
Abstract
Abstract
Objectives:
A small port could possibly minimize the collision of instruments and increase operability in laparoendoscopic single-site surgery (LESS) through the realization of small-triangle manipulation. In this study, we attempted to verify the small-port effect in an in vitro suture model and in vivo LESS hysterectomy with different-sized ports.
Subjects and Methods:
Two different-sized homemade glove ports were used and assessed in both in vitro and in vivo studies. The trocar head of port 1 was 36 mm in diameter and that of port 2 was 25 mm. Thirty sutures under LESS were conducted in a laparoscopic training box with each port. In LESS hysterectomy, 40 patients were recruited, of whom 20 underwent surgery under port 1 and the remaining 20 under port 2. One surgeon with experience in LESS conducted all sutures. The suture time of each stitch in the training box and for closing the vaginal cuff was videotaped and compared.
Results:
In the training model, the mean time for each suture with port 1 and port 2 was 18.6 ± 0.5 and 12.5 ± 0.3 seconds, respectively. In LESS hysterectomy, the mean suture time of the vaginal cuff with port 1 and port 2 was 15.2 ± 3.1 and 12.4 ± 2.6 minutes, respectively. Suture with port 2 was less time consuming than that with port 1 in both in vivo and in vitro studies, and the difference was statistically significant.
Conclusions:
A small port could save time in the suture process both in a training model and in operating room as a result of decrease in instrument collision and realization of small-triangle manipulation.
Introduction
Laparoendoscopic single-site surgery (LESS) is a minimally invasive surgery that has been used frequently because of the documented benefits of less postoperative pain, better esthetics, and shorter hospital stay as compared with multiport laparoscopy.1–3 LESS requires dedicated access port and equipment. Better and economical instrumentation and platform are the most important features in the widespread use of this technique. 4 However, most of the products on the market are either expensive or difficult to manipulate; this restricts the wide application of the surgery.
Surgeons in Korea designed a homemade glove port (HMGP), and its safety and efficacy have been clinically proven. 5 HMGP comprises a wound retractor, a surgical glove, and laparoscopic trocars. From our initial experience, we found that the enlarged head of the trocars would increase external interference and decrease operability in LESS, 6 whereas a smaller one may increase operation efficiency. To verify the “small-port” effect, that is, whether a small port could decrease the external collision between instruments and increase operability in LESS, we performed an in vitro experiment and an in vivo clinical study.
Subjects and Methods
The two ports
The ports in this study were two types of HMGP with two different-sized trocar heads, resulting in the different minimum distance between instruments after entering. Port 1 shown in Figure 1A uses big laparoscopic trocars (101Y; Hangzhou Kangji Medical Instruments Co., Hangzhou, China), in which the minimum distance between the instruments is 36 mm, whereas port 2 shown in Figure 1B uses smaller trocars (VTB05; Victor Medical Instruments Co., Changzhou, China) and the minimum distance between the instruments is 25 mm.
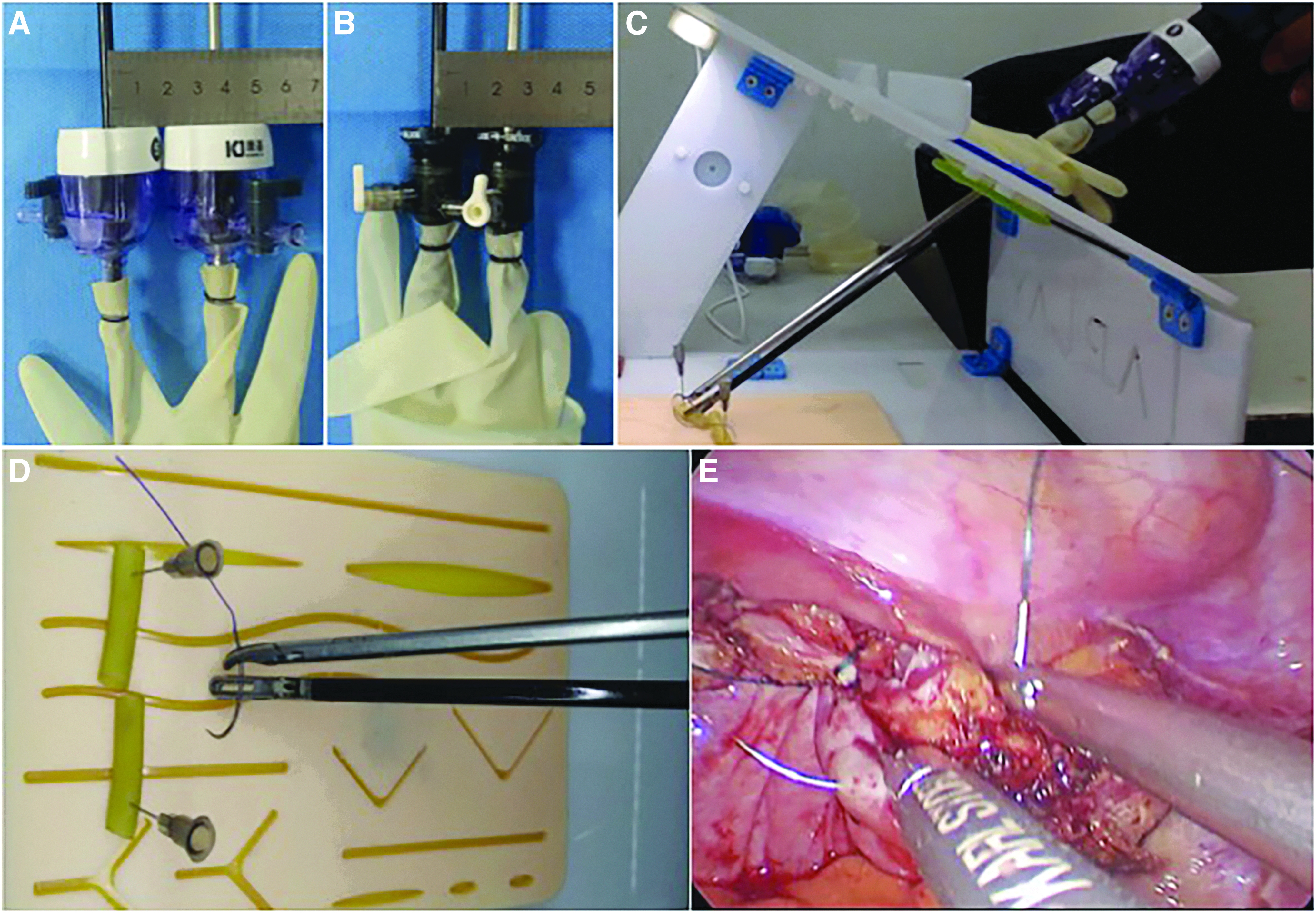
The small-port effect in LESS.
In vitro suture experiment
The suture box is a conventional laparoscopic training box with a 25-mm operating hole. The suture instruments included a laparoscopic needle holder and separating forceps, and Ethicon 2-0 VICRYL® suture (VCP345; Ethicon, Inc.) with a 4-cm tail. Both the needle holder and the forceps were inserted through the port and the operating hole. The procedure was to suture two segments of silicone tube together at one flexible end (Fig. 1C, D), and a total of 30 stitches with each port were done. The suture process was videotaped and the time for each suture was recorded.
In vivo experiment
Between December 2017 and November 2018, 40 cases planned for LESS hysterectomy were randomly assigned to two groups, with 20 patients in group 1 and 20 patients in group 2. Port 1 was used in group 1 and port 2 in group 2. V-Loc™ suture (2-0 VLOCL0315; Covidien™) was used in both groups for suturing the vaginal cuff (Fig. 1E). The surgery was videotaped and analyzed. All patients were followed up at 1 and 3 months after surgery. The primary outcome was the vaginal suture time, which referred to the period from the insertion of the V-Loc suture to the cut of the suture. The secondary outcomes included total operative time, estimated blood loss, complications, body temperature >38°C, and postoperative vaginal bleeding. Any abnormal findings by pelvic examination at follow-ups were recorded.
Both in vitro and in vivo suture procedures were conducted by one surgeon (Y.G.), who had experience of >100 LESSs at the start of the study. The ethics committee of Chongqing Medical University approved the in vivo study, and all patients provided a signed informed consent.
Statistical analysis
The values and variables were reported as mean ± standard deviation. The t-test was performed for the comparison of variables in Gaussian distribution, and chi-square test was used to evaluate the categorical variables. The differences and correlations were considered as statistically significant at P < .05. All the statistical analyses were carried out with the Statistical Package for Social Sciences software (SPSS Version 15.0, SPSS Inc. Chicago, Illinois).
Results
In the in vitro experiment, the time for one suture was 18.6 ± 0.5 seconds with port 1 and 12.5 ± 0.3 seconds with port 2. The difference was statistically significant with P < .05.
In the clinical study, as shown in Table 1, the age and body mass index were comparable between the two groups. The average suture time of the vaginal cuff with port 1 and port 2 was 15.2 ± 3.1 and 12.4 ± 2.6 minutes, respectively, and the difference was statistically significant. No conversion to laparotomy or additional site was needed in either group. The estimated blood loss, total operative time, perioperative complications, postoperative hospital stay, postoperative vaginal bleeding 3 months after surgery, and poor healing of vaginal cuff were comparable in both groups. Six patients (two from group 1 and four from group 2) experienced vaginal spotting after surgery, which stopped spontaneously. One patient from group 1 reported vaginal bleeding after intercourse 2 months postoperatively, and a 3-cm open wound was found at the vaginal cuff. She was treated with gauze compression and antibiotics. The vaginal cuff healed at 4-month follow-up.
Patient Characteristics and Perioperative Parameters
Discussion
LESS is a minimally invasive surgery that has attracted wide attention in the past decade. It requires dedicated equipment and ports, such as a special imaging system, a lengthened laparoscope, and flexible and curved instruments. To decrease the medical cost, HMGP was introduced and applied in clinical use. Lee et al. 5 first reported LESS hysterectomy with HMGP in 2009. Later, Jeon et al. 7 reported their initial experience with 50 patients by using HMGP. The authors concluded that HMGP was cost-effective, could provide adequate range of motion, and was flexible in port placement for LESS. Since then, the use of HMGP was reported in various surgeries and in different areas.2,8–10
The learning curve of LESS is much steeper than that of multiport laparoscopy, which restricts the wide application of LESS. You et al. 11 found that approximately 20 patients were needed to reach technical competency in LESS. Other researchers also indicated that LESS was more difficult to manipulate and the suture technique was the most difficult to handle. In this context, we assessed the suture performance of two different-sized ports in LESS; both in vitro and in vivo studies showed that the small port was associated with a shorter stitching time.
To explain the present result, we proposed the concept of “small-triangle” manipulation. In conventional multiport laparoscopy, each instrument enters the abdominal cavity from different sites, and an operation can be performed by forming triangulation between instruments, 12 namely the triangular manipulation (Fig. 2A). In LESS, as all instruments enter through a single incision, the operation mode has been tremendously transformed. Many studies proposed the “absence of triangulation” or “loss of working triangle.”2,13–17 Actually, the working triangle in LESS does not disappear; rather, it shrinks, which we call the “small triangle” because the angle is much smaller than that in multiport laparoscopy (Fig. 2B). The maintained triangulation between instruments is a key point that contributes to faster surgical procedures, which is applicable in both human and robotic LESS.2,18,19 In this study, small-triangle manipulation could be seen in both in vitro and in vivo experiments (Fig. 1D, E). In fact, the size of the trocar head has an impact on the formation of the small triangle. If the heads of the laparoscopic trocars are big, it would restrict the instruments from approaching, thus, on the one hand, increasing the external port collision and, on the other hand, forcing the instruments inside the abdominal cavity to cross; consequently, no triangulation could be formed (Fig. 2C). In contrast, a smaller trocar does not interfere with the proximity of instruments; this means less collision between ports, thus facilitating the realization of a “small triangle”; this results in enhanced operability with conventional straight instruments. This is the “smaller port” effect.
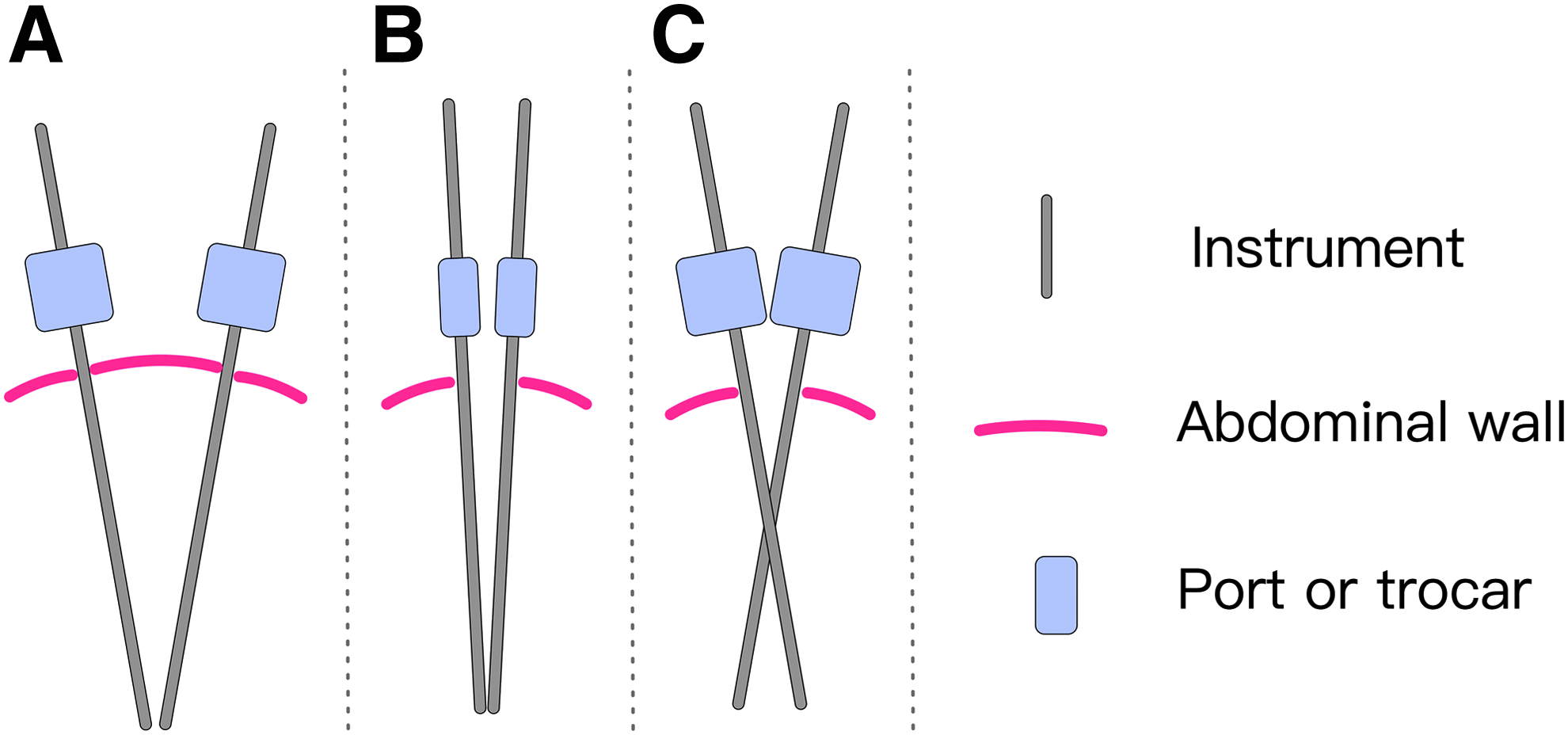
Different manipulations in multiport laparoscopy and LESS.
In this study, we attempted to investigate the effect of the port size on the suture procedure in LESS, the results of which should be interpreted with caution. A good port should meet several requirements such as airtightness, support to instruments, flexible, and easy to set up. In this study, we evaluated only the size of the trocar and avoided the other characteristics. Furthermore, we focused only on suture procedure, and there are other maneuvers in LESS such as resection and stripping, which may decrease the power of the study.
In conclusion, from the training model to the clinical LESS, we believe that a small port could save time in suture process in LESS because of the effect on the formation of “small-triangle” manipulation and decrease in instrument collisions. The small port effect, which we proposed, may provide an idea for future LESS port design.
Footnotes
Author's Contribution
Y.G. was in charge of surgery and article writing. F.Z. performed data collection and analysis. X.D. also did the data collection. J.T. had the conception and did article writing.
Disclosure Statement
No competing financial interests exist.