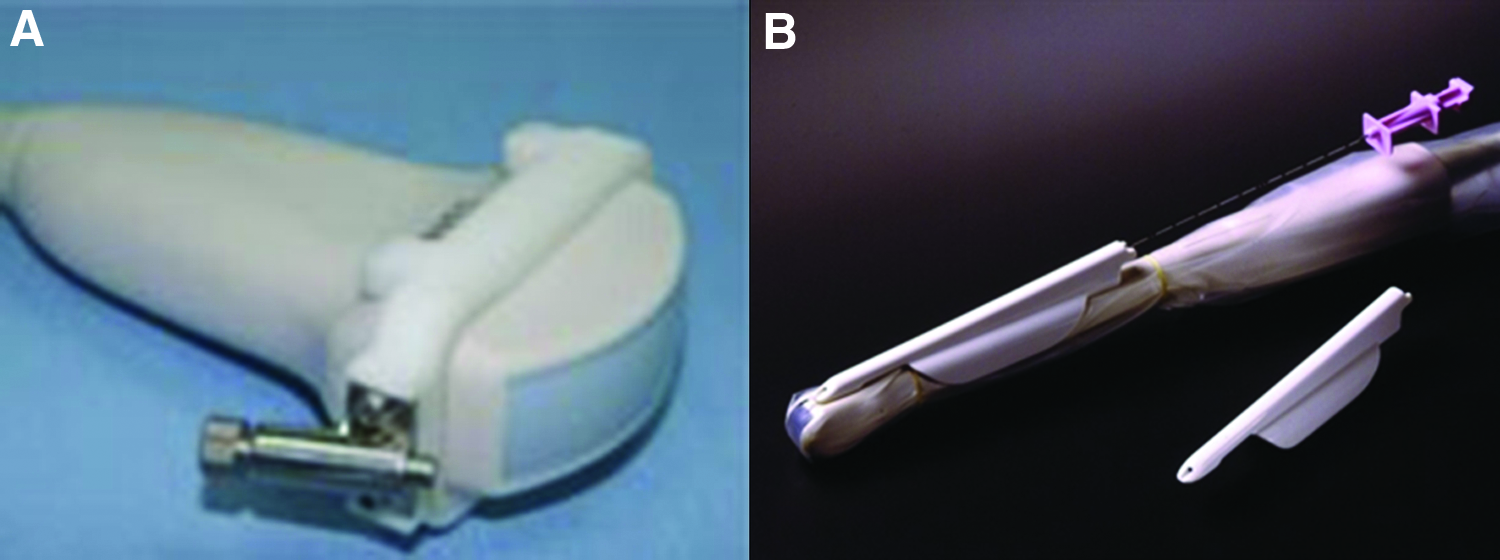
To ease insertion of nephrostomy with convex abdominal probe, an abdominal probe with a needle director is available (Fig. 3A). However, as the needle director attached to the abdominal probe has a directive channel of nearly 2-cm length, it is not sufficient to just hold it on the needle line. A slight movement of the needle causes it to move far from the targeted region. As a result, success rates are not very high. The needle director attached to a TRUSG probe has a channel length of nearly 11 cm (Fig. 3B). Due to the length of the channel, the needle is easily directed without deviating from the desired region. As a result, with our method, it is possible for the needle to enter the desired calyx as long as the location of the calyx is observed. We believe that this technique is a very simple and practical method for a urologist who knows how to perform prostate biopsy accompanied by TRUSG. With this method, we successfully inserted nephrostomy in nearly all our patients and we use this technique routinely in our clinic. In 3 patients with nephrostomy not inserted on the first attempt, the needle still entered the kidney and the guidewire was sent into the kidney. However due to agitation and movement of the patients, the guidewire was displaced from the kidney during tract dilatation, so the procedure was unsuccessful. These patients were given information about the procedure again, local anesthesia was more carefully administered, and nephrostomy was inserted the next day with the same method. We believe that the use of a single-entry nephrostomy set instead of the Seldinger method or sedoanalgesia for the procedure will aid in overcoming this problem. 11 In 1 patient, we could not perform nephrostomy placement with this technique. She had iatrogenic ureteral injury and no hydronephrosis. For this reason, we could not see the calyx with USG.
Mortality related to PN is reported to be as nearly as 0.3%. If severe hemorrhage or surgical intervention is required, it becomes 1%–3%. 12 A broad series was reported, including 1207 PN reported severe complication rates of 4%. 13 In our series, only 1 patient (0.68%) experienced Clavien grade 3 complications. In this patient, arteriovenous fistula developing after the procedure was treated with embolization. None of our other patients had severe complications requiring intervention.
One of the disadvantages of our method is that though clear images of surface organs are provided by the high frequency of the 6.5 MHz USG probe, there is low resolution of the remaining kidney at depth. As a result, kidney images are not as clear as those obtained with a 3.5 MHz probe. According to our experience, the distance between the renal calyx and skin is generally 5–8 cm from the posterior of the mid-axillary line. During the PN procedure, we observed that a 6.5 MHz TRUSG probe can easily visualize the required target calyx at this depth. After determining the target calyx, needle entry was performed. Some USG devices include a 3.5 MHz intracavitary probe. In places with this facility, the 3.5 MHz intracavitary probe may be used to obtain better imaging and perform the procedure. However, this is not definitely required for nephrostomy insertion. As body mass index (BMI) increases, the distance between the skin-calyx increases and USG image quality may reduce. Though BMI is not a definite criterion, it will not be possible to insert nephrostomy with this method in especially morbid obese patients where the target calyx cannot be observed. High quality and image resolution of the USG probe used or use of a 3.5 MHz intracavitary probe may further increase the chances of success.
An important point that requires care while using this method is that the procedure begins by examining the kidney with a 3.5 MHz convex abdominal probe. Assessment of the general structure of the kidney and calyx is important in determining the calyx with entry planned. If the procedure is begun directly with a TRUSG probe, there may be orientation difficulties experienced related to the kidney and calyx with entry planned. After transferring to the TRUSG probe, the section requiring most time is the stage of imaging the calyx. After the probe is placed in the appropriate region and the calyx is clearly observed, the only remaining item is to bring the calyx and guide lines on the screen into accordance and push the needle until the calyx is reached (Fig. 4).
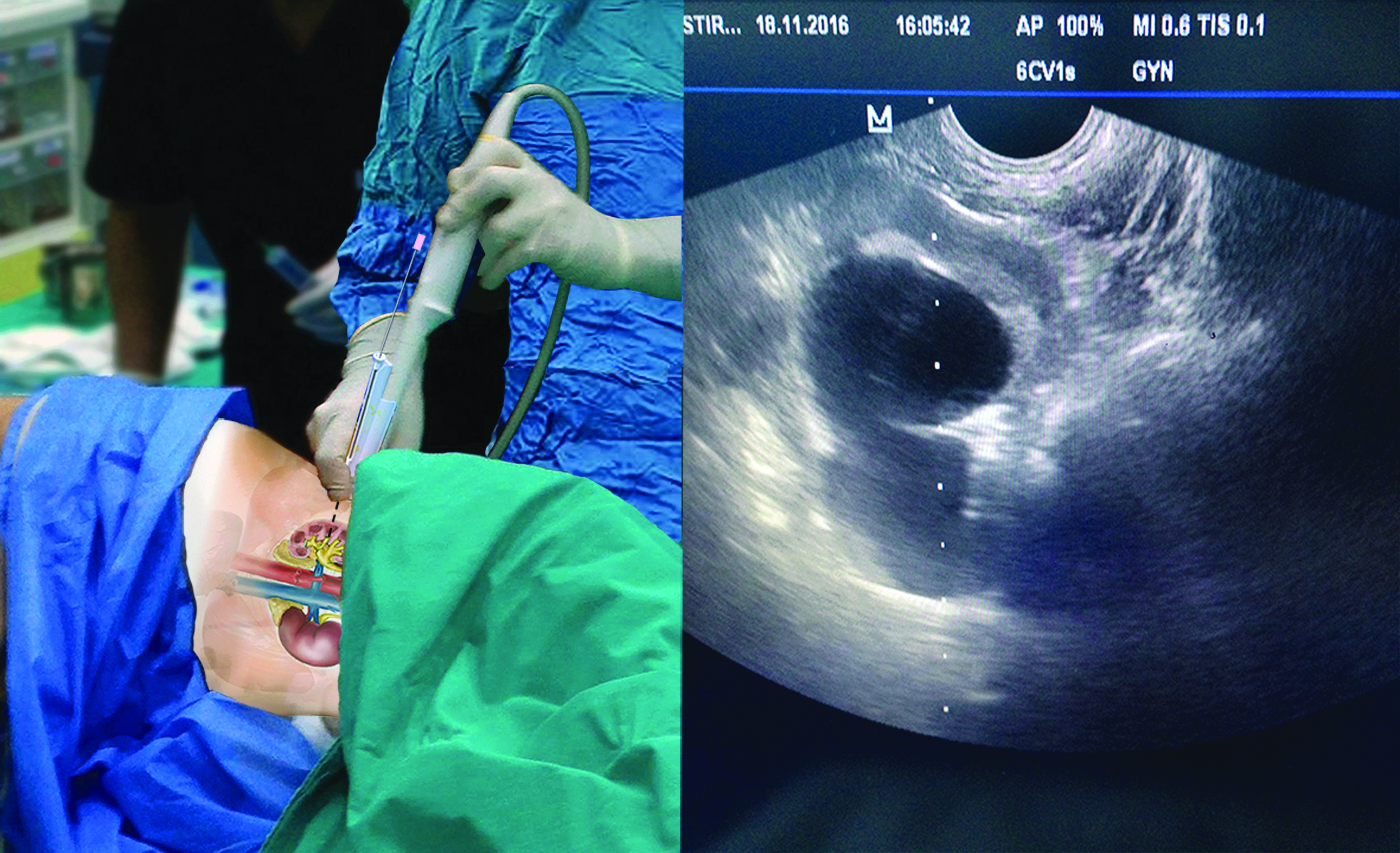
The schematic view of the needle insertion in the targeted calyx with a transrectal ultrasonography probe on the patient and the simultaneous ultrasonography image.
Another important topic during application is the stage where the needle enters the kidney. Generally, inexperienced operators will advance the needle very slowly and attempt to see the level of the needle tip on the screen. However, while in motion the needle tip and level should be clearly visualized. As a result, once the needle enters the skin it should be advanced without stopping. The level of the needle in motion should be followed on the USG screen, and it should advance without stopping or slowing until it is observed to have entered the collecting system. After entry into the kidney, it is not significant whether the guidewire rotates within the calyx or passes to the ureter. During dilatation, it is sufficient that the stiff portion remain between the skin and calyx so it does not displace or roll out of the kidney.
Conclusion
As placement of PN with an abdominal USG probe requires serious experience, it is not a procedure easily applied by every urologist. With our method using a TRUSG probe to insert nephrostomy, the PN procedure becomes much easier. For a urologist who knows how to perform prostate biopsy, it is a very easy method with a very short learning curve. We believe that this method will make PN application much easier and common in daily practice and in this way provide great advantages for patients.
Footnotes
Acknowledgments
The authors wish to thank Assistant Professor Ömer Atabeyoğlu who works in the Landscape Architecture Department of Ordu University for help in preparing the images.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.