
Abstract
Abstract
Purpose:
To compare the results of two- versus three-staged laparoscopic anorectoplasty (LARP) in children with rectoprostatic and bladder neck fistulas.
Materials and Methods:
The present study was retrospectively initiated among 32 consecutive patients who underwent two-staged LARP from October 2010 to December 2012. The associated defects, age at the operation, operative time, complications, length of the postoperative hospital stay, total hospitalization cost, and functional results (according to the Krickenbeck scoring system) were evaluated. The results were compared with those of 19 cases who underwent three-staged LARP from October 2008 to September 2010.
Results:
The average age at the second operation was 4.5 ± 1.2 months in the two-staged group, and 4.2 ± 1.3 months in the three-staged group. In the two-staged group, there were statistically shorter overall operative time and postoperative hospital stay duration. Also, a significantly lower total hospitalization cost was achieved. There was no anastomotic leak in either group. The rates of perineal wound infection, recurrent fistula, and rectal prolapse were 3.85% versus 0% (P = 1.000), 0% versus 5.3% (P = .422), and 11.5% versus 15.8% (P = .686), respectively (two-staged versus three-staged group). The median follow-up time was 67 (range, 54–80) months and 88 (range, 81–104) months, respectively. No significant difference in functional outcome was observed.
Conclusions:
Two-staged LARP is feasible, safe, and more cost-effective, with comparable incidences of complications and functional outcomes with respect to a three-staged procedure.
Introduction
Laparoscopic anorectoplasty (LARP) for patients with high anorectal malformations (ARMs) was first reported by Georgeson et al. in 2000. 1 This new technique, which can facilitate ideal visualization of the structures of deep pelvic cavity, precise placement of the rectum (or sigmoid colon) through the muscular complex, and cosmetic outcomes of abdominal wall, 2 became widespread soon after. Since 2004, LARP has been applied in our institution to treat rectoprostatic and bladder neck fistulas.
Initially, for the rectoprostatic and bladder neck fistulas, we utilized a three-staged procedure comprising a diverting colostomy right after diagnosis, anorectoplasty later, and finally, colostomy closure, as recommended by Peña in the posterior sagittal anorectoplasty (PSARP) approach. 3 In the minimally invasive era, there has been a trend among pediatric surgical centers to correct congenital anomalies at increasingly earlier age, and an increasing tendency to perform primary operation instead of staged procedures. 4
Nevertheless, for more complex cases requiring a distal colostogram to evaluate the malformations, or cases with delayed diagnosis, an initial colostomy is safer and more effective than a later colostomy. For these cases, there is an alternative two-staged procedure, using a colostomy before the main repair followed by stoma closure with simultaneous LARP within the next 6 months5,6 instead of a three-staged procedure.
Nonetheless, there are still concerns regarding the benefits and complications of this two-staged procedure. In this study, we aimed to compare the feasibility and outcome between two- and three-staged LARP.
Materials and Methods
Patients
The approval of the study was obtained from the Ethics Committee of the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (HUST). From September 2009 to October 2012, 32 consecutive neonates and infants with rectoprostatic and bladder neck fistulas (age range, 1 day–6 months; the associated defects are described in Table 1) were treated with colostomy and subsequent anorectoplasty under laparoscope combined with colostomy closure in the Pediatric Surgery Department of Union Hospital, Tongji Medical College, HUST. The divided colostomy was created at the transverse colon in 26 cases, while at the sigmoid colon in 6 cases. Nineteen patients who underwent three-staged LARP for rectoprostatic or bladder neck fistulas between October 2008 and September 2010 were included as the control group. Patients with rectal atresia, a history of premature birth, complex congenital heart defects, or tethered cord were excluded from this study. For all cases in both groups, the age at colostomy was 1–5 days, while the age at LARP was between 3 and 6 months. The associated defects, age at the operation, operative time, length of postoperative hospital stay, as well as perioperative complications (including anastomotic leakage, perineal wound infection, recurrent fistula, and rectal prolapse), total hospitalization cost, and functional outcomes (using the Krickenbeck scoring system), were recorded.
Distribution of Associated Defects
LARP, laparoscopic anorectoplasty.
Surgical procedures
All cases were operated on by the same surgeon but with different assistants.
Laparoscopic colostomy
After general anesthesia was induced, the laparoscope and minimally invasive instruments were introduced. A loop of transverse colon or sigmoid colon was identified under a laparoscope. A colostomy was made using a double-barreled technique creating an about 3-cm-high chimney above the skin with the colon loop separated completely. Simultaneously, the proximal end was put slightly lower than the half-closed distal end. The bowel was sutured to the peritoneum with 5-0 absorbable stitches interruptedly. To avoid peristoma adhesions, a polylactic acid antiadhesive barrier film was placed. Distal colon enema was done using warm saline through a suction tube (usually three episodes needed).
Two-staged LARP
At 3–6 months, the stoma was closed using end-to-end anastomosis. At the meantime, LARP was performed using a three-port technique, including one port in the colostomy site. The muscle stimulator was applied to detect the center of the muscular complex (Fig. 1). Under the laparoscope, a 3-mm trocar was introduced between the contraction center and the puborectalis muscle to form a tunnel through the pelvic floor (Fig. 2). Then, the pelvic tunnel was enlarged using anal dilators gradually up to a 14 mm size. The distal end of the rectum was pulled down through the neo-tunnel, and was fixed to the perineal skin. The wound was repeatedly washed with warm saline and 0.5% iodine before being closed. An anorectal tube was maintained in situ until regular bowel movements occurred (optimal duration is 2–3 days after surgery). Intravenous antibiotic administration was started in the operating room and typically lasted for 48 hours postoperatively. Patients were allowed to drink water 6 hours after surgery. If tolerated, on the first postoperative day, patients were offered an enteral nutrition preparation and later gradually transitioned to a normal diet in 3–6 days. Postoperative perineum nursing care was provided to keep the anastomoses clean and dry. All patients were examined 2 weeks after LARP, and then an anal dilation program was started.
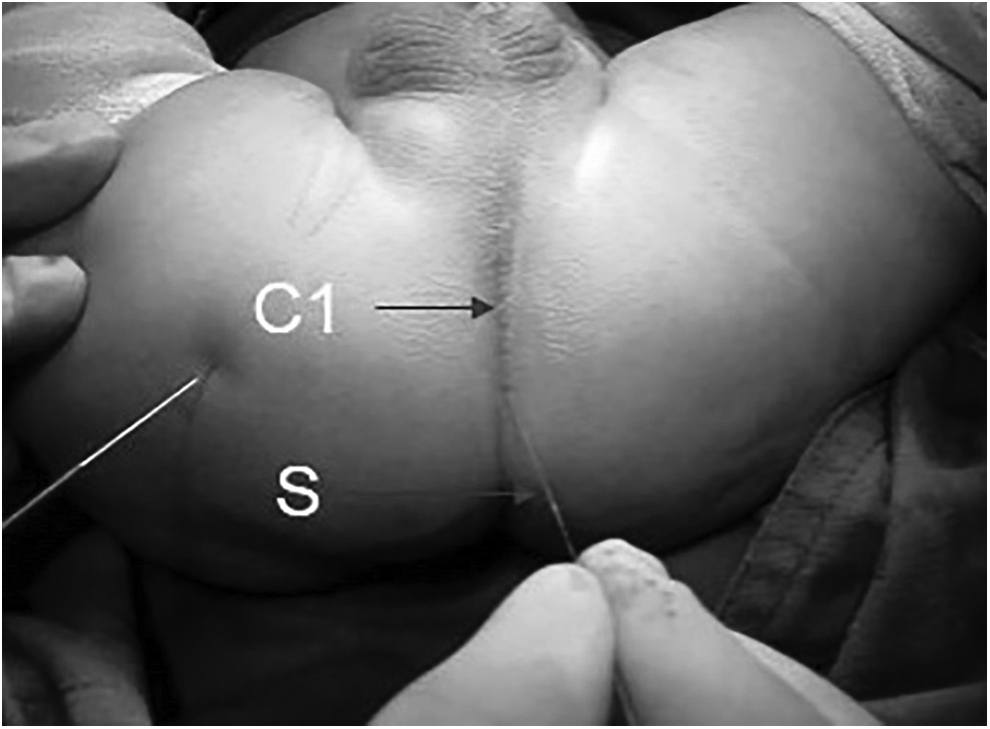
The center of the levator ani muscle sling was detected using the muscle stimulator. C1, the muscle contraction center; S, the muscle stimulator.
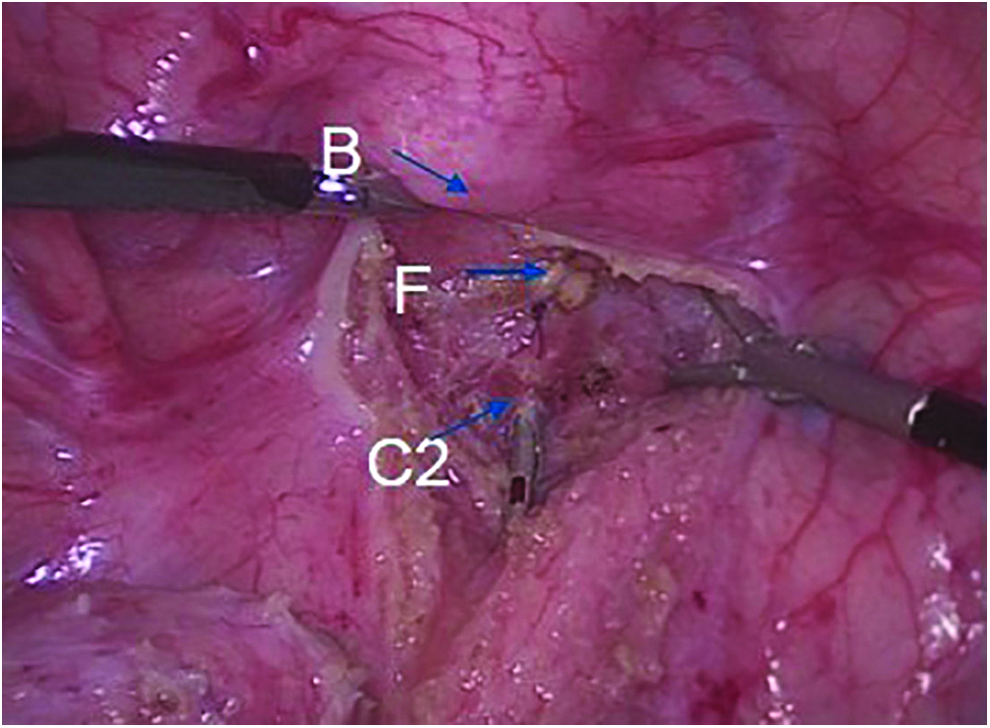
Under the guidance of a laparoscope, a 3-mm trocar was inserted between the muscle contraction center and the puborectalis muscle to form the pelvic floor channel. B, the bladder; C2, the puborectalis muscle; F, the fistula.
Three-staged LARP
A temporary colostomy in a divided double-barreled manner was created at 1–5 days of age, followed by anorectoplasty at 3–6 months. Approximately 1 month after anorectoplasty, the colostomy was closed.
Dilatation protocol
Patients underwent anal dilation strictly according to Peña's protocol. 7 Two weeks after anorectoplasty, the patient's family would be taught the anal dilatation procedure. The initial size of the dilator would be determined by the surgeon after digital rectal examination, and the procedure would be demonstrated to the parents. Dilatation usually began with a 7 or 8 mm dilator that was not even felt by the patient. The parents must undertake the dilatation once a day, leaving the dilator inside for 30 seconds at the beginning. The size of the dilator was supposed to increase every week, until attaining the adequate size, agreeing with the patient's age (Table 2). All the dilation processes are done without anesthesia in our institution.
Adequate Size of Dilators According to Age
Follow-up
Postoperative follow-up was conducted at 1, 3, and 12 months and every year thereafter. The bowel symptoms that were recorded included voluntary bowel movements, frequency of fecal soiling, and constipation, and anorectal function outcomes were scored in patients older than 5 years by the Krickenbeck scoring system (Table 3). 8
Functional Results According to Krickenbeck Scoring System
PBN, P value only for bladder neck fistula patients between two groups; PRP, P value only for rectoprostatic fistula patients between two groups; PT, P value between two groups.
Statistical analyses
A retrospective analysis of the 51 patients was performed, as shown in Table 4.
Outcomes of Two-Staged and Three-Staged Laparoscopic Anorectoplasty
LARP, laparoscopic anorectoplasty.
Using the Krickenbeck scale, the outcomes of the two groups were collected and analyzed in patients older than 5 years (Table 3).
All statistical analyses were performed using SPSS version 20.0 (SPSS, Inc., Chicago, IL). Student's t-test was applied to compare the operative times, hospital stays, and costs between the two groups, and the χ2 test and Fisher's exact test were utilized for proportional data. P value <.05 was considered statistically significant.
Results
Two-staged LARP was performed successfully in all these 32 cases with rectoprostatic or bladder neck fistulas, with no conversion to laparotomy. The bowel loop of the transverse colon was brought out safely through the opening in 26 patients, while laparoscope guidance was needed in 6 cases to identify the sigmoid colon. Regarding the postoperative complications, rectal prolapse occurred in 3 cases in both groups, which was moderate or evident according to Brisighelli's classification. 9 No parastomal hernias or obstructive symptoms were observed in either group. Perineal wound infection was observed in 1 patient (healed without surgical intervention) in the two-staged group, while there was none in the three-staged group. No fecal impactions, urinary tract infections, posterior urethral diverticulum, or colonic anastomotic leakages were found in either group. The average overall operative time for the patients was 236.7 ± 21.3 minutes (280.5 ± 17.1 minutes in the three-staged group, P < .001). The average overall duration of hospital stay was 13.9 ± 1.4 days (20.8 ± 2.2 days in the three-staged group, P < .001). The total hospital costs were the sum of all medical expenses during the two (two stages) or three times (three stages) of hospitalization. It was significantly lower in the two-staged group ($7206.3 ± 387.0 versus $9743.4 ± 699.3, P < .001).
Unfortunately, the bladder neck fistula recurred in 1 case in the three-staged group. Its colostomy was done 3 days after birth at transverse colon. Three months later, the patient underwent LARP. During the operation, the fistula was identified well and was closed by hemolock. Four days after anorectoplasty, urine exuded through the drainage in the pelvic cavity. The contrast medium effusion was identified by cystourethrography. Continuous catheterization combined with intravenous antibiotic therapy was administered for 2 weeks. Cystourethrography was done before the drainage and urine catheter removal.
Functional results of the patients were evaluated after the patient became 5 years. The age difference was analyzed and no significance was found between two groups. According to the Krickenbeck scoring system, no differences were observed with respect to voluntary bowel movements (P = 1.000), soiling (P = .906), or constipation (P = .913) between these two groups.
Discussion
With accumulation of experience and advances in minimally invasive technology, there has been an increasing trend toward performing primary operations instead of staged procedures over the past two decades. For example, among most children with Hirschsprung's disease, the surgical plan has changed from three-staged procedures to a single-staged primary pull-through in most cases, as single-staged operations have been proven to be safe and cost-effective in both neonates and infants.10,11 The same effect is seen in the ARM treatment strategy.1,12,13 Traditionally, three-staged operations are recommended for patients with rectoprostatic and bladder neck fistulas. In Georgeson's initial report, 4 of 11 patients underwent primary repair in a minimally invasive manner, while the other 7 patients underwent two-staged procedures.
Although it remains controversial whether LARP provided better functional outcomes than PSARP, LARP achieves more accurate bowel placement through the pelvic floor, resulting in smaller abdominal and perineal wounds and avoiding the complete division of the muscular complex. 2 Accordingly, LARP achieves faster recovery, shorter hospital stay, and fewer wound complications.13–16 In 2015, Bischoff et al. reviewed 68 articles that included 622 cases operated using laparoscopy. 17 There is no final conclusion showing that the morbidity of rectal prolapse is higher in LARP than it is in PSARP. One study from Japan even reported a much higher rate (67%) of mucosal prolapse in PSARP than it was in LARP (0%). 18 No posterior urethral diverticulum occurred in our study sample. According to the literature and our experience, excessive dissection of the rectum, mucosal remnant, ignorance of anchoring stitches, sphincter dysplasia, postoperative constipation, and oversized anal opening (optimally 1.2–1.5 cm) may contribute to this complication. 19
Generally, stoma closure after main repair was considered crucial for the management of rectoprostatic and bladder neck fistulas to prevent perineal wound infections by fecal diversion and to ensure good anal function. However, our study did not show any increase in infections or worsened functional results from two-staged LARP, in which a colostomy was performed first, followed by stoma closure and simultaneous LARP.
Possible reasons for this finding are listed as follows:
First, advances in medical technology and an improved understanding of health care can lead to faster recovery from diseases, as well as decreased discomfort during perioperative period. The use of laparoscopy in intestinal resection may further facilitate postoperative recovery. 20 In addition, laparoscopic anorectal pull-through causes less trauma to the perineum (only ∼1 cm in length), where the sphincteric channel is gradually dilated rather than completely split and reconstructed, as is the case in PSARP. The less invasive wounds allow promotion of soft tissue restoration, thus reducing the incidence of wound infections. Even if infection of the small perineal incision occurs, the effects would be superficial.
Second, several studies reported that older age was an independent risk associated with infectious complications in stoma closure or definitive bowel resection,21,22 although the specific reasons were not identified. In our study cohort, all patients underwent LARP before 6 months of age and, as a result, most recovered without postoperative infectious events.
Third, patients were allowed to drink water 6 hours after surgery. If tolerated, on the first postoperative day, patients were offered enteral nutrition preparation and later were gradually transitioned to normal diet in 3–6 days. This protocol was adapted from the concept of enhanced rapid recovery surgery. 23 The oral administration of enteral nutrition preparations, called “no-residue diets,” improves postoperative nutritional conditions, diminishes fecal transit times and volumes effectively, and strengthens the immune system and thus reducing the risk of developing infections. 24
In addition, well-defined MRI assessment, better laparoscopic views, and muscle stimulation (as described previously 2 ) enabled the construction of an accurate pull-through tunnel and prevented urethral or nerve injuries, thereby ensuring good functional outcomes.
Nevertheless, a colostomy before main repair gives time for physical development in special cases. Simultaneous stoma closure and LARP prevent repeat anesthesia and shorten the entire recovery period. As a result, the overall costs are definitely reduced.
In this study, there was a longer hospital stay than reported by many other centers. There was a total hospital stay of 13.9 (5 + 8.9) days in the two-staged group, while it was 20 (5 + 7 + 8) days in three-staged group. In China, there is a heavy lack of pediatric knowledge in community medical care system. The patients must be able to eat and defecate normally, and furthermore, the incision must heal well before they could be discharged.
However, there are several limitations in this study. The number of cases was relatively small. The average age at the time of evaluation in the two-staged group was slightly younger than that in the three-staged group. In addition, this study was not a multicenter prospective randomized study. Furthermore, there was a methodological problem that the three-staged approach cases were done before the two-staged cases. Conceivably, the surgeon could have had more experience when doing the two-staged approach and therefore having obtained better results.
In conclusion, we recommend two-staged LARP, first with colostomy, followed by stoma closure combined with pull-through at the second stage, for rectoprostatic and bladder neck fistula repair. This approach reduces the risks of additional operations and eases the economic burdens of the patients. Moreover, there is no increase in the morbidity rate of postoperative complications. Furthermore, the functional outcomes are equivalent to those of three-staged LARP.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The present research was supported by funding from the National Natural Science Foundation of China (No. 81700497) and special funds from the National Health and Family Planning of China for the Public Welfare Research (No. 201402007).