
Abstract
Abstract
Introduction and objectives:
This study assessed the diagnostic protocol and the outcomes of laparoscopic aberrant hepatic duct (AHD) reconstruction in choledochal cyst (CC) surgery.
Methods:
From January 2010 to January 2018, 275 laparoscopic CC excisions were conducted in our hospital. Seven patients of CC with associated AHD were recorded. AHDs that drained into the cystic duct were anastomosed to the Roux-en-Y loop. Clinical data of these 7 patients were retrospectively analyzed.
Results:
AHD is classified into four types according to the literature. The type where AHD drains into the cystic duct is the most commonly encountered one. The incidence of this type was 2.5% (7/275) in our series. Preoperative examination included magnetic resonance cholangiopancreatography (MRCP) (5 patients) and computed tomography (CT) scan (2 patients). Suspected AHD was diagnosed preoperatively in 4 out of the 5 patients who underwent MRCP. For the 2 patients who underwent CT scan only, AHD was not detected preoperatively. AHD was verified intraoperatively for all the 4 patients who had suspected diagnosis. Among them, AHD was well preserved in 3 patients, but damaged at exploration in the remaining 1. For the remaining 3 patients without preoperative AHD diagnosis, bile leakage was detected intraoperatively. Ductoplasty of the AHD with common hepatic duct was performed in 3 patients, and AHD was incorporated into the Roux-en-Y jejunal loop separately in 4 patients. Laparoscopic surgical procedures were completed in 6 of the 7 patients in this study, while 1 patient was converted into an open procedure. Postoperative recovery was uneventful in all patients. The duration of follow-up ranged from 6 months to 4 years (median 2 years) with no complication encountered.
Conclusions:
Routine preoperative MRCP examination of CC is recommended to detect variations of biliary tree. The laparoscopic approach is a feasible option in the experienced hands.
Background and Purpose
In general, the normal common hepatic duct (CHD) is formed by the confluence of the right and left hepatic ducts. Variations in the anatomy of the biliary tree are quite common. The incidence of variations of the biliary tree was found to be 14%–28% in autopsy series 1 and 19% (98 patients) in a series of 513 intraoperative cholangiograms. 2
Aberrant hepatic duct (AHD) is of surgical significance because it usually constitutes a factor of biliary injury during operation. The reported incidence of AHD varies from 1.0% to 31.4%. 3 In Kullman et al.'s report, 2 the incidence of AHD was found to be 8.4%, with AHD draining into the cystic duct in 3.1% (16 patients). Obviously, AHD associated with CDC is a rare condition. Only a few reports about CDC with AHD have been published.4–7 Takahashi et al. 6 reviewed the literature in 2008 and found only 5 patients of AHD before his patient report. Mistreatment of AHD may result in serious complications. 6 Obviously, although the incidence of AHD is rare, its surgical significance cannot be ignored.
Choledochal cyst (CC) excision with reconstruction of the AHD is considered a challenging surgical procedure. Although laparoscopic radical excision of CC and biliary enteral reconstruction is widely accepted, 8 reports on laparoscopic AHD reconstruction are rare.
This study aimed to assess the diagnostic protocol, the feasibility, and the outcomes of laparoscopic AHD reconstruction in CC surgery.
Materials and Methods
From January 2010 to January 2018, 275 laparoscopic CC excisions were performed in our hospital. Upon approval by the ethical committees of GWCMC, a retrospective record review identified that 7 patients of CC associated with AHD draining into the cystic duct were encountered, and all underwent AHD reconstruction. All patients were treated with the institutional standard of care. Informed consent was obtained before any operation.
Data of the 7 patients are shown in Table 1.
Characteristics of Patients of Choledochal Cyst with Aberrant Hepatic Duct
AHD, aberrant hepatic duct; CT, computed tomography; LP, laparoscope; MRCP, magnetic resonance cholangiopancreatography; US, ultrasound.
Preoperative examination
Ultrasonography followed by magnetic resonance cholangiopancreatography (MRCP) were routinely performed preoperatively for CCs in our hospital. Additionally, intraoperative cholangiography (IOC) was performed if the preoperative MRCP images were unclear, especially when the pancreaticobiliary duct junction or suspected intrahepatic duct stenosis could not be clearly visualized, or a suspected AHD needed to be verified. For patients referred from other hospitals with computed tomography (CT) only, MRCP would be offered and performed depending on patient's preference.
Operative procedure
Laparoscopic CC excision was described in our previous report. 9 Briefly, (1) four trocars were placed in the umbilicus, right hypochondrium, right side of the abdomen, and left hypochondrium, respectively. (2) The cyst was dissected down to the distal tapered end of the common bile duct, followed by ligation. The upper part of the cyst was further dissected up to the normal CHD and transected at that level. (3) A Roux-en-Y anastomosis was performed outside the abdominal cavity by exteriorization of the small bowel via the enlarged umbilical incision. (4) A retrocolic end-to-side hepaticojejunostomy was carried out laparoscopically, suturing the posterior wall first and then the anterior wall with continuous 5-0 or 6-0 PDS. (5) When CHD stenosis was encountered in Todani IVa type patients, a simple resection or ductoplasty was performed by a longitudinal incision along the anterior wall of the stenosis, followed by additional cholangioenterostomy. (6) An eventual AHD was then incorporated into the biliaryjejunal anastomosis. No AHD was ligated in these 7 patients.
AHD reconstruction with the Roux-en-Y jejunal loop was completed with one of two approaches, as shown in Figure 1, depending on the distance between the AHD and CHD. One approach was to join the AHD and CHD opening together to form a single stoma and anastomose with a Roux-en-Y jejunal loop, when the AHD and CHD were in a close position with no tension after suturing. The other way was to incorporate the AHD and CHD separately into the Roux-en-Y loop, when the AHD was far away from the CHD, and both ducts could not be approximated. Besides, when an AHD was suspected to drain into the cystic duct in preoperative MRCP, the anterior wall of the cystic duct was incised to locate the orifice of the duct. After the orifice of the AHD was identified, the margin patch of the AHD was utilized to enlarge the anastomosis, preventing future stricture. When the AHD was damaged accidently and the orifice patch could not be reserved, the anterior wall of the duct was incised to create a wider stoma for a larger anastomosis.
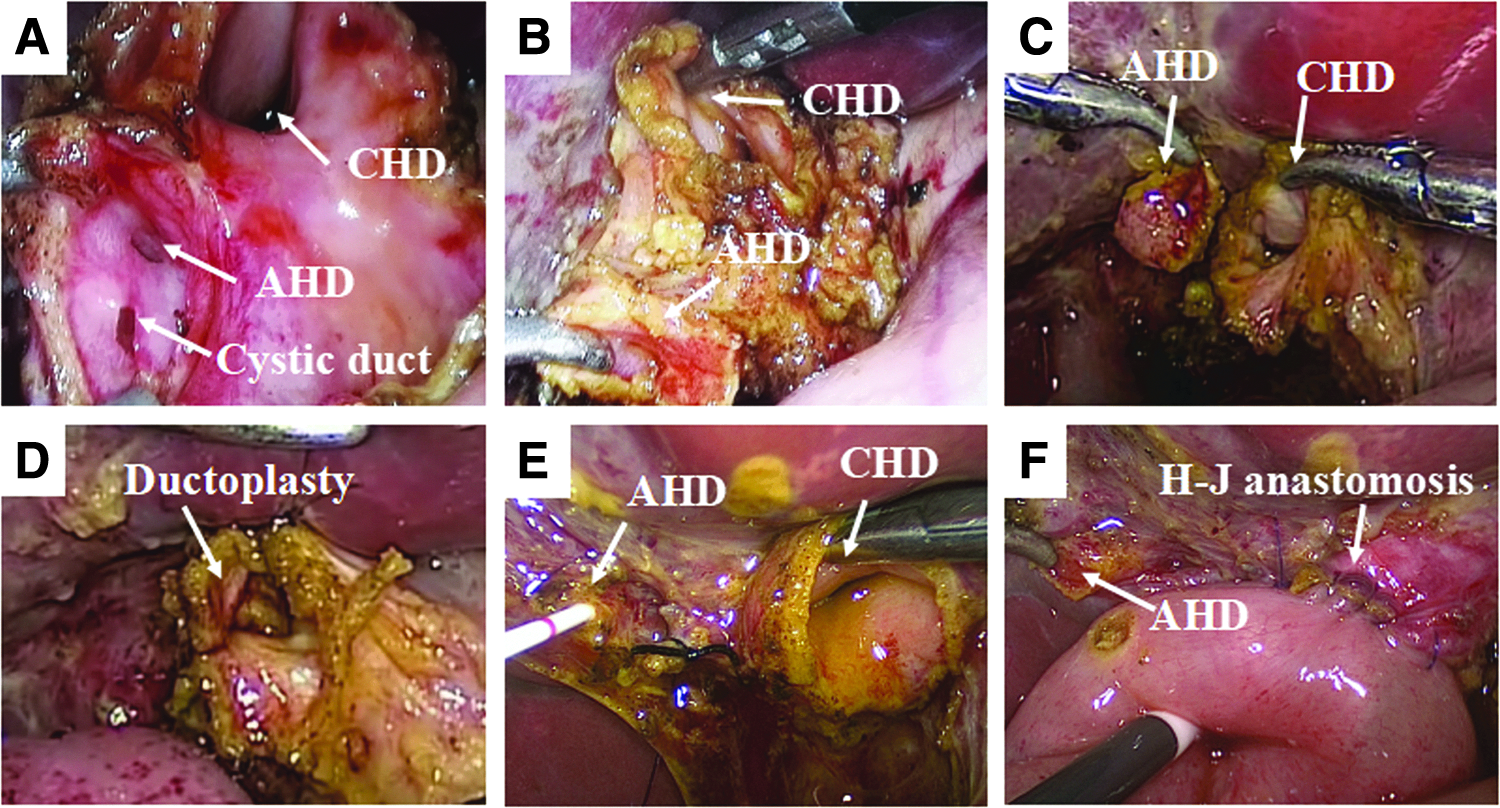
Surgical procedures.
Follow-up protocol
The follow-up protocol looked into (1) clinical symptoms (abdominal pain and jaundice); (2) liver function test (especially conjugated bilirubin, transaminase, gamma-glutamyl transpeptidase); (3) ultrasonography for assessing progressive intrahepatic bile duct dilatation or hepaticolithiasis; and (4) MRCP to delineate the biliary tree structure and anastomosis.
Results
The study population consisted of 275 consecutive pediatric patients with CCs who underwent minimally invasive laparoscopic cyst excision and Roux-en-Y hepaticojejunostomy between January 2010 and January 2018 in a pediatric medical center in south China. Among the 275 patients, 7 CC with AHD were identified and operated on. Aberrant ducts in all the 7 patients were incorporated into biliary-enteric anastomosis, and none was ligated.
Preoperative MRCP was performed in 5 patients (5/7); the remaining 2 patients underwent CT scan only before referral to our hospital. With preoperative MRCP, a suspected AHD was detected in 4 of the 5 patients (patients 2, 3, 6, and 7) (Fig. 2), while no suggestion of AHD could be found in the remaining 1 patient (patient 1). With CT scan alone, the preoperative detection of AHD was missed in 2 CC patients (patients 4 and 5). Four patients with possible AHD findings in MRCP were all verified in the operation. In 3 patients, AHD was successfully identified and well reserved during operation (patients 2, 3, and 7), while the remaining AHD was inadvertently damaged during exploration (patient 6). In all the other 3 patients with no suspected AHD before operation, AHD was identified only when bile leakage was detected after aberrant duct damage (patients 1, 4, and 5).
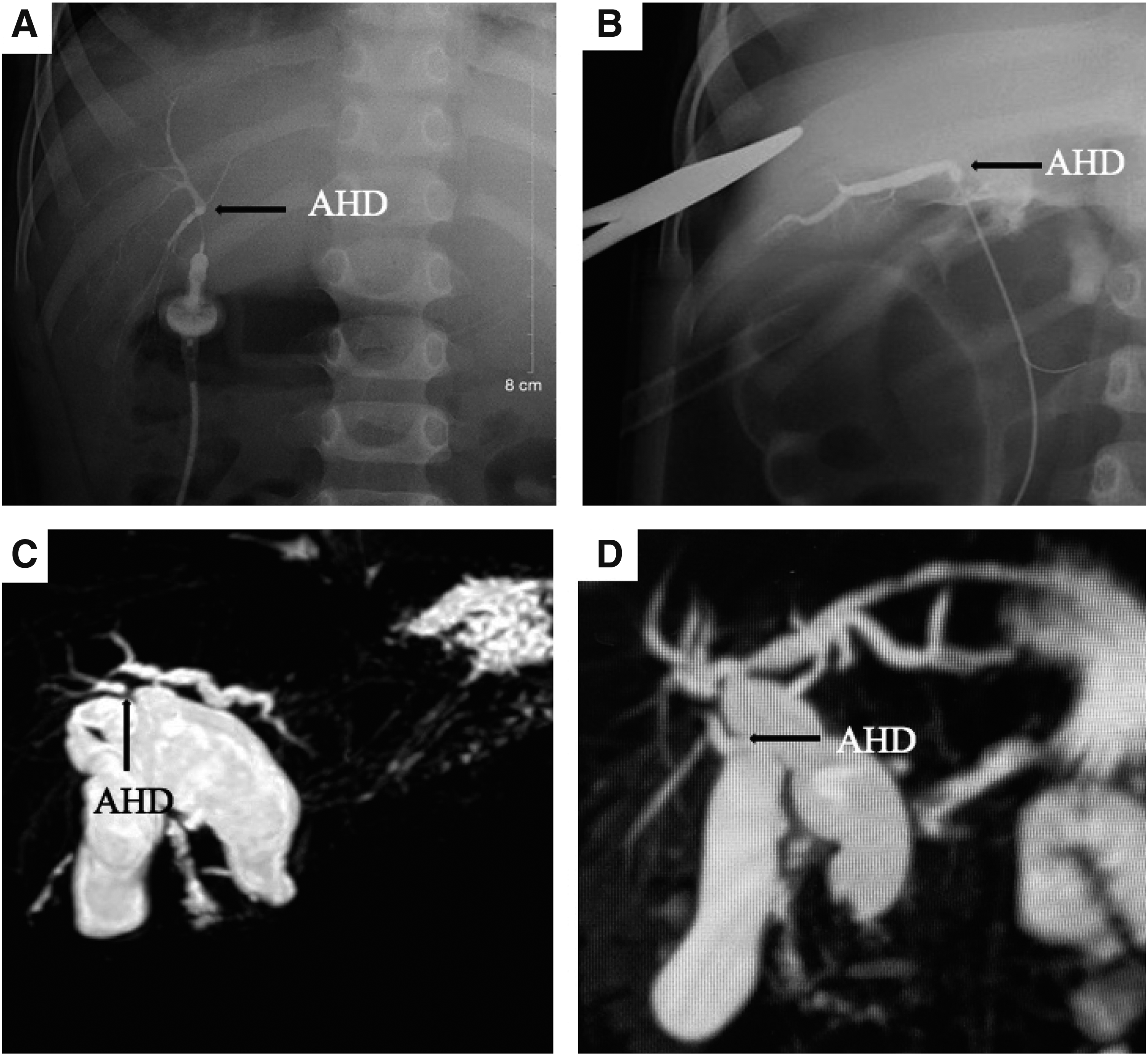
IOC and preoperative MRCP.
Depending on the distance between the AHD and CHD, 3 AHDs were anastomosed with the CHD first to create a common channel, and then incorporated into the jejunal loop, while the other 4 AHDs were anastomosed to the jejunal loop individually.
The postoperative course was smooth in all 6 patients. They were discharged uneventfully 6–7 days after surgery. Patient 2 developed chylous peritonitis on postoperative day 3 and settled spontaneously after 38 days of conservative therapy.
All 7 patients were followed up regularly. The duration of follow-up ranged from 6 months to 4 years (median 2 years). No patients had abdominal pain or jaundice. All patients had normal liver function tests. Ultrasonography revealed no intrahepatic duct dilatation or atrophic changes of the liver. Four postoperative MRCP showed no evidence of dilation of the intrahepatic duct secondary to AHD reconstruction as shown in Figure 3.
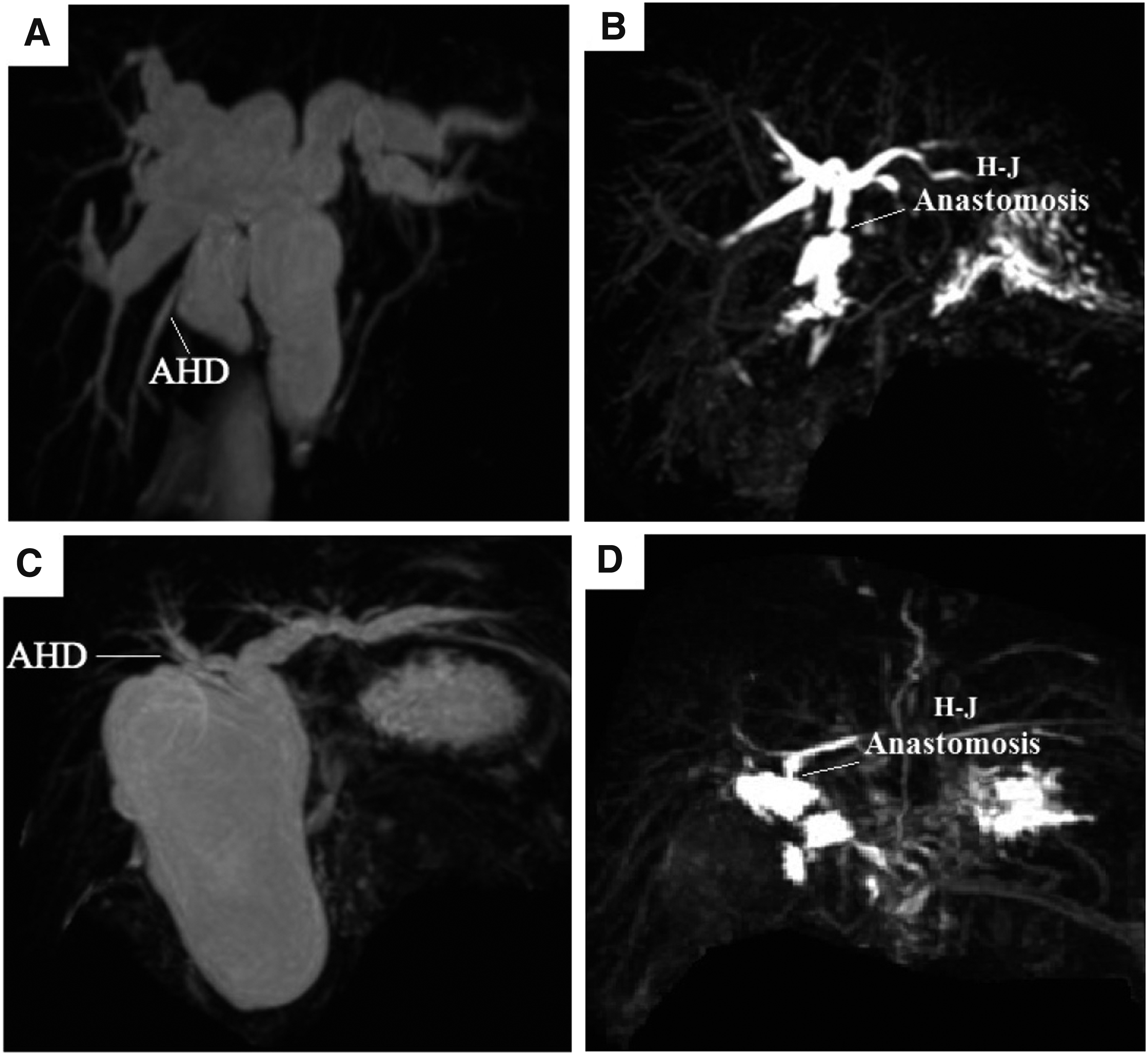
Preoperative and postoperative MRCP in patient 6
Discussion
Terminology and classification of AHD
CC, also known as choledochal malformation or congenital choledochal dilatation, is a major disease in the field of hepaticobiliary surgery in pediatric patients. 10 Aberrant bile duct accompanied with CC is a rare condition. The terms aberrant bile duct and accessory bile duct are the two commonly used descriptions for variations of the biliary tree. By definition, these are quite different identities. An aberrant bile duct, which does not communicate with other biliary segments, is the only bile duct draining a particular segment of the liver, whereas an accessory bile duct, which intercommunicates with other biliary segments, is an additional bile duct draining the same area of the liver. According to the definition, if an aberrant duct is ligated, the specific part of the liver drained by the duct would be obstructed, and atrophic changes would occur afterward. However, these two terms are used interchangeably in the literature,3–6 because the communication between the variant bile duct and the normal duct is not routinely identified.
AHD can be classified into four types according to the site of communication with the bile duct: (1) AHD draining directly into the gallbladder, (2) AHD draining directly into the cystic duct, (3) AHD draining directly into the CHD from the right or left side, and (4) AHD draining directly into the common bile duct. 3
AHD incidence
Our report includes the largest number of patients of CC with AHD. In our series of Chinese patients, the incidence of AHD draining into the cystic duct was 2.5% (7/275), corroborating previous findings1,3 No type IV was found in the 275 patients. The other types of AHD associated with CC, such as types I and III that are not of surgical relevance, were excluded from our series. Therefore, the total incidence of all types of AHD was not calculated in this study. As for the relationship between the CDC and AHD, our data support the assertion of Duh et al. that there is no direct relationship between the presence of a CC and an AHD. Indeed, AHD could be a coincidental finding. 4
Need for AHD reconstruction
In CC surgery, surgical invention is not necessary for types I and III. The first type, which is also called Luschka duct, is often very tiny in pediatric patients and can be dissected with cautery directly. For type III in which the AHD drains into the CHD, the CC could be transected distal to the AHD opening, and the cystic duct should be dissected closely along its wall to avoid AHD injury. Only types II and IV, in which the AHD drains into the cystic duct or the common bile duct, are of surgical relevance in CC excision. Type IV AHD with CC is quite rare, and only 1 patient has been reported in the literature. 6 In our series, no type IV was found, and only type II with AHD draining into the cystic duct was encountered, for which surgical management was necessary.
Ligation of an aberrant bile duct may result in atrophy of the definitive obstructed segment, with potential deleterious effects on pediatric patients with a CC. Sometimes, bile leakage may occur after simple ligation because of the raised pressure of the ligated intrahepatic duct. Therefore, for AHD treatment, bile duct reconstruction is a more reasonable approach.
In adult patients, it is recommended that the AHD should be anastomosed when the diameter of the duct exceeds 2 mm as it may drain a large liver segment. In the first and sixth patients in our series, although the AHD diameter was about 1 mm, IOC images showed that it drained the right-posterior segment of the liver. So, it is obvious that this standard of 2 mm cannot be applied to pediatric patients because of their small body size. Reconstructive surgery is recommended in such circumstance.
Role of preoperative examination in detecting an AHD
The anatomic feature of the biliary tree is important for the surgeon in performing a hepatobiliary operation. Undoubtedly, for a CC, preoperative diagnosis of AHD is helpful in preventing postoperative complications, such as bile leakage and recurrent cholangitis due to AHD injuries. 6 There are various approaches that can be employed to delineate the anatomy of the biliary tree. In the literature, AHD has been identified by IOC, endoscopic retrograde cholangio-pancreatography (ERCP), intraoperative endoscopy, or MRCP6,11–13 before or during operation. Intraoperative cholangiography, first introduced by Mirizzi in 1932, is a widely used and reliable method for detecting variations of the biliary tract. 14 In Lal's study of a series of CC patients, 12 3 of 4 aberrant biliary ducts were missed by IOC conducted before cyst excision. For CCs, AHD may occasionally be missed on IOC because of overlap by a huge dilated cyst. In our series, IOC only was used in 2 of the 7 patients to verify the AHD after bile leakage was found.
Some authors recommend MRCP as a reliable approach for identifying the AHD before operation.1,11,12 In Lal's series, MRCP accurately delineated 10 out of 13 AHDs before surgery. 11 In our study, MRCP was performed in 5 of the 7 patients before CC excision. According to MRCP images, 4 of the 5 patients were suspected of possible AHD, all of which were confirmed in the operation. A suspicious diagnosis reminds the surgeons of a possible AHD, and great care should be taken during exploration and dissection to avoid iatrogenic injury. Meanwhile, no evidence of an AHD on MRCP images was found in the first patient, in which the diameter of the intrahepatic duct was quite small and it was hard to be clearly visualized using MRCP. MRCP is a preferable examination for most CC patients; it not only could provide information about the CC but also reveals the cyst type, as well as the anomalous junction of the pancreaticobiliary duct and the AHD. However, for patients whose bile ducts are quite small without dilation, AHD or some other variations of the biliary tree may not be evident on MRCP. Furthermore, preoperative AHD diagnosis is only a speculation due to the current MRCP technical limitation; sometimes, the image of bile duct may appear to be interrupted, as in patient 3. It is hard to decide whether it is exactly a duct connected to the cystic duct or other part of the biliary tree. Although preoperative diagnosis of the bile duct variation sometimes is only suggestive, it is still useful for the operation. So, MRCP is regarded as a routine examination for CC patients in our hospital, and the MRCP images would be carefully read for each patient to explore any biliary duct variation.
Detecting AHD during operation
Most AHDs in pediatric patients are quite small; for those with no preoperative AHD diagnosis, the AHD was liable to be damaged intraoperatively. Even in patients with a possible diagnosis of AHD before surgery, a great care is needed during operation. In patient 6, AHD was damaged because of its marked displacement by the dilated CC and severe adhesion after repeated inflammation. Because of the small size of the AHD, the reservation of the orifice patch of the tiny AHD is quite helpful to the reconstruction procedure. Therefore, in our series, when a possible diagnosis of AHD was established by MRCP, a careful exploration of the inner aspect of the CHD followed by dissecting the anterior wall of the cystic duct has become a routine procedure for detecting possible AHD. With this approach, 3 patients with AHD were successfully detected, and the orifice patch was preserved for bile duct reconstruction.
Methods of biliary reconstruction and prevention of related complications
According to the distance between the AHD and CHD, two approaches can be employed for biliary reconstruction: the AHD is anastomosed with CHD to create a common channel first, followed by biliojejunal anastomosis; alternatively, the AHD is anastomosed to the Roux-en-Y jejunal loop separately. In this study, the first method was used in 3 patients and the second in the remaining 4. Usually, the AHD is small in size, mostly <2 mm in diameter. If the AHD is transected accidentally during operation, incision on the anterior wall of the AHD is necessary to enlarge the orifice for a wider anastomosis to prevent postoperative stricture. For patient 6 in this series, the diameter of the damaged AHD was only 1 mm. After successful incision of the anterior wall of the duct, the diameter was enlarged to about 2.5 mm, facilitating further anastomosis. If the AHD orifice can be identified after opening the anterior wall of the cystic duct, the margin patch is reserved to enlarge the anastomosis stoma. This renders the anastomosis easier and constitutes an effective way to prevent anastomosis stricture.
With the development of the laparoscopic technique, more demanding conditions could be dealt with now, that is, reconstruction of the common, left, or right bile duct stricture followed by hepatojejunostomy. 8 Under laparoscopic magnification, it is easy to complete a more meticulous manipulation. To the best of our knowledge, this is the first report on the laparoscopic management of CC associated with AHD. The meticulous AHD reconstruction is a technical challenge, and the related complication of bile leakage after reconstruction in open surgery has been reported in the literature.6,12 Fortunately, in this series, 6 of the 7 patients were successfully operated on laparoscopically, and the remaining 1 by conversion to open operation, with minimal postoperative complication. The postoperative course of the 6 patients were uneventful. The postoperative chylous peritonitis in patient 2, we believe, was not related to AHD anastomosis. During a follow-up of 6 months to 4 years (medium 2 years), there was no dilatation of the intrahepatic bile duct or liver atrophy. These results are encouraging. Although the meticulous AHD reconstruction is a more demanding technique in laparoscopic operation, laparoscopic magnification would be helpful for the manipulation, and it is feasible in expert's experienced hands. Furthermore, we consider that laparoscopic AHD reconstruction should be recommended in the era of minimally invasive surgery.
Conclusion
Routine preoperative MRCP examination of CCs is recommended. It facilitates the detection of variations of the biliary tree. MRCP can provide a suspected diagnosis of an AHD in most patients with CC. When MRCP suggests a possible diagnosis of AHD draining into the cystic duct, it is better to dissect the anterior wall of the cystic duct to identify the AHD. An AHD draining into the cystic duct should be reconstructed, while duct ligation is not recommended. The orifice patch of AHD should be used as an effective way to enlarge the anastomosis. The laparoscopic approach is a feasible option in experienced hands.
Footnotes
Disclosure Statement
No competing financial interests exist.