
Abstract
Abstract
Introduction:
Laparoscopic appendectomy is the gold standard for treatment of acute appendicitis. The single-incision laparoscopic surgery (SILS) approach has gained widespread acceptance. This study evaluates the learning curve of contemporarily trained surgeons adopting SILS appendectomy and, more specifically, the safety of the operation during the early phase of this learning curve.
Methods:
A retrospective review of 974 consecutive pediatric patients younger than 18 years of age, who underwent an appendectomy at a single institution from 2005 to 2018, was performed. Nonperforated and perforated appendicitis cases were included. A subgroup analysis was performed on SILS appendectomy. Outcomes measured included length of operating room and anesthesia time, as well as complication rate. A log-logistics and a Loess smoothing model were used.
Results:
A total of 438 single-incision laparoscopic appendectomies were reviewed. A trend toward faster operative times was observed for all surgeons as case numbers increased. The odds of still being operated on decreased by 0.997 for each additional case. Based on a 95% confidence band and this experienced time as the standard, we expect adopting surgeons to reach this experienced level after 51 cases. During the early SILS appendectomy learning curve, there was no significant difference in complication rate compared with multiport laparoscopy.
Conclusion:
As expected, the more single-incision cases were performed, the shorter the operative times. More importantly, there was no increase in complication rate during the learning stage of single-incision appendectomies in either perforated or nonperforated appendicitis.
Introduction
Acute appendicitis is one of the most common surgical emergencies in the pediatric population. 1 Though a few contemporary strategies have suggested nonoperative management, appendectomy, and more specifically laparoscopic appendectomy, remains the standard of care. 2 Less pain, shorter operative times, and improved cosmesis may be driving the push to move even more minimally invasive and potentially scarless options.
These potential advantages have helped single-incision laparoscopic surgery (SILS) gain widespread acceptance.2–5 With any new surgical technique, the adoption phase can potentially be challenging when learning the new skill. But how safe is the surgery during this learning phase? This study evaluates the learning curve of the SILS appendectomy in the pediatric population, but even more importantly, investigates the safety of this operation during the learning curve.
Methods
This study was reviewed and approved by the University of Illinois College of Medicine at Peoria Institutional Review Board (#00000688). After approval, a retrospective review was conducted of pediatric patients less than 18 years of age who underwent an appendectomy between January 2005 and April 2018 at the Children's Hospital of Illinois. Both acute and perforated appendicitis were included in our review. A subgroup analysis was then performed for the laparoscopic appendectomy approach of conventional versus single-incision laparoscopy, specifically the SILS approach utilizing a commercially available multiport trocar. Procedures performed by 17 board-certified pediatric surgeons were reviewed throughout the study period. To evaluate surgeon performance, parameters, including number of procedures, operative time, duration of anesthesia, conversion rate, as well as intra-operative and postoperative complications, were collected.
Statistical analysis
Statistical analysis was performed by using R version 3.5.1. Outcomes assessed were length of operation and whether the surgery resulted in a complication. Dependent variables of interest were case number and perforated appendicitis. The linear mixed-effects model was fitted to determine whether an association existed between either the number of cases a surgeon performed or having a perforated appendix and operation time, while accounting for the potential dependency in repeated measurements from the same surgeon. Due to the rareness of having a complication, logistic regressions were performed stratified by a surgeon to assess whether case number influenced having a complication. Estimation of the time it takes to reach a desired operation time was done by using the 95% confidence bounds of a Loess smoothing model. A Cochran-Mantel-Haenszel (CMH) exact test was used to assess the effect of having a perforated appendix on the likelihood of having a complication conditional on surgeons. A Pearson chi-squared test was used to evaluate the safety of performing SILS, specifically to assess whether there existed a difference in complications between SILS and non-SILS. Lastly, a Breslow-Day test was used to determine the effect of a perforated appendix on the likelihood of having a complication that was different for the two surgery methods.
Results
Data from 974 children who underwent laparoscopic appendectomy between 2005 and 2018 were initially collected. Patients were excluded if they had multiple procedures done under one anesthesia event, affecting the length of operation. Data were divided into patients who were operated on only using SILS and children who underwent conventional, multiport laparoscopy (non-SILS). Surgery characteristics are listed in Table 1.
Surgery Characteristics
Parentheses indicate proportion of surgical characteristics in relation to total number.
IQR, interquartile range; SILS, single-incision laparoscopic surgery.
Operating time
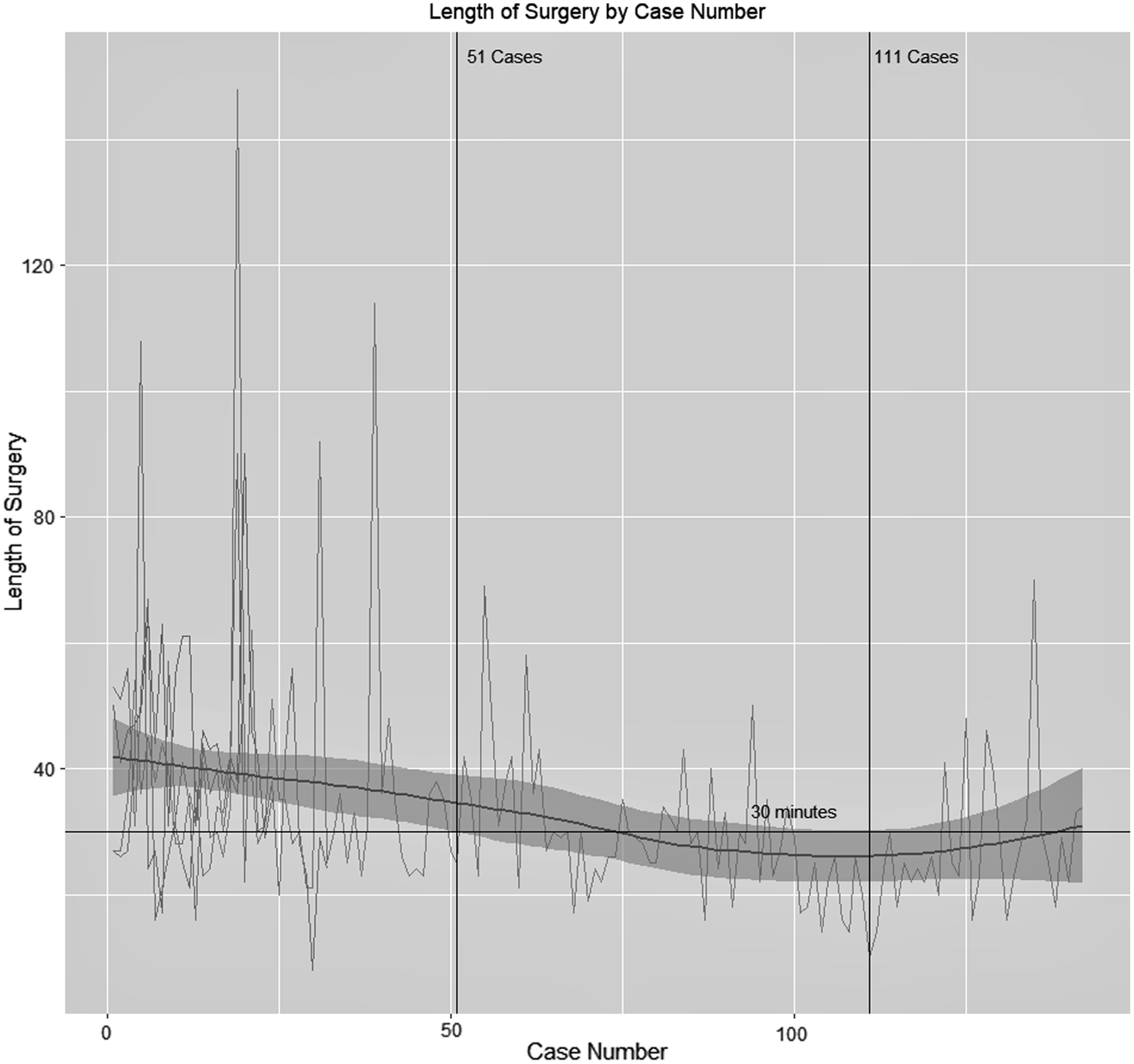
For the initial analysis, children were included if they were operated on by only using SILS technique. This technique was performed by 17 different surgeons, each having completed between 1 and 142 single-site appendectomies (Table 2). When evaluating the effect on length of operation, analysis was limited to the first 34 surgeries of surgeons who completed more than seven appendectomies. Specifically, after adjusting for having a perforated appendix, we would expect a decrease in the length of surgery of 0.16 minutes for every additional case performed (n = 187, t = −1.89, P = .0609, 95% confidence interval [CI] for the difference is −0.32 to −0.006 minutes lower), with the percent of variation attributed to differences in operation time among surgeons being roughly 12%. When looking at the trends for the individual surgeons, Surgeon A, with the most experience performing SILS (142 cases), had the most apparent decrease in operating time across cases. Treating this surgeon's performance as standard and using the 95% confidence band around a Loess smoothing estimate, we expect adopting surgeons to reach the standard median operation time of 30 minutes between 51 and 111 cases (Fig. 1).
Trend of operating time by surgeon.
Summary of Sample by Surgeon
Parentheses indicate number of cases with complication.
SILS, single-incision laparoscopic surgery.
Adverse outcomes
Since having a complication was a rare event and sample size was small, analysis to determine the effect of case number was limited to logistic regressions stratified on surgeons who had a greater frequency of complications (surgeons A, B, and C). This showed that there was not enough evidence to support an association between case number and having a complication. Thus, data do not support the hypothesis that surgeons have a decreased complication rate as they gain more experience with the single-incision laparoscopic technique.
As expected, after performing a CMH exact test stratified by surgeon without limiting the number of surgeries, it was found that having a perforated appendix increased the likelihood of having any complication after surgery. We would expect the odds of having a complication in SILS patients with a perforated appendix to be 5.03 times greater than in SILS patients with a nonperforated appendix (S = 302, P < .0001, 95% CI for odds of complication perforated versus nonperforated 2.38 to 10.66) (Fig. 2).
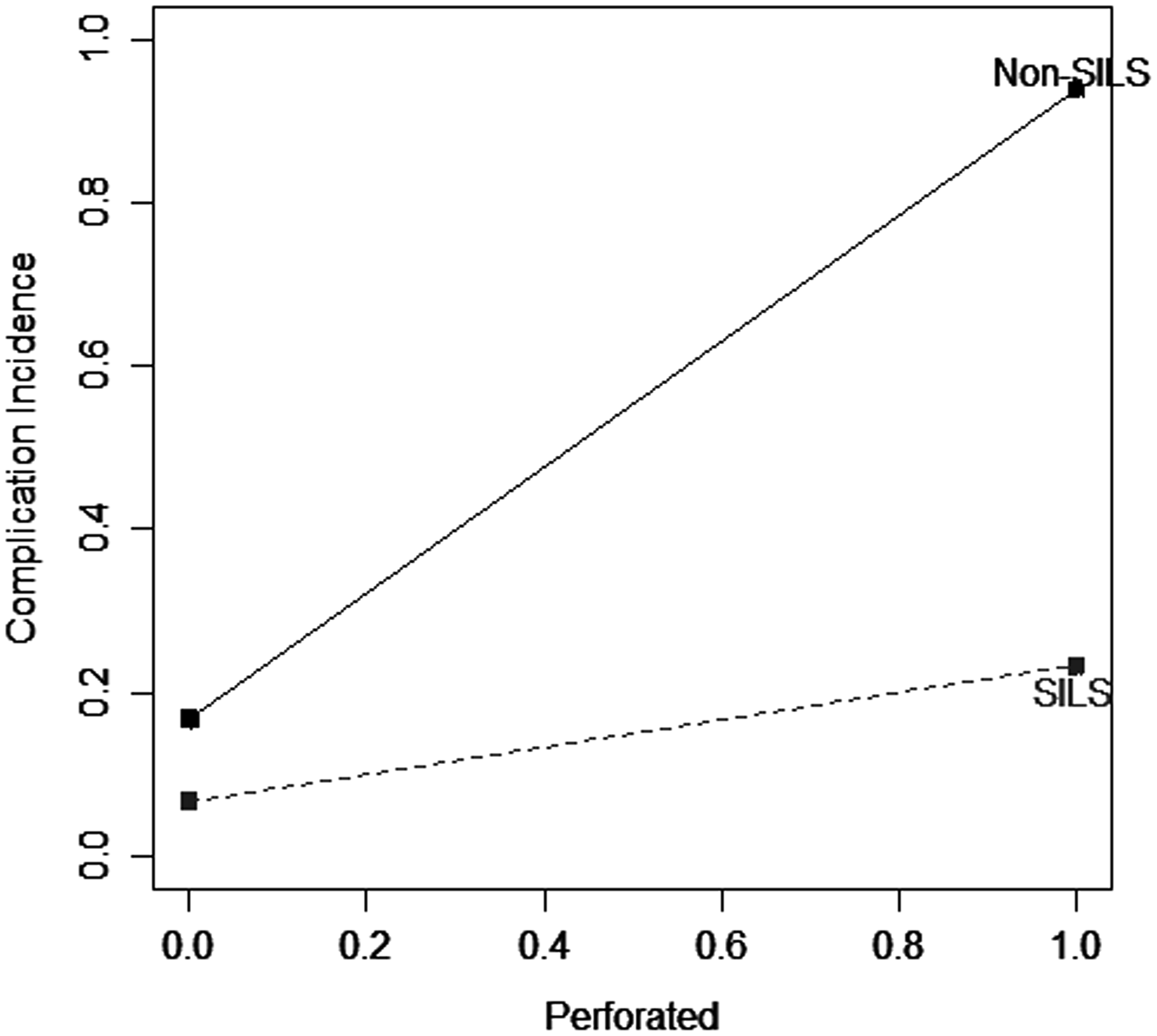
Complication incidence by condition of appendix and surgery technique. SILS, single-incision laparoscopic surgery.
Safety benefit of SILS versus non-SILS
We next considered cases where non-SILS were performed to determine the benefit of SILS in the way of patient safety. A chi-squared test showed a statistical difference in complications between SILS and non-SILS, with ∼30% of non-SILS patients having a complication and only 10% of SILS patients having a complication (odds ratio [OR] 0.28, χ 2 = 35.19, P < .0001, 95% CI for the OR 0.18 to 0.42) (Table 3). After performing a Breslow-Day test, it was found that the ORs comparing complications in perforated appendicitis verses nonperforated appendicitis were different in SILS and non-SILS (χ 2 = 15.91, P < .0001). We saw that the probability of having a complication was 94% in perforated non-SILS and just 20% in perforated SILS cases. These estimates ignore the dependency of observations taken by the same surgeon (Table 4).
Complications by Surgery Technique
Parentheses indicate proportion of surgical characteristics in relation to total number.
SILS, single-incision laparoscopic surgery.
Complications by Condition of Appendix and Surgery Technique
Parentheses indicate proportion of surgical characteristics in relation to total number.
SILS, single-incision laparoscopic surgery.
Discussion
Appendectomy continues to be the gold standard for treatment of acute appendicitis in children. 2 Despite the diagnosis remaining the same, the treatment technique continues to evolve. Traditional open approaches have been almost universally replaced by minimally invasive techniques.2–5 Currently, there is a push to become even less invasive than traditional laparoscopy. However, there have not been studies of the adoption of these techniques in relation to patient safety. Despite this, SILS is now well established with a wide variety of surgeries, from appendectomies to more complex colon resections.4,5 The proposed advantages tend to focus on cosmesis, less pain, and thus the potential for a shorter hospital stay. When adopting a new technique, a learning curve tends to exist. 6 Several studies have identified learning curves for SILS techniques that range anywhere from 5 to 75 cases.5,7–9 Others have shown the safety of an SILS approach when compared with traditional laparoscopy with similar complication rates.8,9 However, minimal literature exists on the safety of the procedure during the learning curve itself. We focused on the safety of SILS appendectomies during the learning curve in the pediatric population.
A learning curve can be identified as a longitudinal reduction and eventual plateauing of different components of a procedure. 7 But this does not just focus on operative time. Other components of an experienced level include complication rate and conversion rate. We believe that these are just as important when determining experienced level. In this study, more than 400 single-incision laparoscopic appendectomies at a single institution were reviewed. Similar to previous studies, a learning curve was identified. Specifically, to reach the level of the “experienced surgeon,” 51 cases needed to be performed. Our defined experienced level was based on a surgeon trained in the area of laparoscopy and SILS. As expected, the more single-incision cases were performed, the shorter the operative times. This trend toward faster operative times was observed in all our pediatric surgeons.
As previously mentioned, we also analyzed the safety of the procedure during these initial cases of an adopting surgeon. We determined that there was no correlation between number of cases and having a complication. These two factors are independent of one another, and, therefore, adopting SILS is a safe technique even during the learning curve phase. We further broke down the data isolating perforated and nonperforated appendicitis. As expected, there were increased complication rates in patients with perforated appendicitis. Yet, again, there was no difference in complication rate when comparing SILS with conventional laparoscopy in either scenario.
There are several limitations to our study. First, sample size for each newly adopting surgeon is small. Some are new, fellowship trained surgeons adopting SILS for the first time. We hope to continue to accrue data as their experience progresses. In addition, there are countless variations to the single-incision approach. Some use a commercially available trocar, whereas others place several trocars within one skin and fascial incision. Our study primarily focused on the SILS approach by using a proprietary multiport trocar. But, similar to Fransen et al., we too believe that SILS appendectomy is not a variation in technique, but rather a variation in approach. 10 Therefore, generalizing the safety during the SILS learning curve may still be applicable.
Finally, several studies have touched on the use of SILS training in residency. Joseph et al. reported that residents can be safely taught SILS techniques with minimal disruption in operating room efficiency. 11 In addition, Fransen et al. showed that a similar learning curve exists and is overcome with practice on the simple box trainers. 10 As we have shown the safety of adopting SILS during the learning curve in pediatric laparoscopic appendectomy, hopefully more surgery residency programs will be willing to incorporate single-incision training into their curriculum.
Footnotes
Acknowledgments
The authors are grateful to Sean Park, Ilakkiya Thangaivelan, and Lance Workman for their help in data collection.
Disclosure Statement
No competing financial interests exist.